
Abstract
Background
Expansion of paramedic roles in the community could reduce non-urgent emergency department (ED) attendances. In Ireland a knowledge gap exists regarding the development of alternative care pathways that avoid ED conveyance. The aim of this research was to explore inter-rater agreement amongst advanced paramedics (AP) about the ‘appropriateness’ of attendances to the ED in Ireland utilising data from the Better Data, Better Planning (BDBP) Study.
Methods
The BDBP study was a multi-centre study investigating factors influencing ED utilisation in Ireland. For this secondary data analysis, a chart review was conducted and adult patient summary files (n = 306) were assessed for measures of appropriateness by a national panel of six AP, including whether each presentation was considered an inappropriate use of ED resources and potentially could be managed by a General Practitioner (GP) within 24–48 h. A subset analysis compared outcomes for patients transported by ambulance with those that were transported to the ED by other means.
Results
The AP panellists determined that between 12% to 73% of ED attendances were considered an inappropriate use of ED resources (Inter-rater Agreement 19%, κ = 0.182, p < .001) and that between 12% to 79% of cases were suitable for management by a GP within 24–48 h (Inter-rater Agreement 11%, κ = 0.120, p < .001). Inter-rater agreement was higher for patients transported by ambulance who tended to be older (p < .001), live alone (p ≤ .01), have higher triage scores (p ≤ .01), and be admitted to hospital (p ≤ .01).
Conclusions
APs did not reach agreement on what constitutes an ‘inappropriate’ attendance to the ED. The reasons for this are multifactorial but it highlights the complexities in developing alternative care pathways for ED avoidance in the community setting. The potential for development of alternative care pathways in Ireland is significant but requires appropriate supervision and governance to support decision-making for paramedic roles with an expanded scope of practice.
Introduction
Internationally the demand for unscheduled care has increased across healthcare systems and emergency department (ED) crowding is becoming a global public health crisis. 1 In Ireland there were 1.7 million ED presentations in 2023, and statutory ambulance services responded to over half a million emergency calls nationally.2,3 This increased demand for emergency care has long surpassed capacity and crowding in Irish EDs is now endemic. 4 ED crowding is associated with negative patient outcomes including delayed treatment and poor quality care, which can impact morbidity and mortality. 5
In Ireland, the Sláintecare Action Plan represents cross-party political consensus on the future of health and social care services in Ireland that is unique in the history of the State. 6 It aims to shift the majority of care from the acute to the community setting and improve population health by delivering the ‘right care, in the right place, at the right time, by the right team’. The international literature suggests that 30–80% of ED attendances could be treated appropriately in non-emergency settings. 7 Irish data from a recent census study investigating demographic and clinical factors influencing ED crowding across regional hospitals, the Better Data, Better Planning (BDBP) Study 8 suggests that this figure ranges from 11% to 73% nationally. 9 Additionally, over half of the calls (52%) responded to by the National Ambulance Service (NAS) in 2023 were not triaged as life-threatening, ranging from serious injury calls to minor illness. 3 Internationally many jurisdictions have acted to address these issues through the use of ‘Treat and Refer’ and alternative care pathways; (i.e. treating patients elsewhere without transporting them to the ED). The introduction of Treat and Refer in the United Kingdom was associated with a 32% reduction in ambulance service conveyance rates. 10 In Ireland, the development of alternative care pathways and Treat and Refer protocols are in the early stages of implementation.
The scope and education of paramedics has changed over time, with a shift from emergency service workers facilitating timely transport to definitive care, to expert clinicians who are integrated within the broader healthcare system. 11 Past research on the interface of care between paramedics and the ED in Ireland has been limited although a previous study by the authors did report concordance rates between advanced paramedic (AP) admission prediction and hospital admission records was strong at 70%. 12 A report by the national Health Information and Quality Authority in 2014 recommended implementation of a Treat and Refer model of care enabling access to alternative care pathways. 13 A survey of Irish Paramedics and Emergency Medicine Consultants conducted in 2020 reported that up to 87% of participants agreed that Treat and Refer will reduce unnecessary ambulance journeys. 14 However, until recently non-conveyance of patients was not generally an option for paramedics in Ireland unless the patient explicitly refused to travel. 15 Under this traditional model of care, increased call volumes for emergency ambulances translate into an ever-increasing number of patients being transported to the ED for treatment which is unsustainable.
In Ireland, the NAS aims to transform from a service that has traditionally transported all patients for hospital treatment, to a clinically led service treating more patients over the phone, on scene or at home. 16 The Community Paramedic 17 is an example of a relatively new role with an extended scope of practice and potential for the development of other alternative care pathways. Another example is the Pathfinder model which is an interprofessional service designed to safely keep older people in their homes as an alternative to ED attendance. 18
Sustainable integration of health services in the Irish out-of-hospital setting could reduce avoidable ED attendances nationally. However, research to date has been limited and a significant knowledge gap exists in relation to the potential for development and expansion of paramedic services. The aim of this research was to explore inter-rater agreement between APs about the ‘appropriateness’ of attendances to the ED in Ireland utilising data from the BDBP Study.
