
Abstract
Background:
The surge in electronic cigarettes and smokeless nicotine products has introduced an emerging concern. Although nicotine cessation is recommended to patients before surgery, existing guidelines are often based on evidence from combustible tobacco. No studies have evaluated how tobacco-free nicotine dependence (TFND) affects outcomes after mandibular fracture repair. The authors of the present study sought to examine whether TFND is associated with increased complications following open fixation of mandibular fracture.
Methods:
This was a retrospective cohort analysis of electronic medical records from multiple healthcare organizations. Patients who underwent open fixation for mandibular fracture were identified. Individuals with TFND, excluding those with cigarette or other tobacco product use, were compared to nicotine-free controls. Propensity score matching (1:1) accounted for demographics and comorbidities. Outcomes assessed within 1 year postoperatively included osteomyelitis, infected hardware, facial abscess formation, nonunion, periodontitis, dental caries, and onset of opioid use disorder. Adjusted risk ratios (RR) were calculated, with statistical significance set at P < .05.
Results:
Following propensity matching, each group had 2623 patients with similar characteristics. Patients with TFND had significantly higher risk of developing osteomyelitis (RR: 1.87, P < .001), infected hardware (RR: 1.46, P = .028), facial abscess formation (RR: 1.63, P = .001), nonunion (RR: 2.15, P = .001), and opioid use disorder (RR: 2.32, P = .009) compared to nicotine-free patients after mandibular fixation.
Conclusions:
Tobacco-free nicotine dependence significantly increases risk of infection and nonunion following mandibular fracture repair. As vaping and smokeless nicotine products become increasingly prevalent, perioperative screening and cessation counseling remain critical.
Keywords
Introduction
Electronic cigarettes and other non-combustible nicotine products (gums, patches, lozenges, and pouches) have become more prevalent over the past decade, particularly among young adults.1-3 Marketed as “safer” alternatives to cigarettes, these trending products have transformed nicotine accessibility yet remain physiologically harmful.4,5 Kopa-Stojak and Pawliczak demonstrated that e-cigarette aerosols contain measurable levels of free radicals and volatile organic compounds. 6 Wu et al showed that nicotine itself promotes vasoconstriction and platelet aggregation. 7 Within plastic surgery, Taub and Matarasso emphasized that the rising use of e-cigarettes warrants closer attention. 8 As these products become increasingly popular, surgeons are encountering patients who receive nicotine without tobacco, which raises concerns about whether current perioperative guidelines are up to date with this modern population.
The deleterious effects of cigarette smoking on wound healing, infection, and tissue perfusion are well established across surgical disciplines.9-11 Gruber et al and Ghanem et al further demonstrated that nicotine, independent of smoke exposure, may disrupt angiogenesis and osteoblast function, which are critical for bone healing.12,13 Clinical studies have also associated tobacco-free nicotine dependence (TFND) with increased risk of postoperative prosthetic infection and sepsis after shoulder, spine, and joint procedures.14-16 However, to the authors’ knowledge, no studies have evaluated the impact of TFND in facial trauma.
Mandibular fractures represent a substantial proportion of reported maxillofacial injuries and commonly affect young men with risk factors, such as smoking or substance use.17,18 Active smoking has been identified as an independent predictor of infection, nonunion, and hardware displacement following mandibular repair.19-21 However, whether tobacco-free nicotine confers similar risk of complications remains unknown. The authors of the present study sought to determine whether TFND is associated with adverse outcomes after open fixation of mandibular fracture.
Methodology
Data Source
Data was extracted from the TriNetX database (TriNetX, LLC, Cambridge, MA), a federated research network that compiles de-identified electronic health records (EHRs) from healthcare centers and institutions. Data query was performed on November 1, 2025, through the Research Network, which aggregates EHRs from 106 participating healthcare organizations and encompasses over 120 million unique individuals. All collected data within TriNetX are de-identified and compliant with the Health Insurance Portability and Accountability Act. Institutional Review Board approval was therefore exempted for this analysis. The present study adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cohort studies to ensure clarity, transparency, and methodological rigor (Supplemental Table 1). 22
Patient Selection
Patients aged 18 years or older who underwent open fixation for mandibular fracture between October 2015 and November 2025 were identified using Current Procedural Terminology (CPT) codes 21462 and 21470. CPT 21462 represents open reduction of mandibular fracture with interdental (maxillomandibular) fixation, whereas CPT 21470 denotes open treatment of complicated mandibular fracture by multiple surgical approaches, including internal fixation, interdental fixation, and/or wiring of dentures or splints. CPT 21461, which describes open treatment without interdental fixation and does not specify fixation-based management, was not included. The study population was then stratified into 2 groups: individuals with documented tobacco-free nicotine dependence (excluding those with any tobacco or cigarette use) and nicotine-free controls. This was done with International Classification of Diseases, 10th Revision (ICD-10) codes: F17 for nicotine dependence as well as exclusion of F17.21, F17.22, and F17.29 for tobacco or cigarette products. Tobacco-free nicotine products are defined as electronic cigarettes, gum, pouches, and lozenges.
