
Abstract
Placement experiences are a fundamental component of tertiary paramedicine programs, where students can link theory with practice. However, the quality of placement experiences has been known to vary. Students have reported varying levels of placement satisfaction, supervisory support, clinical exposure and opportunities for learning. This scoping review aims to explore the factors that influence quality paramedicine student placements. The Joanna Briggs Institute Scoping Review Methodology guided this study. The electronic databases MEDLINE, Emcare, Scopus and CINAHL were comprehensively searched in February 2025 and again in October 2025 for relevant peer-reviewed research articles. The initial search strategy was developed in MEDLINE and subsequently adapted to each database. Title and abstract screening was conducted first, followed by full-text screening, as per the Joanna Briggs Institute Scoping Review methodology. Included articles were assessed for methodological quality. The search strategy resulted in 13,479 articles for screening. A total of 25 met the inclusion criteria. Several key factors were identified which influence quality paramedicine student placements: (i) the impact of supervisors; (ii) the learning experiences of students; (iii) placement setting and structure; and (iv) student satisfaction. Identifying these quality indicators will allow stakeholders, including universities and placement providers, to develop strategies to improve the paramedicine student placement experience.
Introduction
Placement experiences are a core element of paramedicine programs within Australia and form a fundamental component of the Paramedicine Board of Australia's accreditation standards for education providers.1,2 While the value of clinical education is universal, the way it is delivered varies considerably across countries and professions. In Australia, New Zealand and the United Kingdom (UK), undergraduate baccalaureate paramedicine courses are now standard for entry to practice, ranging from 3 to 4 years in duration.3,4 Within the United States of America and Canada, paramedic education is mainly delivered through accredited training programs.5,6 These differences in educational models mirror the variability found internationally in paramedic roles themselves. Historically, paramedics were primarily situated within pre-hospital emergency care, focusing on acute response and transport. Over the last two decades, the profession has undergone substantial evolution, expanding well beyond traditional emergency or transport-only functions. 7 Today, paramedics clinically work across a spectrum of settings, including primary and tertiary care, community health, and ambulance services, with scopes of practice and educational requirements that differ by jurisdiction. 4 As a result of diversification in roles, training pathways, and scopes of practice, paramedicine now exerts a broader and more significant influence across contemporary health systems globally.
The learning theories of experiential learning, situated learning, reflective practice and adult learning theory have all been highlighted as underpinning the design and development of paramedicine education programs. 8 These theories align with constructivism, which outlines that learning is an active process, with learners using experiences and ideas to construct new knowledge and meaning.9,10 Clinical placement, or work-integrated learning, is designed to link theory with practice2,3,11,12 and facilitate development of students’ professionalism, competence, confidence 13 and self-directedness. 14 Students also cultivate interpersonal and organisational attributes, 15 deemed essential skills as employers increasingly expect graduates to demonstrate problem-solving, critical thinking, and communication abilities alongside academic success. 4 Supportive learning environments for placement experiences are invaluable, facilitating student growth and enabling better achievement of learning outcomes.16,17
Within Australia, paramedicine students primarily complete placement with jurisdictional ambulance services, engaging in an operational ambulance environment under the supervision of one or more paramedics. 18 There is demand for diversification of paramedicine placements, 1 and students are more frequently attending non-traditional placements, such as hospital or community-based. 4 This expansion of placement settings has also been driven by a significant increase in student enrolments due to the transition to a tertiary entry-to-practice education model. 18 Notwithstanding, the quality of paramedicine student placement experiences has been known to vary,19,20 with students frequently encountering poor quality ambulance placements due to physical and psychological safety concerns, resulting in negative learning experiences. 21 This includes placements that did not provide theory consolidation or skills practice for their level of education.3,4,20 Placement experiences have been associated with significant student emotional distress, inability to focus on learning, and an urgent need for financial support.22,23 These factors can impact students’ success in their placement. This is particularly pertinent in a profession that is already physically and emotionally demanding.
Currently, there are no standards or framework in Australia regarding the quality of paramedicine student placements, including supervisory requirements, the number of hours of placement, or where and when placement should be undertaken. 11 Subsequently, there is significant inconsistency in placement experiences and expectations of students and supervisors. This contrasts with international programs. For example, the College of Paramedics (UK) have developed standards for paramedicine student placements, including a commitment from stakeholders that no less than 30 weeks (1125 hours) of pre-registration education should be clinical placement, of which 20% (225 hours) would be in areas outside of traditional emergency ambulances. 24
Five factors were identified which enable quality placement experiences for health students, including a culture of quality, effective supervision, learning opportunities, effective communication and collaboration, and resources and facilities. 5 More recently, research has highlighted four domains of quality clinical practice within higher education: student experience, curriculum design, institutional requirements and stakeholder engagement. 25 However, while it is apparent that some evidence exists to describe the conditions ideal for quality placements in the tertiary education or health sector, none of this evidence identifies elements specific to paramedicine, particularly post the introduction of registration in 2018. 26 Therefore, the aim of this scoping review is to explore the factors that influence quality paramedicine student placements within Australia. From this, the definition and measurement of quality will be investigated. The results of this study may allow for the identification of quality indicators for paramedicine placements, enabling benchmarking, and aid in developing strategies to improve the student placement experience.