Methods
Study context
In the Irish setting General Practice (GP) is typically the first point of contact for patients with a health issue and are responsible for referrals to emergency or specialist treatment when required. There are a range of public and private services for patients requiring access to urgent and emergency care, including; GPs, EDs, urgent care centres, acute medical units, minor injury units, pharmacies and statutory ambulance services. 19 EDs operate on a 24/7 basis and out-of-hours GP services and pharmacies operate evening and weekend services. Public Injury Units and private Urgent Care Clinics operate extended daytime hours (8 a.m.–8 p.m.) and provide care for minor injuries and illness. Acute Medical Units are generally accessed by referral. In addition to unscheduled/emergency care, Ireland's public hospitals provide maternity services, inpatient and outpatient care services, including advanced diagnostics. 20
The Pre-hospital Emergency Care Council (PHECC) is the statutory regulator for paramedicine in Ireland and maintains the register of practitioners which includes Emergency Medical Technicians, Paramedics, APs and Specialist Paramedics. 15 Traditionally practitioners undertook vocational training but in the past 10 years there has been a transition to third-level education nationally with paramedics now undertaking a BSc programme and APs being educated to MSc level. Specialist Paramedics are a new role nationally also requiring an MSc with specialist training to practice as a Community Paramedic or Critical Care Paramedic. 17 The National Ambulance Service (NAS) and Dublin Fire Brigade provide a statutory ambulance response, supported by auxiliary, private and voluntary services. According to Irish clinical practice guidelines, paramedics are obliged to transport most patients who call for an ambulance to the ED, unless the patient explicitly refuses transport. 15 There are some exceptions, within specific roles which allow Treat and Refer, and recent years have seen the development of some alternative care pathways, aligned with international best practice.
Design
The BDBP Study was a multi-centre, cross-sectional study across urban, rural and mixed EDs (n = 5) in Ireland. The full methodology has previously been described. 8 The secondary data analysis applied here constitutes a retrospective chart review.
Setting
Following ethics approval, data were collected at five ED sites over separate 24 h periods during the course of 2020 to account for diurnal and seasonal variation in attendance patterns. Participating hospitals were; Midlands Regional Hospital Tullamore, University Hospital Limerick, St Vincents University Hospital, St James University Hospital and University Hospital Kerry with the 24 h census data being collected at each site from Thursday at 12 p.m. to Friday at 12 p.m.
Participants and procedure
All adult patients presenting to the ED at participating sites over a 24 h census period were eligible for inclusion in the BDBP Study. The inclusion criteria applied in the BDBP Study were (A) Adult aged ≥18 years (B) Manchester Triage System categories 2–5 and medically stable in relation to temperature, heart rate, respiratory rate, blood pressure, mental status and oxygenation (C) Patient has capacity and willingness to provide informed consent. Exclusion criteria included (A) Scheduled admissions to the ED, (B) Mental Health presentations, (C) Patients with altered capacity due to drug or alcohol intoxication, and (D) Inability to communicate sufficiently in English to participate. For these patients, clinical data were collected via electronic records and a questionnaire provided information on demographics, healthcare utilisation, service awareness and factors influencing the decision to attend the ED.
AP chart review
Following on from initial BDBP data collection, a Research Nurse performed a follow-up site visit to each ED to conduct a chart review for participants. Data were extracted from electronic patient records and an anonymised patient summary file was compiled (Supplemental File S1) which included the following information; demographics, source of referral, current medications, social history, presenting complaint, duration of presenting complaint, Manchester triage category, vital signs at triage, patient's level of self-reported pain and anxiety, investigations (e.g. blood sample, electrocardiogram; ECG, diagnostic imaging, etc.), interventions (e.g. airway, suturing, splint, etc.), medication administered (e.g. analgesic, fluids, antibiotic, etc.) and referrals.
Patient Summary Files were assessed independently by a panel comprised of n = 6 APs in a retrospective chart review. The anonymised patient summary files were the sole unit of analysis for the AP review panel and the participating clinicians did not examine the data from the patient questionnaires. The number of panellists selected was based on precedent from previously published work examining inter-rater agreement on ED attendance. 21 APs were selected for the review panel as the most senior pre-hospital practitioners in the Irish setting, with PHECC registration at AP level being a requirement for Specialist Paramedics and previous work on development of alternative care pathways has focused on APs.12,17,18,22 The AP Panellists were fully informed of the aims of the study and the Research Nurse provided standardised training to all participating AP on the chart review and analysis. The Review Panel was selected based on national reputation and experience and was recruited purposively by email invitation initially, followed up by a meeting with the research team. The panel was comprised of registered APs with a minimum of 10 years of experience working on frontline emergency ambulances, in addition to other settings including Fire-based EMS and Aeromedical services. While all panellists currently either worked/studied part-time or full-time in different academic institutions, all maintained clinical competence with some working in voluntary ambulance services. The panellists also comprised both genders and spanned a variety of ages and locations nationally.
Measures of ‘appropriateness’ and rating scale analysis
The APs participating in this study were asked for responses to three questions;
According to you, could the patient have been managed by a GP the same day or next day? Yes/No According to you, was this patient's ED visit an inappropriate use of ED resources? Yes/No According to you, how appropriate was this ED visit? Rating Scale 0–10
Therefore, the measures of appropriateness related to the individual perception of the rater across domains. The ‘appropriateness’ rating scale (0–10) was initially analysed using descriptive statistics. Following consultation with an interprofessional clinical panel the Likert scale was trichotomised as follows; inappropriate (0–3), neither appropriate or inappropriate (4–6) and appropriate (7–10). The proportion of attendances in each category was calculated and cross-tabulated for percentage agreement.