Outcomes
Postoperative complications were evaluated within 1 year of surgery. Outcomes were osteomyelitis, infected hardware, facial abscess formation, nonunion, periodontitis, dental caries, and onset opioid use disorder. These events were determined by the ICD-10 codes in Supplemental Table 2.
Statistical Analysis
Data analysis was performed using the TriNetX Analytics Platform, which employs proprietary computations built on JAVA, R, and Python. Continuous variables were expressed as means with standard deviations and compared using independent-samples t-tests when data were approximately normally distributed; nonparametric tests were applied when normality assumptions were not met. Categorical variables were summarized as frequencies and percentages, with comparisons using either chi-square or Fisher’s exact tests, as appropriate.
Propensity Score Matching
To reduce confounding, 1:1 propensity score matching was conducted using multivariable logistic regression. Covariates included demographic factors (age, sex, race, ethnicity, and body mass index [BMI]); socioeconomic indicators (educational attainment, employment instability, occupational hazards, limited access to basic resources, housing insecurity, adverse psychosocial environments, and early-life challenges); and medical comorbidities (diabetes, hypertension, cerebrovascular disease, congestive heart failure, hypothyroidism, chronic obstructive pulmonary disease [COPD], alcohol use disorder, chronic kidney and liver disease, and obesity). Demographic and comorbidity distributions before and after matching are summarized in Tables 1 and 2, respectively. The CPT codes 21462 and 21470 were also included in the matching model to minimize procedural heterogeneity and variations in fracture severity. Covariate balance between matched groups was confirmed when p-values exceeded 0.05. Although standardized mean differences (SMDs) are not natively available within TriNetX, this criterion corresponds to the conventionally accepted threshold of SMD < 0.1 for adequate covariate balance. The study’s design