Methods
The Joanna Briggs Institute (JBI) Scoping Review Methodology 27 was adhered to for this review. A scoping review was identified as the most appropriate methodology to address the aim, as it identified knowledge gaps, the types of available evidence in the field of paramedicine placements and investigated key contributors related to the topic. 27 The findings were reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR) guidelines. 28 A review protocol was formulated and published on the Open Science Framework (registration number: 10.17605/OSF.IO/R6NZ8).
Review question
What are the factors that influence quality Australian paramedicine student placements?
Inclusion and exclusion criteria
To address the aim of this scoping review, research articles that met the following population, concept and context (PCC) search strategy were eligible for inclusion: Population: Paramedicine student studying at an Australian University Concept: Placement experience completed as part of a university program, within Australia or at an international location (encompassing all types of placements students experience within their studies e.g. clinical and non-clinical) Context: University program (inclusive of undergraduate and post graduate programs)
Quantitative, qualitative, and mixed-method studies that explored factors that influenced the quality of placement experience, in line with the PCC explanation above, were eligible for inclusion. Studies were also eligible for inclusion where paramedicine students were a sub-cohort of the overall participants, and the population of interest could be distinguished from other cohorts within the results. Grey literature was also eligible for inclusion. Studies were excluded if they had an unsuitable study design (this included reviews, case studies and editorials), were not available in English language (to ensure accuracy and ease of interpretation), or full text access was not available.
Search strategy
Academic literature was systematically searched in February and October 2025, using four electronic peer-reviewed databases: MEDLINE (Ovid), Emcare (Ovid), Scopus (Elsevier) and CINAHL (EBESCOhost) with no time limits applied. ERIC was excluded as initial trial searches did not find any ‘gold set’ articles (articles highlighted following preliminary research on the topic area). The search strategy utilised a variety of words formulated from synonyms of the key words and concepts. It was developed and modified in collaboration with a medical librarian to improve quality. Subject headings were utilised where appropriate and adapted as required for individual databases. The PRESS Guideline checklist was also utilised to ensure rigour in search strategy development. 29 The base search strategy used in MEDLINE (Ovid) is provided in Table 1.
Search strategy as per MEDLINE (Ovid).

Grey literature was identified through manual searches of published conference abstracts, Trove, Google, national health websites, known related non-indexed related journals including International Journal of Paramedicine, Irish Journal of Paramedicine, and South African Journal of Prehospital Care, and professional association websites. These searches were conducted in August 2025 (Supplemental Material 2). A targeted search strategy was utilised due to limited advanced search functionality on some platforms, screening only the first 100 results. Articles and grey literature will be collectively referred to as sources.
Study selection
One author (AF) conducted the literature search and imported the results into EndNote 30 and Covidence 31 for review and removal of duplicates. Articles were then subjected to independent title and abstract screening, using the eligibility criteria by two authors (AF and CF). Remaining articles underwent independent full-text screening for eligibility by two authors using the same criteria. Any conflicts were resolved by a third author (CG). Reviewers were not blinded to any components of the eligible sources. Once the accepted sources were confirmed, the citation lists of each included article were reviewed via Citation Chaser. 32 The method collated all reference lists of included sources (backward citation searching) as well as future publications that had cited the included sources (forward citation chaining). Eligible literature not previously identified was included at this point.
Deviation from protocol
The final manuscript deviated from the a priori protocol by refining the exclusion criteria to better align with the student paramedicine population. This included the exclusion of sources where paramedicine students were a sub-cohort of the overall participants, and the population of interest could not be distinguished from other participants within the results.
Data extraction and analysis
Data from the included sources was extracted into Covidence. 31 The variables extracted for each article included author(s), publication year, country of placement, study aim(s), study design, study population, and key findings related to the research question. Descriptive statistics were employed to appropriately summarise the data. In accordance with the JBI methodology for scoping reviews, data was synthesised using a content analysis approach.33,34 This was completed in Excel and involved identifying themes within the data according to the core factors identified through semantic inductive coding. This was followed by further descriptive content analysis of the findings relevant to the review's aims. 35 One researcher (AF) independently reviewed and coded each included text at the semantic level, identifying recurring concepts and generating initial themes. The authors then met to discuss and collate these themes into overarching categories and sub-categories. The data extraction template was created as per the JBI scoping review guidelines 27 and presented in tabular form.36,37
Results
Study inclusion
A total of 13,479 articles were identified through database searching. After the removal of duplicates, 9514 publications underwent title and abstract screening. A total of 55 articles were assessed for eligibility at the full-text stage. Manual searching, which included grey literature and citation searching, identified four resources of evidence, resulting in 25 sources included for analysis. The search and study selection process is presented in Figure 1.