Data analysis
Data entry and coding were conducted in Excel (Microsoft, San Diego, CA), and analysis was performed in SPSS (IBM SPSS Statistics Version 26, Armonk, NY). In the BDBP database pairwise deletion was applied to missing patient data, however there was no missing data documented in the AP Chart Review. Descriptive statistics are presented as frequencies and percentages. Normality testing was conducted using the Kolmogorov–Smirnov test and the data was found to be non-parametric, therefore medians and Interquartile Ranges are presented as measures of central tendency and variability. The Mann–Whitney U test was used to examine relationships between ordinal and continuous variables and the chi-square test or Fisher's exact test was used for categorical variables, depending on expected cell size. Interobserver agreement was calculated using Fleiss’ κ and presented with confidence intervals. 23 The strength of agreement values for κ are: ≤0 indicates no agreement, none to slight 0.01–0.20, fair 0.21–0.40, moderate 0.41– 0.60, substantial 0.61–0.80, and 0.81–1.00 is almost perfect agreement.
Ethical approval
The study was performed in accordance with the Declaration of Helsinki 24 and ethical approval was obtained from the following Research Ethics Committee (REC); University of Limerick Hospitals Group (Ref. 122/19), HSE Midlands Area (Ref: 231019CG), St Vincent's Healthcare Group Ethics and Medical Research Committee (Ref. RS20-004), Tallaght University Hospital/ St James’s Hospital Joint REC (Ref. 2020-04) and Cork Teaching Hospitals (Ref. ECM 4 (J)/ECM 4 (bb). Written informed consent was obtained from all participants for participation and publication.
Reporting guidelines
STROBE reporting guidelines were used in drafting this manuscript 25 and the associated checklist is included in Supplemental File S2.
Results
Demographic and clinical characteristics
The demographic and clinical profile of patients in the BDBP Study have previously been described in full. 8 Of the n = 601 patients attending the participating EDs over the 24 h Census period at each site, a total of n = 306 (51%) were eligible for participation in the BDBP Study and were included in the AP chart review. In this secondary data analysis focusing on AP rated ‘appropriateness’ of ED attendance, 19% of patients (n = 57) were transported by ambulance, while 81% (n = 246) were transported by other means, and n = 3 records did not report mode of transportation (Table 1).
Demographic and clinical characteristics of BDBP participants (n = 306) categorised by mode of transport to the ED.
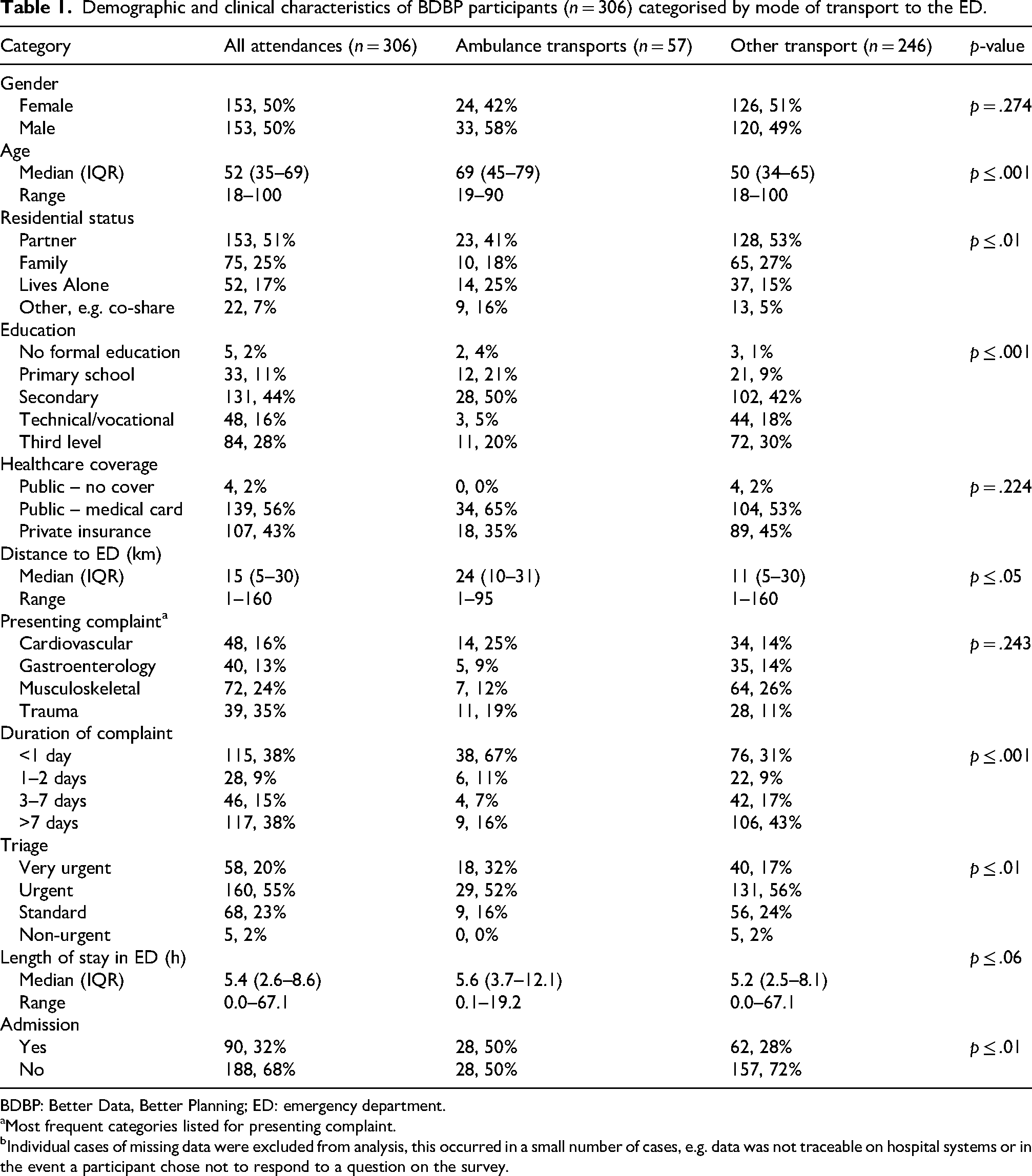
BDBP: Better Data, Better Planning; ED: emergency department.
