
Abstract
A good health financing system is crucial for the effective performance of a country's health system. Many health systems around the world, especially in lower- and middle-income countries such as Nigeria, grapple with perennial challenges such as chronic underfunding, wastefulness, and lack of accountability rendering these systems inefficient. Nigeria's health system faces additional extraneous challenges such as a huge and rapidly growing population, a stagnant economy, and worsening insecurity of lives and property. Furthermore, recent disease outbreaks such as the Ebola epidemic and the COVID-19 pandemic and an evolving disease demography evidenced by an increasing prevalence of chronic, noncommunicable diseases asphyxiate an already floundering health system. To address these challenges and to bolster its efforts in attaining universal health coverage (UHC) and meeting the targets of the Sustainable Development Goals, the Nigerian government launched a new health policy in 2017. A review of the health financing section of this policy shows a focus on improving funding for health care by all levels of government and guaranteeing affordable and equitable access to health services by all Nigerians, albeit with insufficient clarity on how these will be achieved. A more critical review of the country's health financing system also reveals deep-seated systemic issues. Its out-of-pocket payments for funding health care are among the highest in the world, with abysmally low government contributions to health. Successive governments seem to lack the political will to address these shortfalls. Critical gaps exist in the country's health laws, making it difficult to implement the strategies proposed in the new policy. Nigeria must strengthen its health laws to, among other things, mandate health insurance and provide adequate funding for the health system by the government. It should also formulate a dedicated, more precise health financing policy with specific, measurable aims targeting identified problems to enable it to attain universal health coverage.
Why is Financing Important?
Deliberations on health systems often focus on how health care should be financed because a good health care financing system ultimately determines the overall performance of the health system and the health outcomes of a nation. 1 More so, a good health care financing system is essential for achieving universal health coverage (UHC). 2 Health system reforms, therefore, are often targeted at strategies that improve health care financing, such as increasing health funding or improving the efficiency of health expenditure, so that health care is made affordable and accessible for every member of the society.
Health financing policy debates are often contentious because they deal with the allocation and expenditure of scarce national resources in the health sector. In lower- and middle-income countries (LMICs), the health sector is often neglected as it competes with other sectors of the economy for the allocation of these resources. This competition is even stiffer when other factors—such as the particular political and social economies, power structures, and political ideologies, such as plutocracies—in these environments are taken into cognizance. In many of these countries, the health sector grapples with chronic underfunding, misappropriation of resources, lack of transparency, poor accountability, and corrupt practices. Ultimately, the health system is weakened, and the citizens bear the brunt.
Despite constituting over three-quarters of the world's population and bearing over 90 percent of the global burden of disease, only a tenth of total global health expenditure is spent in LMICs. 3 The strain on these health systems has become untenable in recent times as the burden of disease shifts from communicable to noncommunicable and chronic diseases. With the outbreak of the COVID-19 pandemic in 2020, these already strained and fragile health systems were stretched to breaking points. This article critically analyzes the health care financing system of Nigeria, an LMIC in sub-Saharan Africa. Specifically, it reviews the most recent national policy on health care financing in the country, the National Health Policy 2016 (“the policy” or NHP 2016).
Contextual Background: Nigeria
Overview and Population
Nigeria is currently the world's sixth most populous country and the most populous in Africa. 4 With a population growth rate of 2.5 percent, one of the fastest in the world, it is forecasted to become the third most populous country in the world by 2050.4,5 Over 90 percent of its population are aged 54 years and below, making it one of the youngest in the world. 4
This rapid growth rate has significant implications for the country's health system. Currently, there are no policies in place to check this impending population explosion. 4 Rather, staggering poverty levels amid a stagnant economy, worsening insecurity of lives and property, massive internal displacements, high levels of illiteracy, and a lack of political will to address any of these problems exacerbate an already grave situation. 6
Government and Governance
Nigeria practices a democracy with a federal system of government consisting of 36 states and a Federal Capital Territory. Power is shared between three tiers of government: federal, state, and local, albeit unequally, with the central, federal government retaining much of it. 7 The health sector is concurrently administered by all three tiers of government. 8 The extent to which each tier of government contributes to the administration and funding of health care in the country varies considerably and determines how health is accessed and purchased in different parts of the country.