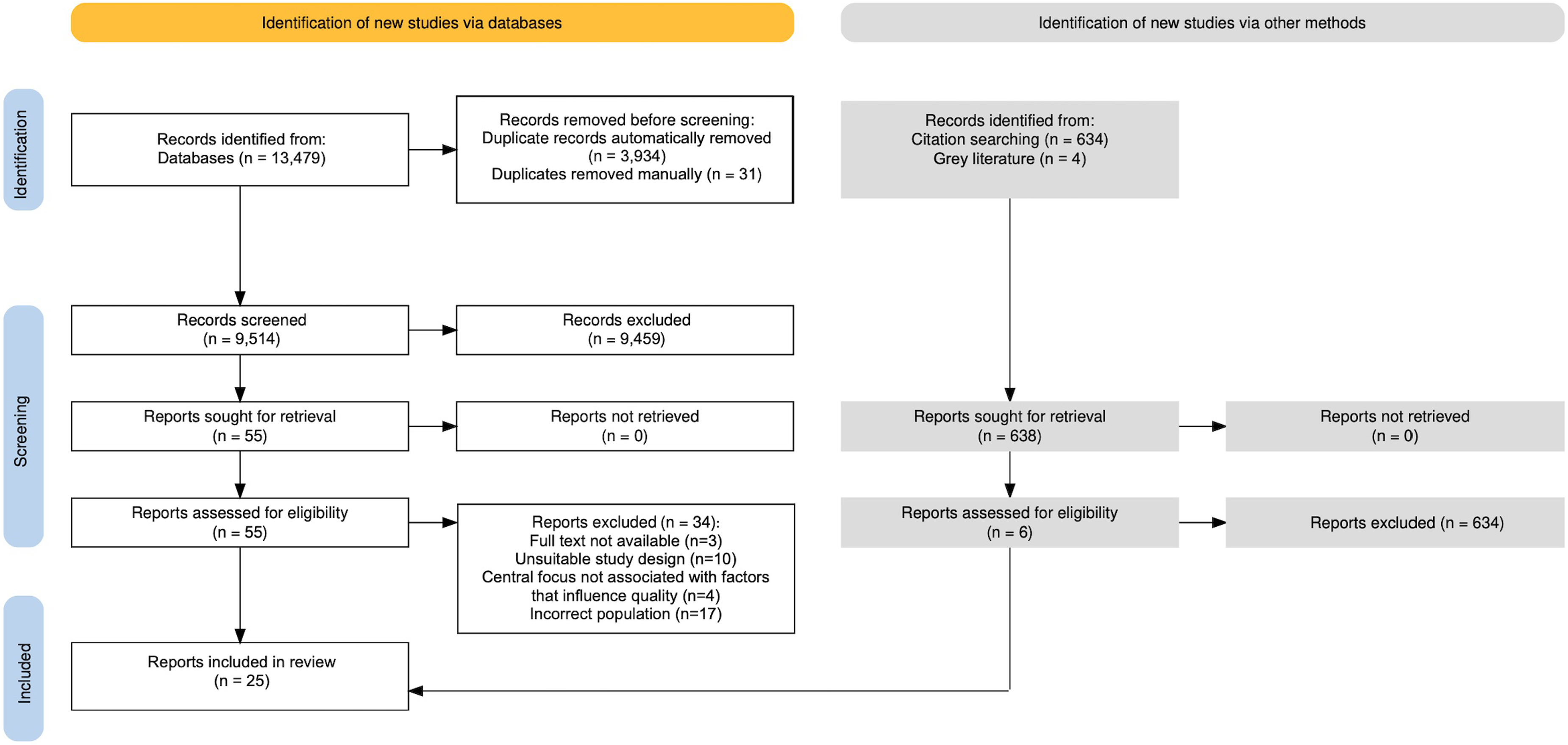
PRISMA flowchart of included publications.
Study characteristics
Publication dates ranged from 2007 to 2025, with 17 (68%) of the included sources published prior to the introduction of paramedic registration in 2018 (see Figure 2). Included sources involved placement experiences conducted in Australia (n = 20, 80%) and a small proportion conducted in other countries, including New Zealand (n = 3, 12%), Israel (n = 2, 8%), Vanuatu (n = 2, 8%) and South Africa (n = 2, 8%). The most common study designs were cross-sectional surveys (n = 13, 52%) and qualitative methods (n = 6, 24%). Articles were published in 16 different journals, with the ‘Australasian Journal of Paramedicine’ (n = 4, 17%) and the ‘Journal of Paramedic Practice’ (n = 3, 13%) the most common (Table 2). A summary of the results of the included sources is provided in Table 3. No source reported on a measure of quality for Australian paramedicine student placements.

Publications per year of included sources.
Categories and sub-categories of factors that influence quality paramedicine student placements.

Characteristics of included studies.