Most frequent categories listed for presenting complaint.
Individual cases of missing data were excluded from analysis, this occurred in a small number of cases, e.g. data was not traceable on hospital systems or in the event a participant chose not to respond to a question on the survey.
In relation to demographics, significant differences in means of transport were observed across age (p ≤ .001), residential status (p ≤ .01), education (p ≤ .001) and distance to ED (p ≤ .05). Patients transported by ambulance tended to be older (69 y vs. 50 y; p < .001), more likely to live alone (25% vs. 15%; p ≤ .01) and to live further away from the ED (24 km vs. 11 km; p ≤ .05) than patients transported by other means. Patients transported by ambulance were also more likely to report primary school (21% vs. 9%) or secondary school (50% vs. 42%) as their highest level of education (p ≤ .001).
With regard to clinical features, significant differences were observed across the groups in duration of complaint (p ≤ .001), triage category (p ≤ .01), and hospital admission (p ≤ .01). Patients transported by ambulance reported a more recent onset of symptoms (<1 day 67% vs. 31%; p ≤ .001), were more likely to be triaged as very urgent (32% vs. 17%; p ≤ .01); and to be admitted to hospital (50% vs. 28%; (p ≤ .01) than the other transport group. Differences between groups in relation to length of stay in the ED approached significance (p ≤ .06).
Agreement on measures of ‘appropriateness’
With regard to ‘appropriateness’ of ED attendance the AP panellists judged that between 12% to 79% of all ED attendances were suitable for management by a GP on the same or the following day. The level of agreement between the members of the panel was 11%, giving an inter-rater agreement value of κ = 0.120 (p < .001), indicating low agreement. Panellist judgement that the patient's ED visit was an inappropriate use of ED resources ranged from 12% to 73% and the level of inter-rater agreement between members of the panel was 19% (κ = 0.182; p < .001) also indicating low agreement (Table 2).
AP agreement on appropriateness measures for ED attendance (n = 306).
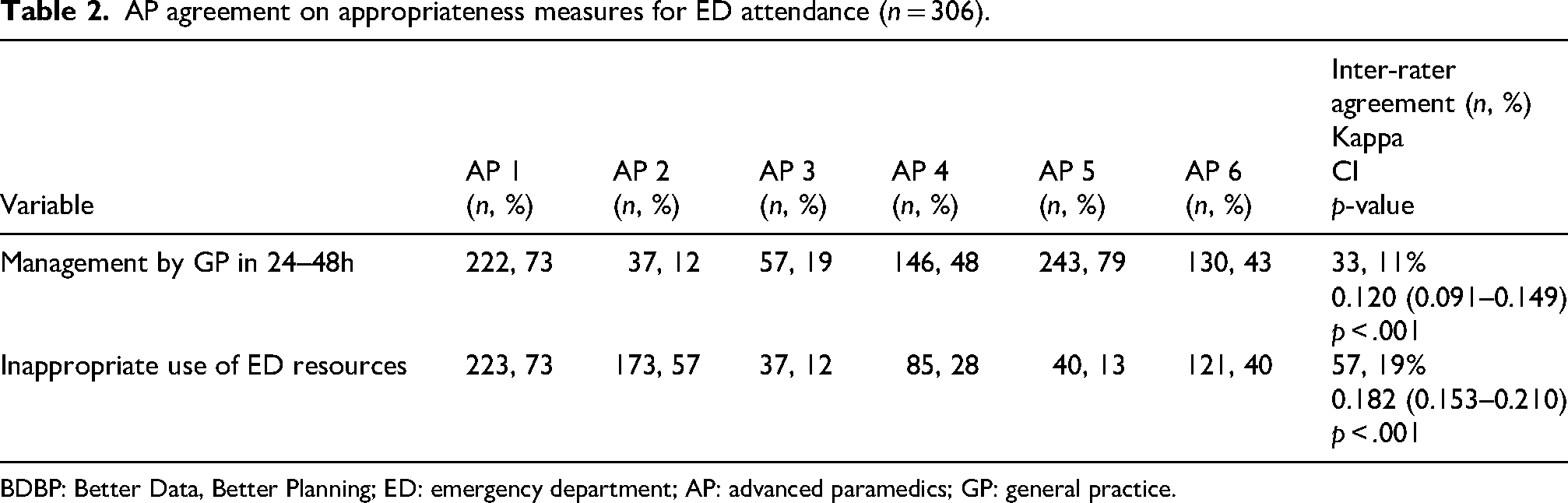
BDBP: Better Data, Better Planning; ED: emergency department; AP: advanced paramedics; GP: general practice.