Economy
Nigeria is Africa's largest economy, heavily endowed with deposits of natural gas and crude oil.4,9 However, because of the volatility of these products in the international market and the country's heavy dependance on them, its economy is labile. Economic recovery has been slow since the global oil crash of 2016. Successive governments have failed in their efforts to diversify the economy. Poverty remains rife, with unemployment and inflation rates in double digits.9,10
Health Care Delivery
Health care delivery in Nigeria is pluralistic through both orthodox (or conventional) and traditional providers. 11 Although both coexist, there is little integration and collaboration between the two. 11 A large proportion of the population accesses health care through traditional or complementary health care providers, but extant laws are weak. 12 The orthodox system, on the other hand, comprises primary, secondary, and tertiary health centers administered by both public and private health care providers.11,13 The primary health care (PHC) system is designed to be the cornerstone of health care delivery in the country and constitutes about 85 percent of health centers, but these are poorly run.11,13 The private sector provides up to 60 percent of health services in the country. 11
The responsibilities of each tier of government in funding and administering health care are not clearly defined by the constitution. 13 However, the NHP ascribes responsibilities for primary, secondary, and tertiary health care to local, state, and federal governments, respectively. 11 The boundaries are nonetheless imprecise. For instance, the National Primary Health Care Development Agency that administers PHC in the country is managed by the federal government. 11
The Nigerian Health System: Where the Problem Lies
The Nigerian health system has been described as “weak and inefficient,” performing poorly across all the building blocks of a health system and ranking low among other health systems.13–16 It is besieged by numerous challenges such as poor governance and infrastructure, wastefulness, poor access to health care, absence of financial risk protection, depleting health workforce, and low quality of care, compounded by the lethargic political will to address these. 13
Despite hosting the often-cited Abuja declaration of 2001, a conference of African presidents where it was resolved to allocate a minimum of 15 percent of their annual national budgets to the health sector, Nigeria has persistently fallen far short of this benchmark. Two decades later, the highest budgetary allocation to the health sector was 7.28 percent in 2018, less than half of the benchmark. 17 In contrast, South Africa allocated 13.3 percent (almost double Nigeria's) in the same year. Similarly, in the West African sub-region, the Nigerian government's allocation to the health sector ranks among the lowest. 18
Furthermore, compared to other African economic powerhouses, South Africa and Kenya, whose government funding of health is almost two-thirds and half of total health funding (62% and 47%), respectively, the Nigerian government's contribution to health is only 15 percent. 19 In the context of being Africa's largest economy, these statistics are incongruous.
The national health indices reflect a grim picture. Life expectancy at birth is currently 62.6 years, significantly lower than the global average of 73 years. 20 The maternal mortality and under-five mortality rates are among the highest in the world.21,22 Steep inequalities in health outcome also exist between the upper- and lower-income earners, urban and rural dwellers, and southern and northern regions of the country. 13
On the positive side, the timely control of the Ebola virus outbreak in 2014 and the interruption of wild polio virus transmission in the country are laudable achievements by the health system. 13 A rapid national response to the COVID-19 outbreak is also commendable.
Rationale for a Policy Review
The above background paints a picture of a health system in need of attention. Chronic underfunding and the absence of a universal health insurance system are largely responsible for the poor state of the health system. 15 Not uncommonly, households slip into poverty as a result of catastrophic expenditures on health. 23 Nigeria's case is unique because of its large and fast-growing population, high level of insecurity of lives and property, high poverty levels, and stagnant economy.
The 1999 federal constitution, which regulates the health sector, is silent on how health should be administered and funded in the country. It does not clearly delineate the roles and responsibilities of each tier of government in the health sector and does not mandate specific budgetary allocations for the health sector. The National Health Act of 2014 also failed to address these gray areas. 13 A new NHP titled “Promoting the Health of Nigerians to Accelerate Socioeconomic Development,” with a section on health care financing, was formulated in 2016 with a focus on achieving UHC in the country. A quick search of major databases such as PubMed, Medline, and Google Scholar did not show any recent studies that holistically reviews this policy.
Aims of the Policy Review
This article reviews the health financing section of the NHP 2016. Specifically, it examines how health care is funded in Nigeria and how these funds are pooled, allocated, and utilized in the health sector. It analyzes these health financing themes in the context of the current political and economic climate in the country and compares it with other countries, especially those that have attained UHC. It concludes by recommending ways of improving the country's health financing system.