Four categories were derived after narrative data synthesis that pointed toward placement quality indicators being: (i) impact of supervisors; (ii) learning experience; (iii) setting and structure; and (iv) student satisfaction. See Table 3 for the development of these categorical indicators of quality with branching sub-categories.
Discussion
This scoping review sought to explore the factors that influence quality paramedicine student placements. Identifying these quality indicators is important from the perspective of key stakeholders, including universities and placement providers. Through defining both the enablers and barriers to quality placement experiences, stakeholders can maximise the value of these experiences by providing clear quality placement standards. This, in turn, will improve student experience. The 25 included sources identified four primary categories that influence quality paramedicine student placements, namely the impact of supervisors, the types and quality of learning experiences, the setting and structure of placement, and student satisfaction.
Impact of supervisors
Supervisors responsible for students on placement were found to have a significant impact on the quality of the student placement experience, both positive and negative. Key factors included the importance of a supportive supervisor-student relationship, the need for appropriately trained supervisors, suitable allocation of and preparation of supervisors, the importance of student safety, good communication and desirable personal attributes that all lead to quality reported placement experiences.
A supportive, collaborative and positive supervisor-student relationship was found to be essential to increase students’ wellbeing and enable students to fully engage in learning activities while on placement.42,53 This educational relationship was found to lead to more effective learning and was important for students to develop key clinical and professional competencies. 54 A discrepancy between supervisor perspectives was identified. Vocationally trained paramedics believed student placements were observational in nature, whereas university-trained paramedics believed active participation was essential. 55 This variation could ultimately impact student experience. A statistically significant relationship has been previously established between the overall satisfaction of health professional students and the workplace supervision they received. 63 Effective supervision was also found to enhance health professional students’ learning, increased confidence and reduced stress. 64 Several key capabilities required for the paramedic ‘preceptor’ role have been established within the literature, with ‘building positive relationships’ outlined as fundamental. 65 This importance of effective supervisor–student relationships cannot be overstated. They foster optimal student learning and have the potential to enhance the overall quality of the placement experience.
There was also an identified need for individuals to have the necessary skills and knowledge required to be a supervisor, via purpose-built training programs. A framework for best practice clinical learning environments outlined which supervisors were recommended to be high-quality and appropriately qualified staff, who possess the knowledge, skills and competence to supervise students adequately. 43 The need for standardised supervisory training was identified as crucial to establish students’ learning needs and enhance skills required to effectively support practice.53,54 Yet it is not purely the responsibility of the supervisor and student to participate in learning; a culture of education must exist within the organisation, where education, educators and students are valued. 43 This is a shared responsibility between jurisdictional services, tertiary institutions, and supervisors. A recent Australasian paramedicine workforce survey report found that only 42% of Australian paramedic participants felt ‘very well’ or ‘extremely well’ prepared for supervision and 10% perceived they were not well prepared at all. 66 Paramedic students in the UK identified practice educators who had greater training and experience in education, good clinical knowledge and understanding, were more effective facilitators of positive learning environments.67,68 Additionally, variations in supervisor quality and lack of training were identified as contributing to the exclusion of placement experiences from formal assessment.4,20 Increasing concern existed regarding the shortage of supervisors and the variability in supervisory standards in some university placements. An issue presumed to be largely driven by the growing demands for student placements and the lack of appropriately trained individuals to take on supervisory roles. 69 There is a significant need for supervisors to undertake formal training to support their practice of supervising students. This, better armed supervisors with the tools to provide engaging learning experiences, implement effective learning strategies, be adaptable to different learning styles, and foster a culture of education within placement settings, ultimately improving the quality of the placement experience for students.
Findings also indicated the value of allocating students to a single, appropriately trained supervisor for their placement, with advance notice provided.43,55 In one study, only 44% of students were allocated to a ‘Clinical Instructor’. 40 Situations where supervisors were unaware that students were allocated to them for placement were reported, resulting in unsatisfactory initial experiences for both students and supervisors.53,54 Wider health sciences literature has established that healthcare students’ initial impressions on placement served as a barometer to determine how their placements would progress.70–72 Students who began their placement with feelings of alienation or apprehension led to levels of distress and anxiety, while those who were made to feel welcome resulted in feeling valued and accepted. 71 The first impressions on placement were strong indicators of students’ capacity and motivation to learn. Strengthening communication processes between tertiary institutions, placement providers, and supervisors could facilitate adequate planning and optimise placement experiences for students.
Supervisors, if adequately prepared and possess amicable personal qualities, can positively impact the quality of placement experiences. This was achieved when supervisors are professional, 41 well prepared,44,45 supportive,44,45 welcoming,41–43,46 accommodating of student involvement40–43,51,53 and create an encouraging and safe learning environment.41–43 Conversely, supervisors who had little engagement with students, 52 appeared ‘burnt out’, 48 inconvenienced, disappointed, and burdened by students, hampered the students’ learning experiences. 42 Demonstrating professional behaviour, interpersonal interactions, having an intrinsic desire to initiate learning opportunities, enthusiasm and motivation are attributes outlined within a recent study highlighting the capabilities for paramedic preceptors. 65 These attributes were also reinforced within the nursing literature, 73 whereby nursing students appreciated staff who willingly shared their knowledge and skills and involved them in patient care activities, describing the professional generosity as validation that their role as a student was valued and respected. 71 These personal attributes are essential not only to motivate paramedic students to succeed in their learning but also in creating a safe environment, optimal for quality student learning.