Members of the AP panel rated the appropriateness of each ED attendance on a Likert scale from 0 (inappropriate) to 10 (appropriate). Ratings varied widely across panellists (Figure 1) and median appropriateness ratings for each panellist ranged from 0 to 6 (Supplemental Tables S2 and S3). Inter-rater Likert scale agreement was κ = −0.003 (−0.14–0.007), indicating no agreement (p < .546).
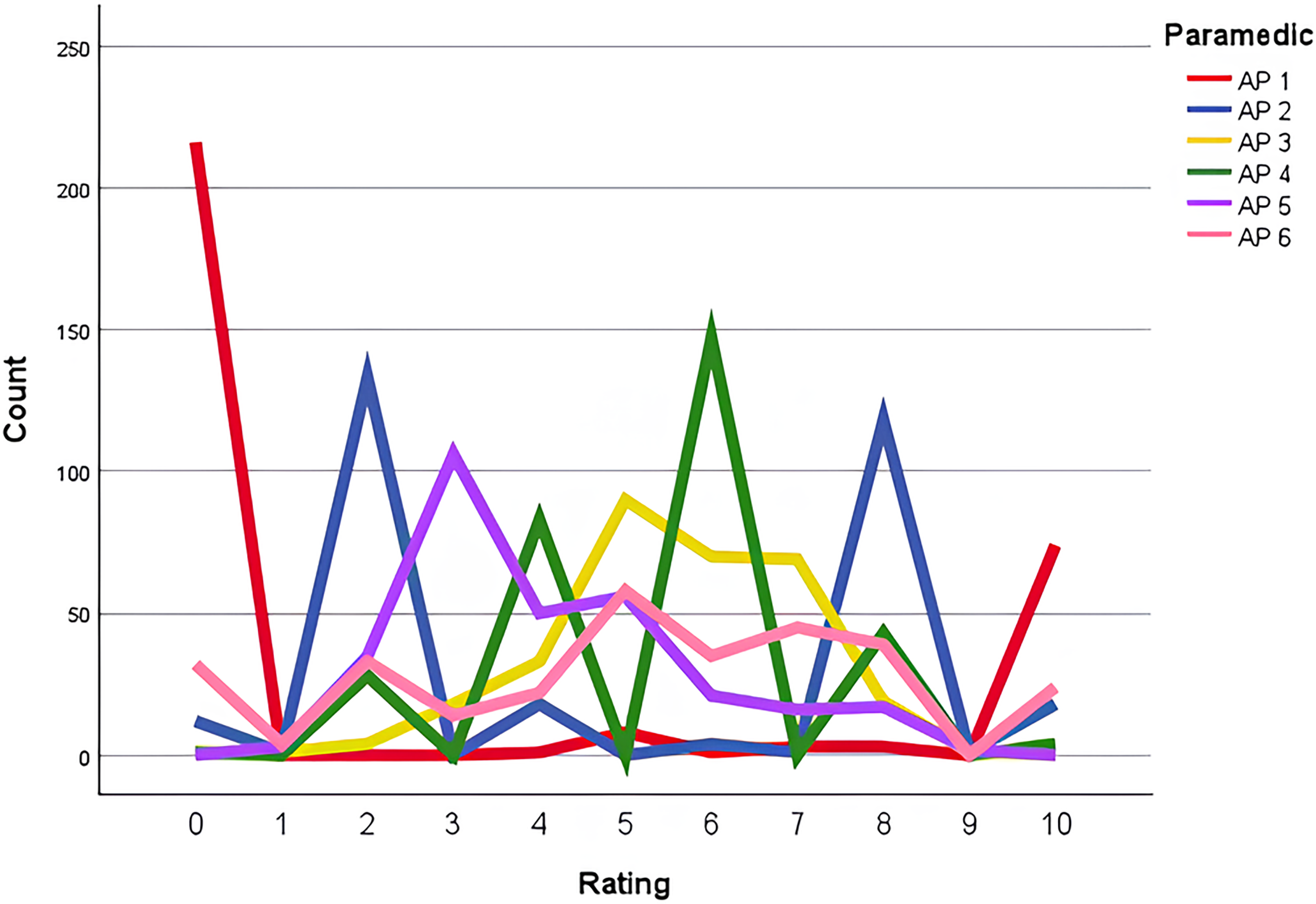
AP Likert scale rating for appropriateness of ED presentations (n = 306).
Appropriateness ratings were trichotomized into ‘inappropriate’ (0–3), ‘Neither inappropriate nor appropriate’ (4–6), and ‘appropriate’ (7–10) categories for analysis. Between 8% and 71% of ED attendances were judged to be inappropriate by panellists, between 3% and 75% of attendances were judged to be neither inappropriate or appropriate and between 11% and 45% of attendances were judged to be appropriate. Using the trichotomised score the APs reached full agreement by all n = 6 panellists, on the appropriateness of ED attendance for 5% of charts (n = 15). Inter-rater agreement for trichotomised appropriateness categories was k = 0.104 (0.083–0.124) p ≤ .001, indicating low agreement (Table 3).
AP agreement on appropriate attendances to the ED according to categorisation of a rating scale of appropriateness (n = 306).