is illustrated in Figure 1. Postoperative outcomes were compared between matched groups using adjusted risk ratios (RR) with 95% confidence intervals (CIs). Statistical significance was defined a priori as P < .05.
Propensity Score Matching: Demographics.
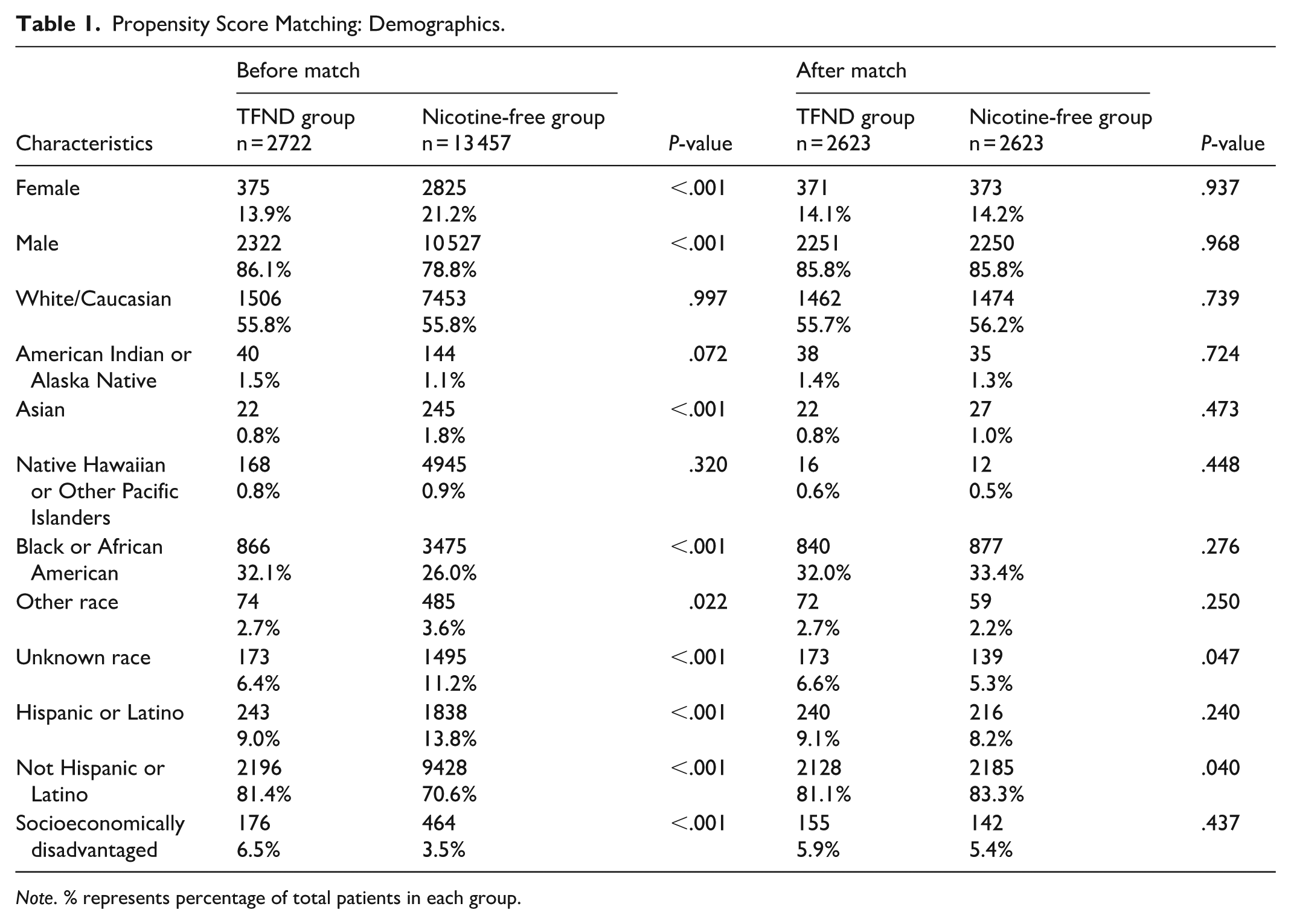
Note. % represents percentage of total patients in each group.
Propensity Score Matching: Comorbidities and CPT Codes.
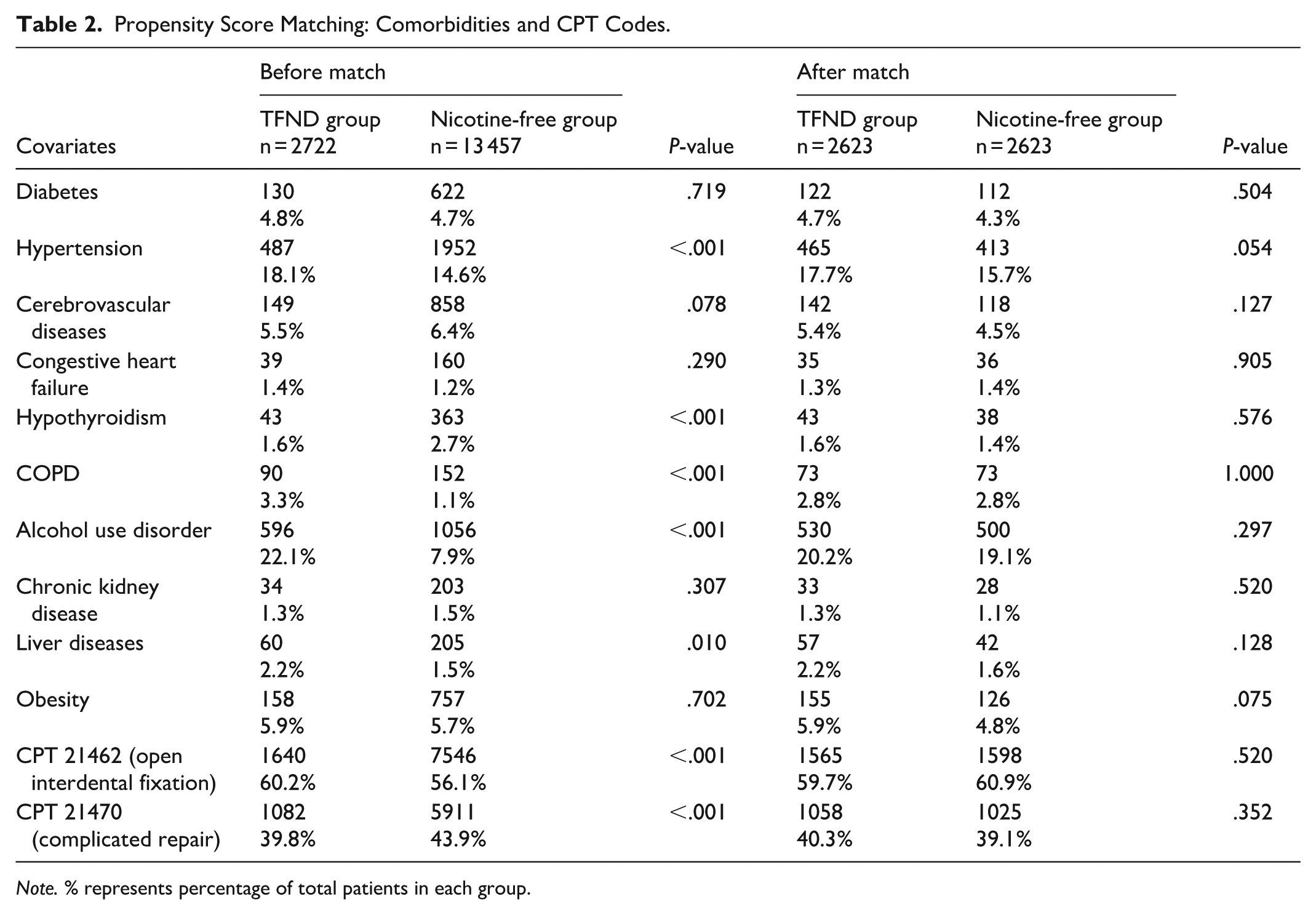
Note. % represents percentage of total patients in each group.
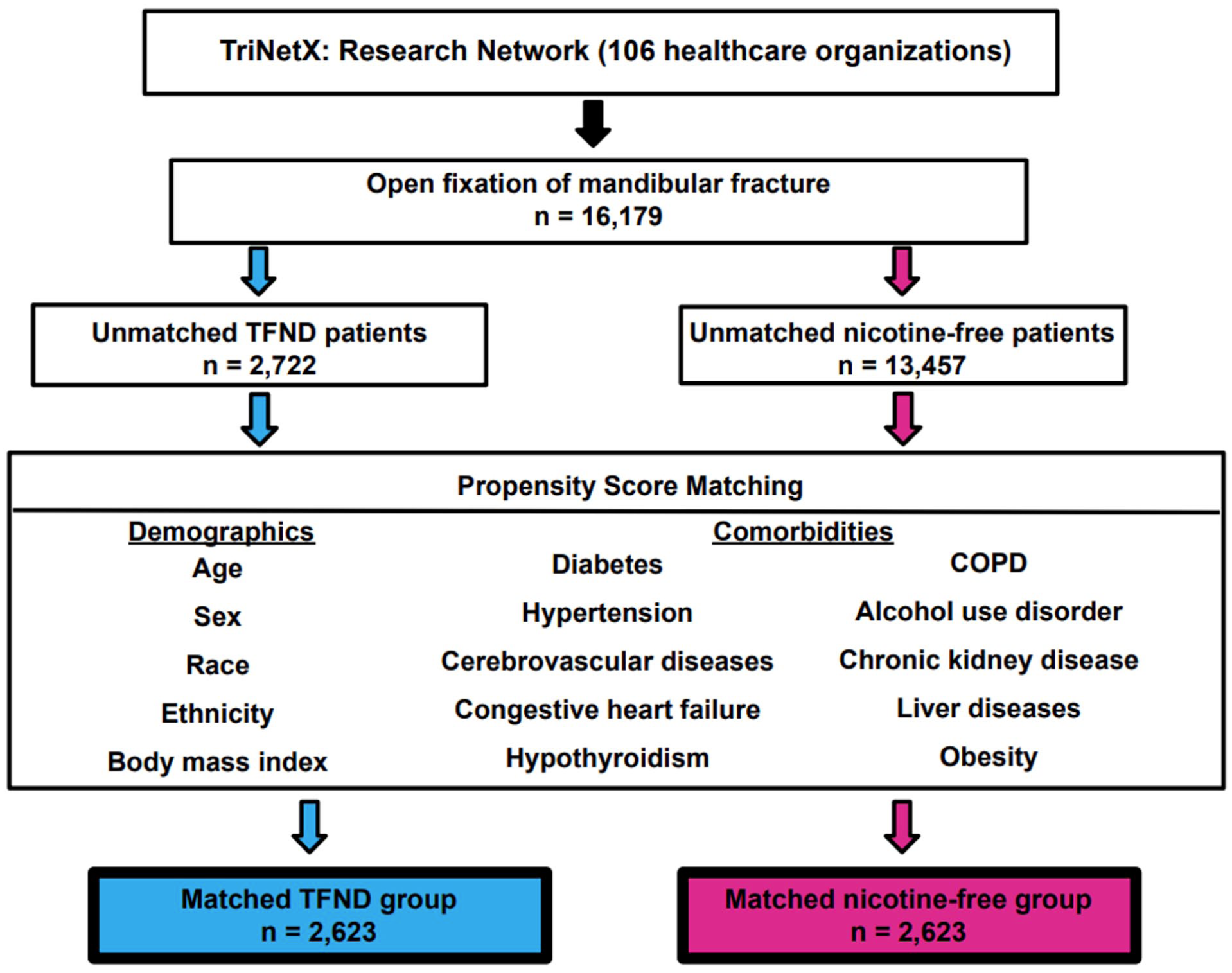
Flowchart outlines the study design.
Results
An initial total of 16 179 patients underwent open fixation of mandibular fracture, with 2722 unmatched patients with TFND and 13 457 unmatched nicotine-free patients. Following 1:1 matched analysis, each group had 2623 patients. The overall age ranged from 18 to 90 years, with a mean of 34.6 ± 12.9 years in the TFND group and 33.8 ± 15.5 years in the nicotine-free group. The TFND group had a mean BMI of 25.1 ± 5.2 kg/m2 compared to 25.6 ± 5.3 kg/m2 in the nicotine-free group. Both matched cohorts were predominantly male, comprising more than 80% of each group. Most patients in both groups underwent open interdental (maxillomandibular) fixation (CPT 21462), while a smaller proportion required more extensive repair (CPT 21470). Within 1 year following fixation, patients in the matched TFND group had significantly higher postoperative risk of developing osteomyelitis (4.5% vs 2.4%, RR: 1.87, 95% CI: 1.38-2.54, P < .001), infected hardware (3.1% vs 2.1%, RR: 1.46, 95% CI: 1.04-2.05, P = .028), facial abscess formation (4.2% vs 2.6%, RR: 1.63, 95% CI: 1.21-2.20, P = .001), nonunion (2.2% vs 1.0%, RR: 2.15, 95% CI: 1.37-3.38, P = .001), and onset of opioid use disorder (1.2% vs 0.5%, RR: 2.32, 95% CI: 1.21-4.44, P = .009) compared to the matched nicotine-free group. No significant differences were observed for periodontitis (1.1% vs 0.9%, RR: 1.22, 95% CI: 0.71-2.08, P = .474) and dental caries (5.8% vs 6.2%, RR: 0.93, 95% CI: 0.74-1.18, P = .556) (Table 3).
Outcomes.