The Paramedicine Board of Australia's accreditation standards identify that students should be afforded physical, psychological and cultural safety while on clinical placement. 1 Paramedicine students often experience poor quality placement experiences due to physical and psychological safety concerns, leading to negative learning experiences. Students have reported experiencing bullying or harassment on placement, often perpetrated from those directly supervising them,38–40,42,48,56 including verbal38,39,42,56 and psychological abuse,38–40,56 physical violence 39 and sexual harassment.38–40,56 Student psychological safety concerns have been previously established within paramedicine literature, whereby paramedicine students have been known to be treated with incivility from supervisors, 5 experience exclusionary behaviours 74 and provided non-constructive feedback. 75 These findings contrast with the Paramedicine Board of Australia's 76 professional capabilities for registered paramedics, which emphasise the obligation of paramedics to foster the development of others, including supporting students in achieving their learning objectives. Psychological safety is required for effective student learning to occur, 61 a previously highlighted key capability for the paramedic preceptor role. 65 Currently, there appears to be no studies examining cultural safety on placement. To ensure that quality placement experiences can be established, supervisors must be advocates for student safety and establish safe learning environments.
Clear communication between students, supervisors and stakeholders involved in placement education were found to be critical for effective clinical education. Students and supervisors often didn’t know each other's capabilities, meaning students had to be more self-directed in sourcing learning opportunities.46,52,57 Similar findings are present in wider literature whereby paramedicine students reported that supervisors are often not aware of the student's role and responsibilities, limiting their involvement and engagement 3 and misaligned placement expectations for both groups. 20 While it is the responsibility of the student to provide necessary information to supervisors, this should also be a shared responsibility between placement providers and the tertiary sector. 1 This ineffective communication can challenge students to access meaningful learning opportunities and navigate placement expectations. Effective communication between supervisors, students, universities and organisations has been highlighted to be conductive to quality student placements. 43 Regardless, situations present whereby the disconnect between student and supervisor's expectations are detrimental to student learning, introducing unnecessary risk and stress.
The impact of supervisors on the quality of paramedicine student placements is significant. Evidence outlines several key factors specific to supervisors, including the importance of a supportive supervisor–student relationship, supervisors who are appropriately trained, personal attributes, suitable allocation, the supervisor's role in advocating for student safety, and open and consistent communication. These factors influence student well-being, motivation and ability to engage effectively on placement.
Learning experiences
The opportunity to engage in active learning experiences plays a pivotal role in student satisfaction and the quality of paramedicine student placement. This can be influenced by factors including student preparedness, ability to participate in ‘hands on’ experience, actual student learning, diverse placement settings, and the use of ‘downtime’.
The ability of a student to be fully prepared for placement often relates to their level of engagement in the process. It is important that students are prepared and have clear, structured placement objectives, 43 particularly pertinent in diverse placement settings.41,52 Students who attended international placements reported prior learning adequately prepared them clinically,44–46 but not for working within interdisciplinary teams. 46 Further evidence of student preparedness was reported by Gosling et al., 47 where skills refined throughout their course weren’t always effective for communicating with special needs persons, and introductory training on placement had better prepared students. However, the benefit of education sessions on placement had mixed results, often seen to detract from ‘hands on’ practical learning in some settings.52,60 A statistically significant relationship between receiving educational resources during placement and overall satisfaction of health professional students has been previously established. 63 While content learnt at university does appear to sufficiently prepare students clinically, gaps exist surrounding interpersonal skills and working with diverse populations. This suggests the need for tailored ‘on the job’ training programs specific to the placement setting, which consider students’ university curriculum to ensure appropriate student preparation and quality experiences. This is a profession-wide responsibility – a responsibility of a partnership between placement providers, the tertiary sector and professional bodies.