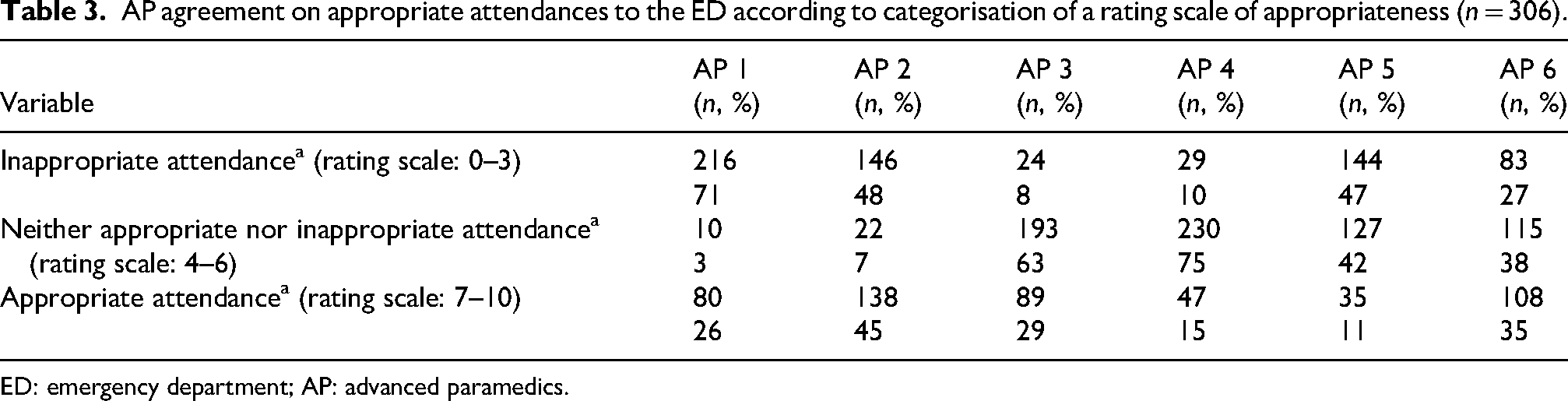
ED: emergency department; AP: advanced paramedics.
In a subset analysis (Table 4) agreement on the appropriateness of management by a GP within 24–48 h was significantly higher in patients transported by ambulance compared to patients transported to the ED by other means (19% vs. 9%, p < .05). Agreement on the inappropriate use of ED resources was also significantly higher in patients transported by ambulance (37% vs. 15% p < .001). However, there was no significant difference between groups in panellist agreement on appropriateness rating (4% vs. 5%, p = .578).
Agreement on measures of appropriateness for ambulance transports (n = 306).
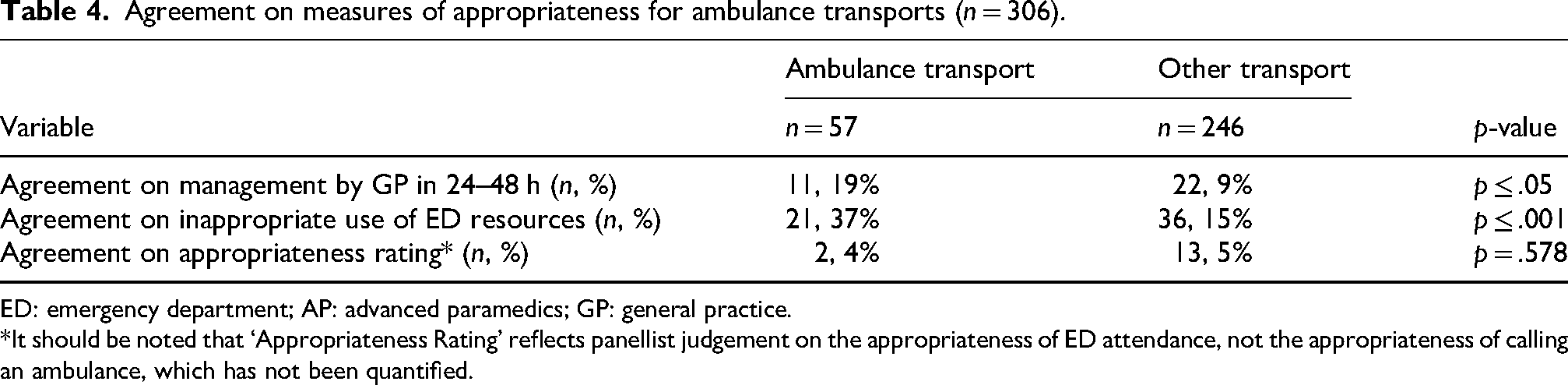
ED: emergency department; AP: advanced paramedics; GP: general practice.
*It should be noted that ‘Appropriateness Rating’ reflects panellist judgement on the appropriateness of ED attendance, not the appropriateness of calling an ambulance, which has not been quantified.
Discussion
The findings of this study suggest that a proportion of low-acuity ED attendances are potentially ‘inappropriate’, however agreement could not be reached by APs on how an ‘inappropriate’ ED attendance can be determined using a series of ‘appropriateness’ measures. Access to urgent and emergency care in health systems should be highly co-ordinated to ensure that time to definitive care is limited and inappropriate use of ED is avoided. However, in the Irish setting the extent to which these services are integrated depends on where, when and by whom the service is provided and regional disparities exist. 19 Therefore, pragmatically it is the case that patients frequently default to accessing care through GPs or the ED 8 and this was the rationale for the ED-GP comparisons and appropriateness measures used in this study.