Methods
Methodology/Design
A comparative-case study approach as described by Walt and colleagues (2008) is employed in analyzing the policy, with Nigeria as the “case,” and selected countries (chosen based on demographic, political, economic, and geographical similarities with Nigeria) as the “comparison”. 24 Where appropriate, more developed health systems are referenced to illustrate wider issues.
Framework
The policy triangle framework as postulated by Walt and Gilson (1994) is used as a framework for reviewing the policy (Figure 1). 25 The context represents the socio-political climate in which the policy was formulated (“where/when”), the actors are the key stakeholders involved in formulating the policy (“who”), the process is the mechanism and strategies employed in formulating the policy (“how”), and the content is the subject matter and constitution of the policy (“what”). The content is discussed in three thematic sub-headings: revenue generation, pooling and allocation, and expenditure.
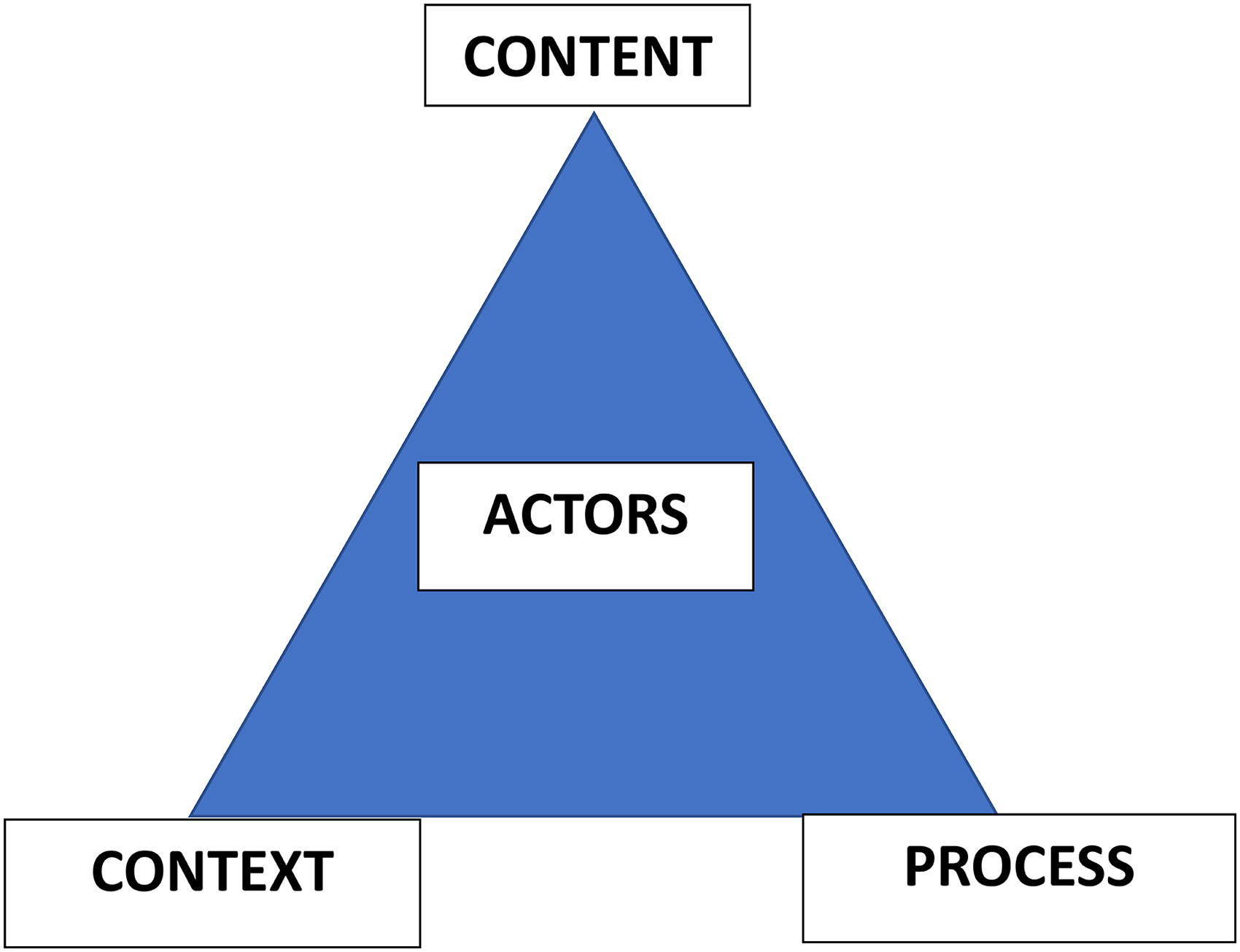
Policy triangle framework. 25
Data Gathering and Analysis
The key document reviewed in the analysis is the health care financing section of the NHP 2016. Other supporting data were sourced from a scoping review of relevant literature from PubMed, Medline, and Google Scholar. Relevant health indices and statistics were collated from the World Health Organization (WHO) Global Health Observatory Repository.