Students require sufficient ‘hands on’ experience throughout their placement to maximise the opportunities for connecting theory with practice. Without adequate ‘hands on’ experience, students are often faced with a lower-quality educational experience. Students could participate in active practical experience on placement, either during patient management or ‘downtime’.40,44,45 While periods of ‘downtime’ present opportunities for structured learning activities to occur, students experienced unproductive use of ‘downtime’. 40 It is evident that there are missed learning opportunities occurring on placement. Variances in clinical exposure and opportunities to participate in clinical scenarios or practice skills were reported,40,53 subsequently reducing overall student satisfaction.44–46,52 In particular, placement satisfaction dropped when cases were purely non-emergency in nature. 61 Simpson et al. 57 outlined that students utilised emergency cases to ‘test’ their compatibility for a career in paramedicine and were often disappointed if not presented with these opportunities. Students should be provided with appropriate learning opportunities in order to establish a best-practice clinical learning environment. 43 Standard 3.13 of the Paramedicine Board of Australia's accreditation standards highlights that clinical placements within paramedicine programs should possess the ‘quality, quantity, duration and diversity of students experience’ (p. 21) to produce graduates with the capability to practise across a range of settings. 1 It has been previously established that paramedicine students were satisfied with the number of cases they attended on placement, yet believed structured learning activities during downtime would be beneficial. 3 Unpredictability in caseload is not a surprising finding, given most placements for paramedicine students occur in ambulance settings. Students’ expectations for placement were not reported within this review's results; however, they could feed into their satisfaction with a quality placement. Sending students on placements alone does not ensure learning will occur. These highly variable placement experiences result in differing levels of student learning, satisfaction and variances in quality.
Placement experiences were described to support students’ learning in a broad range of knowledge and skills. Several studies reported these experiences contributed to students’ learning surrounding interpersonal skills, 50 paramedic practice, ambulance operations, 61 equipment 42 and consolidation of clinical learning objectives.44,45 Contrasting findings were reported regarding students’ ability to access and manage patients.44,45 A considerable attraction for students on placement experiences is to ‘put to practice’ what has been learned in the classroom. There is a need to further structure experiences to ensure student learning is maximised. This is particularly important for placements conducted in an ambulance environment, where front-line operations are the priority, rather than student education.
Non-traditional, diverse placement settings exposed students to a wide range of patient groups, health professionals and health systems. They have the potential to provide quality learning experiences to students that can’t be achieved within the ambulance setting. Students’ skills, attitudes and knowledge were broadened through exposure to mental health patients, 41 elderly patients,51,59 special needs students 47 and other health professionals.41,46,47,51 Interprofessional learning experiences while on placement have been linked to overall placement satisfaction in a wide range of disciplines. 63 These opportunities provide students with important learning experiences to contrast between other various health and community settings. Students perceived differences in scope of practice, education and resourcing on diverse placements as facilitators and barriers to learning.49,52 Previous research has found that non-traditional placement activities consistently lack opportunities to apply theoretical learning in practice. It has been argued that these experiences may offer limited educational value for students and minimal benefit to the host organisation. 4 However, diverse placement settings can broaden students’ knowledge, better equipping them to assess and manage patients from vulnerable groups while offering unique placements with quality learning.
Active student participation in placement experiences contribute to student learning and professional development. Ensuring that the learning experiences are maximised is crucial in establishing quality placement experiences for students. This starts prior to placement, beginning through adequate student preparedness and follows on to the activities conducted on placement, whereby students should be actively involved in placement activities, including during downtime, for actual learning to be optimised. This includes in diverse placement settings, which offer unique learning opportunities.
Setting and structure
Various logistical elements of paramedicine student placements have been reported to impact students’ satisfaction and success on placement. These include scheduling communication and rostering requirements, location of the placement, financial implications to students and experiences within non-traditional settings.
Placement duration and location, coordination, and orientation practices play a critical role in fostering student confidence, continuity of learning, and was found to shape students’ ability to engage in meaningful learning and contribute to the quality of placement experiences. Students reported scheduling issues, including being left at an ambulance station, allocated to another paramedic crew,40,48 or being sent home when no crews were available. 48 Poor rostering coordination 52 and unsatisfactory organisational communication53,54 led to student difficulties in engaging in meaningful tasks, limited opportunities for interprofessional learning and supervisors unaware of who to communicate with at universities regarding student concerns.53,54 Not only does this present potential student safety concerns, but it also unveils ineffective coordination between placement providers and universities.
Clinical placements varied in duration from a single day to 7 weeks.55,46 However, it is argued that limited duration does not always equate to poor quality. 4 Logistical difficulties in managing short-duration placements and the limited learning opportunities they offered were reported.54,61 Longer duration placements and continuity of location and supervisor were reported to afford supervisors and students greater familiarity, increased student confidence and learning opportunities.42,54,55 The duration of placement plays a key role in enabling active and engaged learning as students need time to acclimate and establish relationships with colleagues to foster a sense of belonging. 71 Continuity of placement experiences also supported supervisors to better identify students’ learning needs. 43 Given the unpredictable nature of paramedic practice, supervisors have been found to not have adequate time to accurately determine students’ competency.4,77 A quality paramedicine student placement should possess continuity of location and supervisor, be of a longer duration, and have improved rostering and communication.