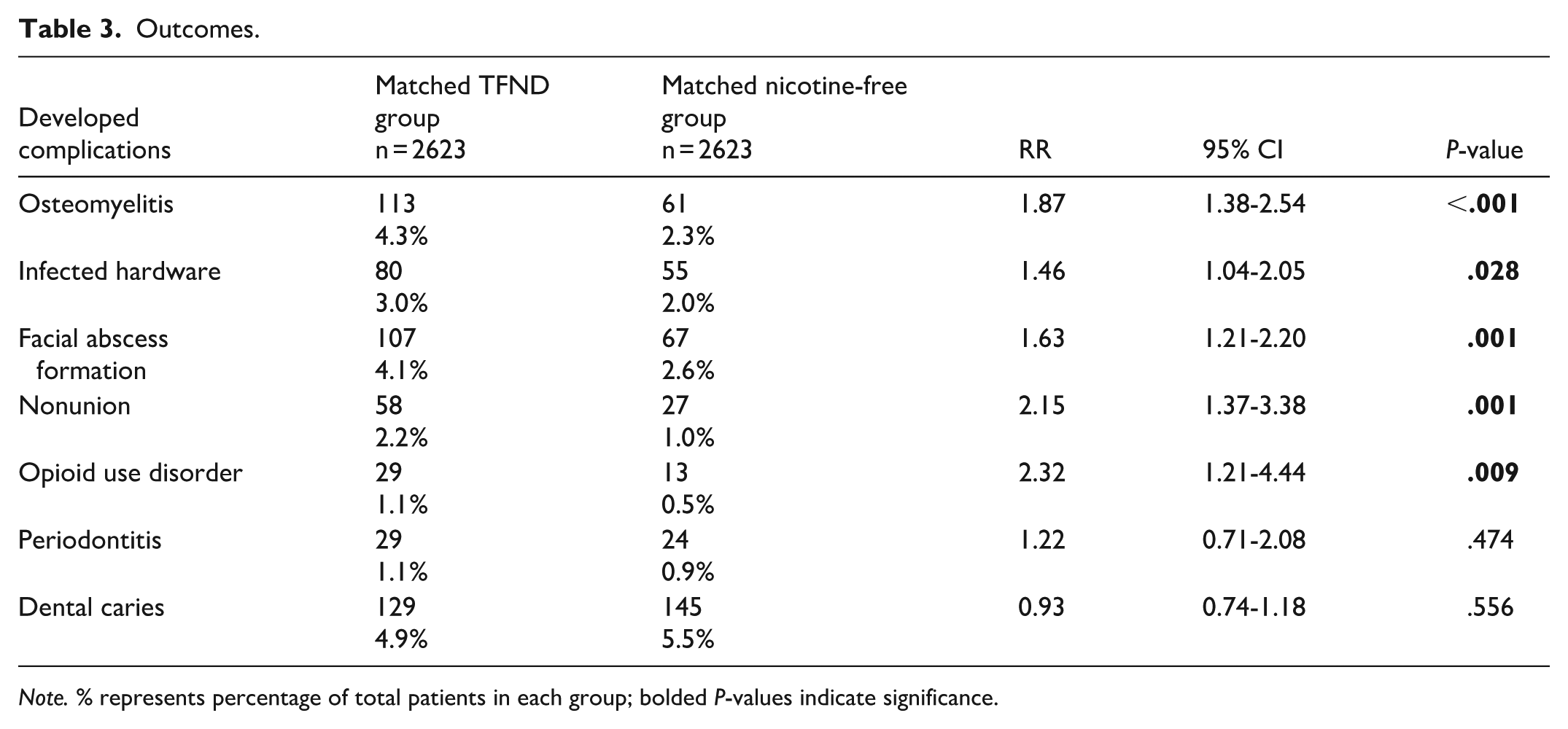
Note. % represents percentage of total patients in each group; bolded P-values indicate significance.
Discussion
The present study represents the first large, multi-institutional analysis of more than 5000 patients to assess the impact of tobacco-free nicotine dependence on open fixation of mandibular fracture. Patients with TFND had significantly increased risk of developing osteomyelitis, hardware infection, facial abscess formation, nonunion, and development of opioid use disorder within 1 year postoperatively, whereas risks of periodontitis and dental caries did not significantly differ from nicotine-free patients.