Policy Analysis
Policy History
The first comprehensive national health policy in Nigeria was launched over three decades ago in 1988 and revised in 2004. Both policies were crucial in laying the foundations for the fledgling health system. Following the revision in 2004, a National Health Financing Policy was formulated in 2006 aimed at making health care more accessible and affordable in the country. 13 Other attempts were made to further strengthen the health system, such as two national health summits in 1995 and 2014, respectively, with an aim to attain the requirements of the Millennium Development Goals (MDGs), especially achieving UHC and financial risk protection. 13 Unfortunately, none of these materialized into a stronger and more resilient health system.
Policy Process
Following recent global health trends, such as the increased traction toward UHC, especially in LMICs; the transition from MDGs to Sustainable Development Goals (SDGs); an evolving disease demography evidenced by an increase in the prevalence of chronic noncommunicable diseases; and recent epidemics, such as the Ebola virus outbreak of 2014, it became imperative to formulate a new national health policy to strengthen the health system. More so, local conditions such as an unstable economy, rising poverty level, a burgeoning population, and worsening insecurity of lives and property dictated that this policy update was urgent.
A National Health Act was enacted in 2014, creating a convenient legal milieu for the much-needed national health policy. As anticipated, the NHP with a section on health care financing was formulated in 2016 and launched in 2017.
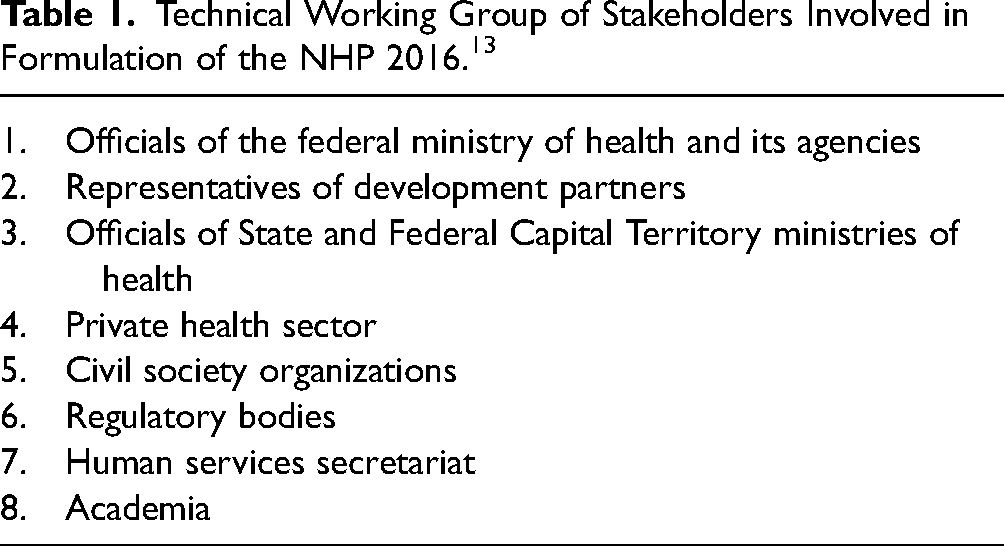
The NHP 2016 was initiated by the Federal Ministry of Health in collaboration with other stakeholders (Table 1). Two meetings of the technical working group were held in January 2015 and February 2016 and resulted in a final draft of the policy. 13
Technical Working Group of Stakeholders Involved in Formulation of the NHP 2016. 13
Policy Actors and Stakeholders
The NHP 2016 was formulated by collaborative efforts between relevant stakeholders and the Federal Ministry of Health (Table 1). A more extensive list of stakeholders for the implementation of the policy is listed in the policy document. 13
Policy Context
Health care financing and the overall development of the health sector do not appear to be front-burner issues in Nigeria's political discourse. At least, this was the feeling in the run-up to the general elections in 2015, when health-sector reforms were conspicuously absent in the campaign manifesto of the major political parties in the country (the All-Progressives Congress and the People's Democratic Party).26,27 On assumption of office after victory at the polls, health-sector reform was again not included in President Muhammadu Buhari's key administrative agenda. Well into his second term in office, in January 2022, the President constituted a health-sector reform committee. The outcome of this committee's work is awaited. 28
The NHP 2016 was formulated one year into his tenure against a backdrop of a lackluster health system challenged by poor funding by all levels of government, unaffordability of health services, and low acceptance of health insurance by the populace. The socio-political landscape in 2016, when the NHP was formulated, was characterized by endemic corruption in the health sector and a dissatisfied health workforce leading to incessant strike actions, as well as other aforementioned factors.