In this chart review, the APs considered 12% to 73% of low-acuity ED presentations (n = 306) to be an inappropriate use of ED resources, but inter-rater agreement between the panellists was low at 19% (κ = 0.182; p < .001). Similarly, 12% to 79% of low-acuity ED attendances were deemed suitable for management by a GP within 24–48 h, however again panel agreement was low at 11% (κ = 0.120; p < .001). The results of this secondary data analysis are aligned with previously reported findings from the BDBP Study across clinical disciplines on the issue of inappropriate ED attendances in Ireland.9,26 A national GP-Emergency Medicine Consultant Panel previously determined that 18 to 35% of ED attendances (n = 306) could be considered ‘inappropriate’ (Panel Agreement 73%) and reported that 11% to 38% of cases could be treated by a GP within 24–48 h (Panel Agreement 70%). 9 In a single-site analysis of n = 77 cases by an inter-professional panel (including representatives from emergency medicine, GP, nursing and paramedicine) 12–35% of cases were considered an inappropriate use of ED resources (Panel Agreement 58%) and 30–40% of cases were considered suitable for management by GP in 24–48 h (Panel Agreement 56%). 26
In the subset analysis, AP agreement on inappropriate use of ED resources (37% vs. 15% p < .001) and on the management of patients by GP in 24–48 h (19% vs 9%, p < .05) was significantly higher in patients transported to the ED by ambulance compared to patients transported by other means. This may reflect the fact that the APs were more familiar with these presentations as a function of their training. Demographic and clinical differences were observed across these groups and patients transported by ambulance tended to be older (p < .001), more likely to live alone (p ≤ .01) had higher triage scores (p ≤ .01) and were more likely to be admitted to hospital (p ≤ .01), which is in agreement with previously reported findings in the international literature. 27 Social history was included in the Patient Summary files and it must be acknowledged that transport decisions on conveyance are complex and paramedic decision-making may be mitigated by non-clinical factors such as social circumstances. 28 Low acuity ED presentations, as defined by triage category, were the focus of the BDBP Study as these attendances may potentially be avoidable. However, in terms of appropriateness of ED use it must also be acknowledged that some low acuity presentations may still warrant hospital attendance as emergent conditions, even if access is available to alternative care pathways and GP services, and this is particularly the case for out-of-hours presentations. Conversion to admission was not factored into the analysis because it is an imperfect standard for appropriateness of attendance at the ED. 29 Admission thresholds may differ across hospitals and other reasons exist for acute hospital admissions, including the need for additional investigations and procedures.
It is notable that for APs a wide variability was observed for the Likert scale ratings on appropriateness and trichotomisation of appropriateness categories with inter-rater agreement generally being much lower for AP than has been previously reported for other clinical disciplines.9,26 In this study the AP reached full agreement by all n = 6 panellists, on the appropriateness of ED attendance for just 5% of cases (n = 15). This finding is unexpected because Irish pre-hospital practitioners follow defined clinical practice guidelines for assessment, treatment and disposition of patients 15 therefore a more standardised approach and stronger agreement would have been expected by the APs. The patient summary files included details of diagnostic tests ordered for patients after assessment in the ED, and even with the benefit of this knowledge the participating APs did not reach agreement on appropriateness, which serves to highlight how challenging this process is routinely in the prehospital setting. However, it must also be acknowledged that paramedic education focuses on a symptom-based approach to patient care and prioritises the assessment and management of emergent conditions over a definitive diagnosis or disposition decision. 30 In subjective assessments achieving agreement for heterogenous low acuity presentations is complex and differences in clinical judgement for AP may have been influenced by background, training and exposure to alternative care pathways regionally. 31 Additionally, access to follow-up data of patients by paramedics after ED treatment is limited in most Irish hospitals 32 and this lack of continuous feedback to paramedics may also impact decision making and agreement on appropriateness of presentations.
The need for further education on low acuity conditions and alternative care pathways is not unique to Ireland and a recent scoping review highlighted the ‘limited’ scope of current training programmes internationally and the gap which exists between traditional emergency care education and what paramedics actually experience in clinical practice. 33 Internationally, in systems with treat and refer in place, however, paramedics feel they are conveying many patients who do not require their skills or expertise to an ED, and that practical and cultural support to correct this is limited within services. 34
A recent systematic review found that with additional training and an enhanced skillset paramedics can significantly reduce ED presentations and hospital admissions. 35 International best practice in paramedicine has evolved towards ‘Treat and Refer’ pathways which aim to optimise patient care and ambulance service resources by diversion of patients away from EDs to alternative settings. In the Irish context the need for alternative care pathways and the potential for paramedics working in extended practice roles has specifically been recognised in the Sláintecare Strategy. 6 The potential for an extended scope of practice in paramedicine has also been recognised in primary care and there is an appetite among the paramedic profession to pursue roles in GP. 36 It has also been reported that Irish doctors are open to integrating APs as a sustainable model of care in rural GP clinics. 22 Collaboration with GPs would facilitate the identification of cases which can be safely and efficiently managed in the community by alternative care pathways, thereby supporting greater integration of EMS and primary care.