Placement location also had a significant influence on the quality of the placement experience, with students often encountering contrasting experiences depending on location. Rural and metropolitan based placement were valued for their different contributions to learning. 42 Metropolitan placements were found to allow students to experience a variety of sites and encounter a range of case types, particularly emergency situations. However, this did not result in added learning benefits with students reporting the need to build effective supervisor–student relationships, particularly if they did not have continuity of location and supervisor. 53
There were inconsistent findings in relation to rural placements. Despite being reported as being more favourable than metropolitan locations, 40 quality rural placement experiences were often dependent on the occurrence of cases attended by students, which were often infrequent.53,61 The advantages of rural placements have been seen in a wide range of health disciplines, including more hands-on learning, exposure to a wider range of patients, and better mentorship.63,78 Similar results have been found with paramedicine students, whereby placement location and duration were found to have a significant influence on student experience.4,20 Variances in quality clearly exist based on placement location and resulting learning experiences. These factors have a considerable impact on the student placement experience.
There are significant financial implications for students when attending placement. With little financial support available, paramedicine students’ engagement and ability to learn is affected, resulting in poor-quality experiences. Wray and McCall (2007) reported that paramedicine students did not receive any financial assistance from their university for placement. 62 Students were required to cover all costs, including transport, meals, mandatory placement requirements such as uniforms, and accommodation, which were reported to be as much as A$700 per week (equivalent to A$1135.33 in 2025).62,79 Darcy Associates 43 outlined as part of the framework for best practice clinical learning environment, assistance should be provided to health students to cover the costs associated with placement away from their home base. Currently, some universities offer nominal financial assistance to support paramedicine students attending placement. 80 Broadly, it has been established that non-medical health students were less likely to receive organisation, mental health, social or financial support for placement and generally paid almost twice as much for placement costs in comparison to medical students (mean weekly cost of accommodation: $117.7 vs. $62.6; equivalent to $145.8 vs. $77.6 in 2025).78,79 It is clear to see ‘placement poverty’ exists among paramedicine students, echoing concerns raised in the recent Australian Universities Accord Report. 69 These financial strains may decrease the appeal of paramedicine degrees and present a significant barrier for students from lower socioeconomic backgrounds enrolling, impacting the diversity of the future workforce.
Paramedicine students’ complete placement in a wide range of settings, both nationally and internationally. Some settings are viewed by students more favourably than others, with quality a consideration. 55 A range of placement settings suitable for paramedicine students were identified, including primary healthcare, general practice, aged care, mental health, emergency departments, intensive care, and midwifery settings. 55 Experiences within the emergency department were the most favoured hospital-based placement by students,42,44 while Coroner settings were the least favoured. 42 One study reported that students self-sourced their own volunteer community placements, which resulted in students attending a broad range of settings. 50 Whilst it may be beneficial to have the opportunity to attend a variety of placement settings, this diversity also results in variable workload and clinical exposure for students. 57 Disagreement existed within the paramedic workforce, based upon one's own training pathway, as to whether placements should be purely in ambulance services or across a diverse range of settings. 54 When the profession cannot agree on the benefits of diverse placement settings, a challenge exists in prompting the educational value of these settings to students. Diverse placement settings, including non-ambulance placements and international settings, are meaningful learning experiences with clear indicators of quality. Despite this, there is a risk to quality if placements aren’t appropriately standardised.
Student satisfaction
Students’ satisfaction with their placement experience is a key factor influencing quality and, as previously discussed, is influenced by factors previously mentioned. ‘Satisfaction’ was highlighted as an important clinical learning domain, 60 with students reporting positive experiences40–42,47,50 that would benefit others.41,44 However, student placement satisfaction varied. 61 This contrasts with undergraduate nursing students, who have a high level of satisfaction with their clinical placements, particularly regarding patient and personal safety and the future application to learning. 81 It should be noted that nursing have provided a strong tool to measure quality student placements, of which ‘satisfaction’ is one element, unlike paramedicine.12,81
International placement experiences were perceived to make students more independent, 49 employable,44,46 foster maturity, 46 encourage professional growth,41,57 networking44,46 and support workplace transition. 46 Additionally, students perceived they enhanced global paramedic perspectives44,45 and improved students’ cultural safety.44,45,49 Nevertheless, it should be noted that although international placements are seen to be positive experiences, they are frequently generated by the ‘wow’ factor and often have low participant numbers.44,45,49,58 Student satisfaction of their placement experience has a clear relationship to the quality of the placement itself, impacted by elements such as student learning, duration and placement setting.
The impact of paramedic registration
Prior to the introduction of paramedic registration in 2018 and paramedicine course accreditation in 2021,1,26 entry-to-practice paramedicine programs were endorsed by the Council of Ambulance Authorities (CAA). 82 This review identified that the majority of sources (68%) were published prior to paramedic registration occurring. 26 While the introduction of paramedic registration impacted both industry and the tertiary education sector, it is not evident that this change has improved the quality of placement experiences. This is despite the Paramedicine Board's accreditation standards 2.10 and 3.13 highlighting the importance of quality on clinical placements. 1 Sources included pre and post-registration highlights that highlight the same barriers and facilitators.