Policy Content
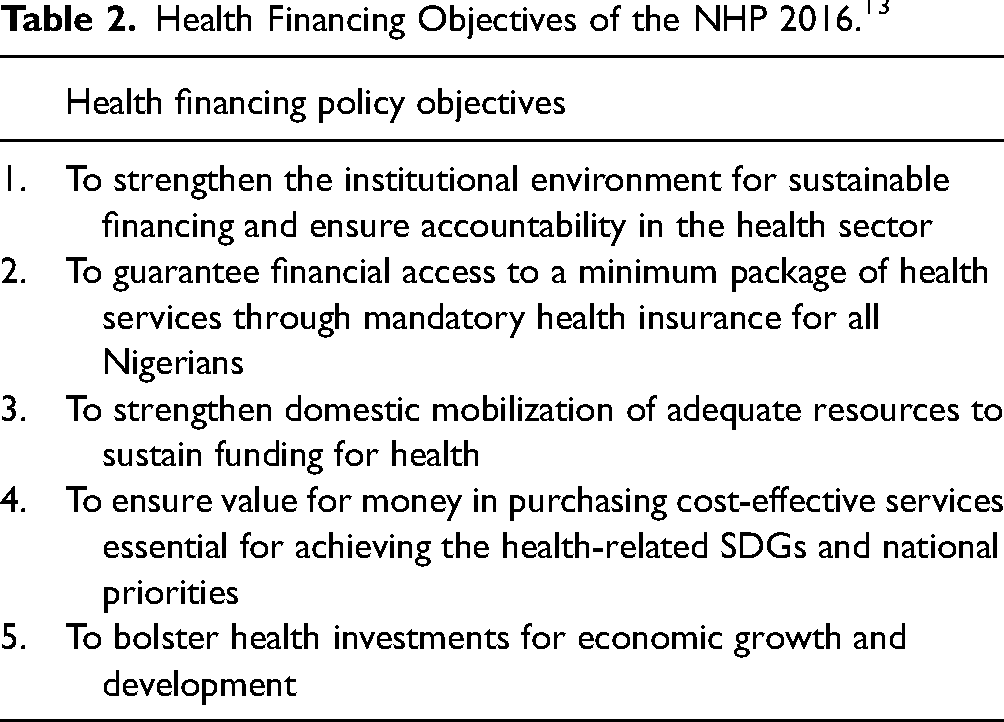
The content of the health financing section of the NHP 2016 will be discussed in three thematic subheadings: revenue generation, pooling, and expenditure. The overarching goal of the NHP 2016 is to ensure quality and affordable health care for all citizens. Health care financing is one of the 10 thrusts of the policy and seeks to ensure adequate funding for the health sector, equitable access to health services, and financial risk protection for the poor and vulnerable (Table 2). 13
Health Financing Objectives of the NHP 2016. 13
Revenue Generation