In terms of public and patient perspectives the authors acknowledge that utilisation of the term ‘inappropriate’ in relation to accessing emergency care may represent problematic terminology, despite being commonly used in the medical literature. Regarding access to care and what may be termed inappropriate use of health services, discordance between societal expectations and the expectations of emergency care providers has recently been reported in the Irish setting. 37 Patient choice on alternative care pathways is an important consideration that should be respected and a recent Irish study of older adults utilising the Pathfinder model suggests a strong preference to be cared for at home as an alternative to the ED. 38
Limitations of the study include the fact that the BDBP Study took place during 2020 and therefore the COVID-19 pandemic is a confounding variable for this research and the data could now be considered aged. However, no similar data exists or has been published nationally since and therefore this study does add to the limited body of knowledge on this topic. This data relates to lower acuity attendances in regional Irish EDs therefore outcomes may not be fully applicable to other settings. The sample size of n = 6 AP may not be representative of the workforce which also impacts the generalisability of the findings, although the panel was diverse in terms of clinical experience, demographics, service type and location. A limitation of chart review analysis is that APs must make their decisions without the benefit of meeting the patient. Also, details of the diagnostic tests ordered in the ED were included in the patient summary files, this information would not usually be available in the prehospital setting when paramedics make the decision to convey and this is a further limitation of the chart review analysis. Considering their speciality, it is possible that APs are likely to perceive lower acuity attendances as non-emergencies as they are more accustomed to managing high acuity presentations. As non-conveyance is generally not an option for APs in Ireland (outside of specific alternative care pathways) this means that existing protocols are not in place to judge the appropriateness of ED alternatives or delaying care which may have contributed to poor agreements because the panellists were working off their own heuristics, rather than standardised protocols that would exist if alternative care pathways were implemented widely. Finally, in relation to the statistical analysis, known limitations of kappa coefficients include sensitivity to extreme disagreements between raters and to circumstances where one rater disagrees with other raters consistently. 39
Future research should seek to understand how alternative care pathways could enhance the quality of needs-based care in the community. Paramedic reasoning for their decision-making process in determining appropriateness of ED attendance could be investigated further as could the identification of training needs that may be required for implementation of alternative care pathways. It is important to investigate what supportive protocols for alternative care pathways might look like, and if paramedics would feel comfortable with greater clinical responsibility in making these judgements if provided with suitable guidance. Ambulance services should be resourced and supported in developing these initiatives in order to transition from the ED as a default destination and reduce reliance on secondary care services, aligning with the national Sláintecare strategy to ensure that patients can access the ‘right care, in the right place, at the right time, by the right team’ in the Irish health service.
Conclusions
The findings suggest that ‘inappropriate’ ED attendances represent a proportion of ED attendances in Ireland, however agreement was not reached by APs on what constitutes an ‘inappropriate’ attendance to the ED. This variance can be attributed to multiple clinical factors and could be mitigated by non-clinical factors such as social circumstances, while regional disparities may also impact the decision-making process for APs. This study highlights the complexities which must be considered around developing alternative care pathways for ED avoidance. The potential to develop paramedic roles in Ireland is significant with an emphasis on providing patient-centred care in the community. Integration with primary care is necessary to develop a shared understanding of the feasibility of alternative care pathways and appropriate governance must be established to support decision-making for paramedic roles with an expanded scope of practice.
Supplemental Material
sj-docx-1-pam-10.1177_27536386261453935 - Supplemental material for Advanced paramedic agreement on ‘inappropriate’ emergency department attendances: Secondary data analysis from the better data, better planning study
Supplemental material, sj-docx-1-pam-10.1177_27536386261453935 for Advanced paramedic agreement on ‘inappropriate’ emergency department attendances: Secondary data analysis from the better data, better planning study by Niamh M Cummins, Rose Galvin, Jake S Phillips, Louise A Barry, Eamonn Byrne, Julian Devergie, Keith Hayes, Kieran Henry, Chris O’Connor, Michelle O’Toole and Tomás Barry in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386261453935 - Supplemental material for Advanced paramedic agreement on ‘inappropriate’ emergency department attendances: Secondary data analysis from the better data, better planning study
Supplemental material, sj-docx-2-pam-10.1177_27536386261453935 for Advanced paramedic agreement on ‘inappropriate’ emergency department attendances: Secondary data analysis from the better data, better planning study by Niamh M Cummins, Rose Galvin, Jake S Phillips, Louise A Barry, Eamonn Byrne, Julian Devergie, Keith Hayes, Kieran Henry, Chris O’Connor, Michelle O’Toole and Tomás Barry in Paramedicine
Footnotes
Acknowledgements
The authors would like to acknowledge the assistance of all the staff in each of the regional ED, and sincerely thank the participants, without whom this research would not be possible.
Ethical approval
The study was performed in accordance with the Declaration of Helsinki and ethical approval was obtained from the following Research Ethics Committee (REC); University of Limerick Hospitals Group (Ref. 122/19), HSE Midlands Area (Ref: 231019CG), St Vincent's Healthcare Group Ethics and Medical Research Committee (Ref. RS20-004), Tallaght University Hospital/ St James's Hospital Joint REC (Ref. 2020-04) and Cork Teaching Hospitals (Ref. ECM 4 (J)/ECM 4 (bb). Written informed consent was obtained from all participants for participation and publication.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Health Research Board, Health Service Executive Clinical Design and Innovation Office (Grant No. Clinician Scientist Fellowships 2020 006, Emerging Clinician Scientist Awards 2024 002, 2019–2021) and University of Limerick Education and Health Sciences (EHS) Seed Funding.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NMC is an Associate Editor at Paramedicine. She played no role in the editorial process, which was conducted in adherence to the journal's published peer review processes. The remaining authors have no conflicts to declare.
Availability of data
The BDBP dataset is available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.