Limitations
In interpreting the findings of this review, several methodological and contextual limitations should be considered. Articles published in languages other than English were excluded to avoid the need for transcribing, which may have resulted in the omission of potentially relevant studies. It is unlikely that exclusions due to language were relevant, as the focus was on paramedicine students undertaking placement as part of an Australian degree program. Additionally, it is acknowledged that the terms ‘placement’ and ‘supervisor’ have various interpretations and definitions. Although the search strategy attempted to encompass these variations, it may not be exhaustive. Some included articles utilised low participant numbers. Reasons for this were that diverse placement settings are often seen as ‘novel’, allowing only a small number of student participation, and the lack of a valid and reliable tool within paramedicine to evaluate the quality of student placements. Taken together, these limitations do not diminish the value of the review but highlight areas where further, more methodologically robust research is needed, providing an important context for the recommendations below. Finally, it must be noted that following the introduction of paramedic registration in 2018, changes were seen in both the industry and the tertiary education sector, including the expectations of supervisors and placement experience.
Recommendations
This review has synthesised the available literature, and several quality measures have been identified. These recommendations are a shared responsibility between tertiary institutions, placement providers and accrediting agencies.
Supervisors, whether ambulance paramedics or others, should be encouraged to possess the attributes of being well prepared, welcoming, supportive, accommodating of student involvement, and able to create a safe and encouraging learning environment. Supervisors should be appropriately trained to supervise students. Supervisors should be alert to instances of physical and psychological abuse of students and respond appropriately. Placement experiences should be structured so that students have specific learning outcomes and activities to ensure opportunities for learning. This includes students being provided with ‘hands on’ experience, actively involving them in patient care or scenarios. Adequate logistical preparation is required prior to placement, including appropriate allocation of students to supervisors, early notification to supervisors, and clear communication on students’ learning outcomes and scope of practice. Placement providers should provide students with training and resources specific to the setting, including adequate orientation. Consideration should occur for students to attend a combination of rural and metropolitan locations to accommodate for diversity in experiences, case load and learning opportunities. Educational providers and government should provide financial assistance to paramedicine students to cover costs associated with placement, particularly in rural locations. All students should have the opportunity to participate in non-traditional paramedic-based placements, including in-hospital, and community settings. To facilitate this, clear expectations, learning activities and adequate preparation of students and supervisors are essential. Placements should have continuity, including placements of longer duration and consistent supervisors. A valid and reliable quality assessment tool should be developed, specific for the paramedicine student placement context, to allow for evaluation of quality placement experiences.
It is identified that some of these recommendations are noted in the Paramedicine Board of Australia's Professional Capabilities for Registered Paramedics 76 and Accreditation Standards 1 ; however, their reporting and application across settings are inconsistent. These 11 recommendations derived from content analysis of the included sources align with the five factors previously identified, which enable quality placement experiences for health students, 5 and the four domains of quality clinical practice within higher education. 25
Conclusion
This review offers insight into the factors which influence quality paramedicine student placements. Four primary categories of factors that influence quality paramedicine student placements have been established, namely the impact of supervisors, the types and quality of learning experiences, the setting and structure of placement, and student satisfaction. These factors are indicators of quality, which should be established in all paramedicine student placement experiences. Considerable heterogeneity exists within the literature regarding students’ current experience of quality. This suggests there needs to be a more standardised and meaningful approach to the structure of placement experiences to ensure quality is achieved and maintained. Furthermore, no valid and reliable tool was found within the literature to measure quality in paramedicine placements. To improve and maintain the quality of paramedicine student placements, a united and collaborative approach is required by all stakeholders involved, particularly if poor quality indicators likely impact on graduate outcomes. Only via clear placement standards can stakeholders ensure quality can be measured and achieved, allowing for national placement benchmarking to occur and aiding in developing strategies to improve the paramedicine student placement experience.
Supplemental Material
sj-docx-1-pam-10.1177_27536386261461782 - Supplemental material for Factors that influence quality student paramedicine placements in Australia: A scoping review
Supplemental material, sj-docx-1-pam-10.1177_27536386261461782 for Factors that influence quality student paramedicine placements in Australia: A scoping review by Ashleigh Finn, Caitlin Fitzgibbon, Brendan Shannon, Kelli Innes and Cameron M Gosling in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386261461782 - Supplemental material for Factors that influence quality student paramedicine placements in Australia: A scoping review
Supplemental material, sj-docx-2-pam-10.1177_27536386261461782 for Factors that influence quality student paramedicine placements in Australia: A scoping review by Ashleigh Finn, Caitlin Fitzgibbon, Brendan Shannon, Kelli Innes and Cameron M Gosling in Paramedicine
Footnotes
Acknowledgements
We would like to acknowledge Anna Stokes, Librarian at Monash University, for their support with developing the search strategy.
Ethical approval and informed consent statements
There are no human participants in this article, and informed consent is not required.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
Brendan Shannon is an Associate Editor for Paramedicine. He played no role in the editorial decision making, which as conducted in adherence to the journal's editorial policy.
Data availability statement
Not applicable
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.