TFND patients experienced a notably higher risk of osteomyelitis, hardware infection, and facial abscess formation. Similar associations between tobacco-free nicotine and postoperative infection have been reported in procedures involving hardware implantation.14-16 Nicotine potentiates platelet activation and thromboxane-mediated vasoconstriction, which can restrict capillary perfusion and oxygen delivery in healing tissue.7,23,24 Reduced oxygen in turn may impair neutrophil oxidative burst and macrophage function, attenuating bacterial clearance following fixation.25,26 Experimental models further demonstrate that nicotine suppresses fibroblast migration, collagen synthesis, and capillary regrowth in gingival tissue.27-29 Thus, the physiological disturbances could compromise angiogenesis and antibiotic treatment along fixation interfaces. Within the mandible, where cortical vascularity is already limited, this may heighten susceptibility to bacterial biofilm formation on implanted hardware and delay osseous integration. 25 Ma et al demonstrated that nicotine directly suppresses osteogenesis in rabbit mandibular bone, corroborating its inhibitory influence on osteoblastic activity and mineral deposition. 30 In human osseous tissue, both persistent hypoxia as well as limited bone remodeling from nicotine usage could facilitate bacterial adherence within the microstructural irregularities and progression to osteomyelitis. 31 Similarly, TFND patients may have delayed mucosal healing and compromised epithelial barrier integrity, which could predispose them to infected abscess formation around fixation sites. 32 Although most existing evidence pertains to cigarette smoke, emerging studies on nicotine and e-cigarette aerosols have demonstrated impaired oral epithelial regeneration, oxidative injury, and microbial dysbiosis, suggesting comparable mucosal vulnerability in tobacco-free nicotine users.33-35 Further investigation should aim to delineate how these emerging delivery methods influence epithelial regeneration and microbial flora within the oral cavity. In the interim, patients with TFND should be managed with the same perioperative vigilance as traditional smokers, including cessation counseling and prompt evaluation for potential infection.
TFND patients also had a significantly higher rate of nonunion following mandibular fixation. Bone healing relies on coordinated activity of osteoblast and osteoclast, which require adequate vascular supply and proper inflammatory signaling. 36 Nicotine may uncouple this process by disrupting the balance between osteoblastic and osteoclastic activity, which could impair extracellular matrix maturation and mineral deposition. 13 Consequently, these dysregulations may lead to disorganized bone formation and delayed structural consolidation. 37 In addition, nicotine-induced vasoconstriction may restrict perfusion and oxygen delivery at the fracture site, further hindering osseous integration and destabilizing fixation. 38 Although our study establishes only a correlative association, these findings suggest that TFND patients could experience delayed union and underscores the need for mechanistic studies to clarify the impact of tobacco-free nicotine on bone metabolism. Clinically, surgeons should anticipate the risk of prolonged recovery trajectories and consider nutritional optimization for patients who are unable or unwilling to discontinue these nicotine products.
TFND patients also demonstrated a significantly higher rate of being diagnosed with opioid use disorder in the postoperative period. This relationship likely reflects overlapping neurobiological and behavioral mechanisms that link nicotine dependency to heightened vulnerability for opioid dependence. 39 Both nicotine and opioids activate dopaminergic transmission within the mesolimbic reward circuitry, facilitating reinforcement and compulsive drug-seeking behaviors through shared neuroadaptive changes. 40 Nicotine has been shown to upregulate μ-opioid receptor expression and potentiate dopamine release in preclinical models, thereby enhancing the rewarding properties of opioids. 41 Cross-sensitization between the 2 substances may also accelerate tolerance development, leading to escalating opioid requirements for analgesia and greater risk of dependency after surgery. 42 Beyond these neurochemical effects, nicotine use itself may signal a broader behavioral predisposition toward substance reinforcement and maladaptive coping in response to perioperative stressors. 43 The observed association calls for integrated perioperative management of nicotine-dependent patients. Vigilant prescribing practices and postoperative monitoring of analgesic use in in this high-risk population may mitigate the risk of developing opioid use disorder. Future studies are warranted to delineate how tobacco-free nicotine modulates opioid addiction and to determine whether therapeutic interventions can mitigate this risk.
While nicotine cessation has long been a part of perioperative counseling, current recommendations were largely derived from studies on combustible tobacco use. The present findings therefore expand this evidence base to include “modern” nicotine products, demonstrating that tobacco-free nicotine dependence is associated with increased risk of postoperative infection, nonunion, and opioid use disorder. Tobacco-free nicotine products may be associated with physiological changes involving tissue perfusion, bone formation, and recovery that could contribute to adverse postoperative outcomes. Rather than altering standard practice, this study reinforces a surgical guideline to parallel a generation of patients who may not identify as “smokers” yet remain physiologically vulnerable to nicotine’s vasoconstrictive and osteoinhibitory effects. Incorporating explicit screening for all nicotine products into preoperative risk assessment frameworks would align clinical decision-making with current epidemiologic trends and ensure counseling remains evidence-based amid the shifting nicotine landscape.
While the TriNetX network provided a robust sample size and improved external validity, several limitations must be acknowledged. TriNetX is a retrospective database and, by design, is unable to determine a causal relationship. While propensity score matching improved cohort comparability, unmeasured confounders, such as degree of mandibular displacement, fracture pattern, and timing of intervention, may still have influenced outcomes. As such, the CPT codes (21470 and 21462) approximate the operative scope but do not specify anatomic fracture subsite (eg, condylar, angle, symphyseal, or parasymphyseal). Furthermore, variability in prophylaxis protocols, surgeon experience, and institutional policies could further contribute to differences in complication risks. For instance, although opioid use disorder was assessed as a new-onset diagnosis following surgery, undocumented opioid exposure histories, perioperative prescribing variability, and unaccounted underlying behavioral predispositions toward substance dependence may have influenced this outcome as well. A prospective single-institution study with standardized operative techniques and perioperative protocols will enhance internal validity. Finally, this study did not compare different types of tobacco-free nicotine products (electronic cigarettes vs gum vs pouches) or include a combustible tobacco cohort for direct comparison. While the present design intentionally isolated tobacco-free nicotine dependence, TriNetX does not provide serum concentration of nicotine or cotinine levels, duration of use, or frequency of consumption. Consequently, dose-dependent relationships and differences between tobacco-free and tobacco-based nicotine products could not be evaluated. Additionally, because nicotine dependence coding within administrative databases may incompletely distinguish combustible from noncombustible nicotine sources, some degree of exposure misclassification remains possible despite exclusion of tobacco-specific ICD-10 codes. Future studies comparing nicotine delivery methods and exposure intensity may better clarify how nicotine concentration and route of administration influence postoperative risk. Furthermore, time-to-event analyses may provide additional insight into the temporal onset and progression of postoperative complications following mandibular fixation. Despite these limitations, this study’s multi-institutional design and propensity score matching bolster external validity. The present analysis provides the first large-scale evidence isolating the effects of nontobacco nicotine on postoperative maxillofacial outcomes. Our findings may help inform perioperative counseling considerations regarding these increasingly popular alternative nicotine products. Nicotine exposure, irrespective of delivery method, may represent a clinically relevant and modifiable perioperative risk factor. However, as tobacco-free nicotine products continue to increase in global prevalence, more insightful and mechanistic research is needed. 44
Conclusion
Tobacco-free nicotine dependence was associated with increased postoperative infection and nonunion risk following open fixation of mandibular fracture. The present study reinforces the necessity of screening and cessation counseling for patients who use tobacco-free nicotine products, including e-cigarettes, gums, or patches. Careful perioperative monitoring for these emerging products may improve outcomes following mandibular repair.
Supplemental Material
sj-docx-1-fac-10.1177_27325016261461290 – Supplemental material for Tobacco-Free Nicotine Increases Risk of Infection and Nonunion Following Open Fixation of Mandibular Fracture
Supplemental material, sj-docx-1-fac-10.1177_27325016261461290 for Tobacco-Free Nicotine Increases Risk of Infection and Nonunion Following Open Fixation of Mandibular Fracture by Matthew Q. Dao, Emma M. Lascar, Sheuli Chowdhury, Perri S. Vingan, Jasmin Wilson, Nissim Hazkour, Sabrina Shih, Eloise W. Stanton, Peter W. Henderson and Peter J. Taub in FACE
Supplemental Material
sj-docx-2-fac-10.1177_27325016261461290 – Supplemental material for Tobacco-Free Nicotine Increases Risk of Infection and Nonunion Following Open Fixation of Mandibular Fracture
Supplemental material, sj-docx-2-fac-10.1177_27325016261461290 for Tobacco-Free Nicotine Increases Risk of Infection and Nonunion Following Open Fixation of Mandibular Fracture by Matthew Q. Dao, Emma M. Lascar, Sheuli Chowdhury, Perri S. Vingan, Jasmin Wilson, Nissim Hazkour, Sabrina Shih, Eloise W. Stanton, Peter W. Henderson and Peter J. Taub in FACE
Footnotes
Ethical Considerations
This study analyzed de-identified data from the TriNetX database and does not require institutional review board approval.
Consent to Participate
This study utilized de-identified data obtained from the TriNetX Research Network. As no identifiable patient information was accessed, informed consent was waived and not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Peter J. Taub is a member of the Editorial Board of FACE and did not take part in the peer review or decision making process for this submission.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.