Funding for health care in Nigeria is generated through four major sources: government funding through budgetary allocations to the Ministry of Health; direct out-of-pocket payments by health service users at the point of care; health insurance prepayments, including social, community-based, and private schemes; and external funding from donor agencies (Figure 2).23, 29–32
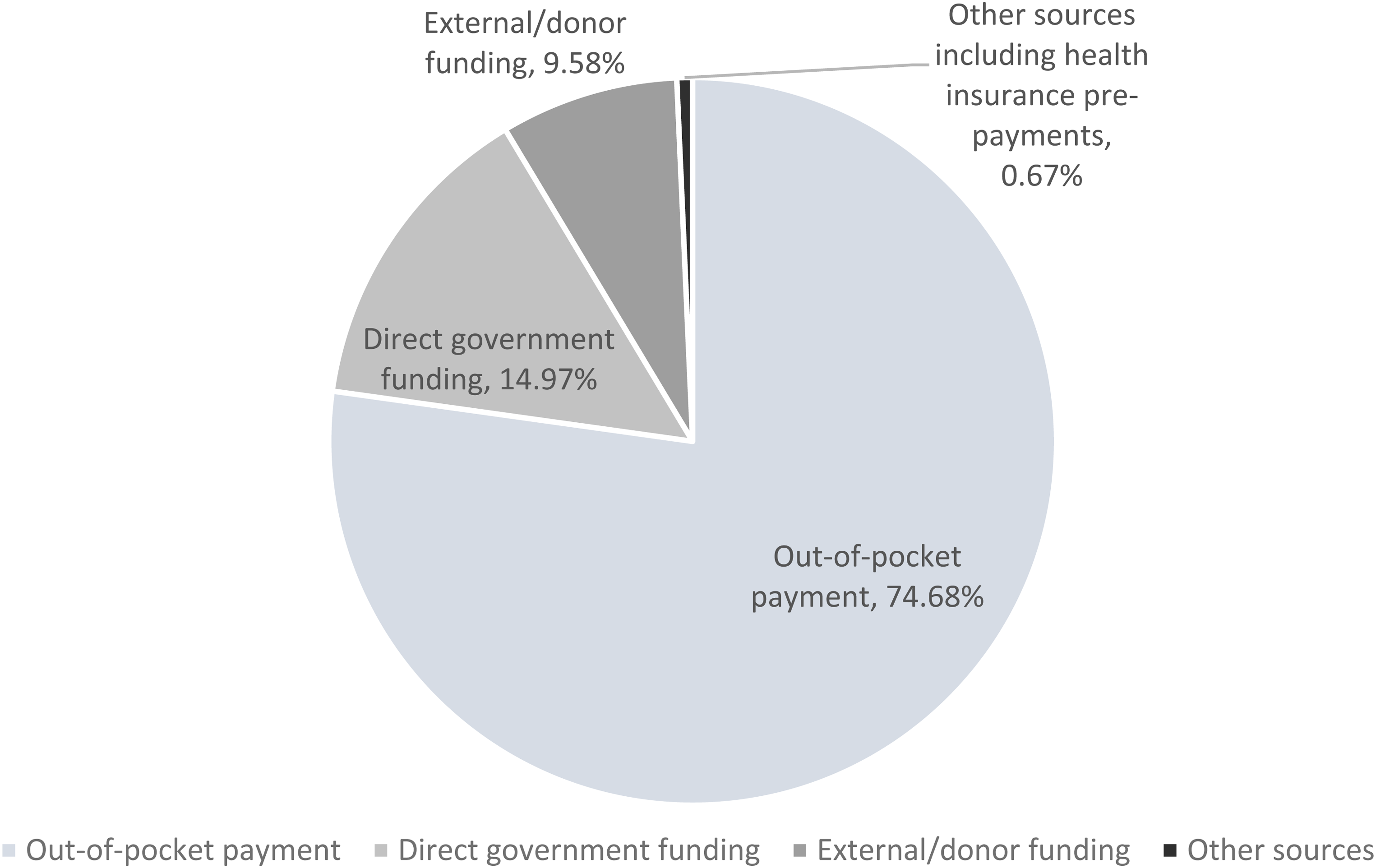
Proportion of revenue generation for the Nigerian health sector from different sources (2020 data, extracted from WHO global health observatory data Repository 32 ).
The Nigerian government's allocation to the health sector is among the lowest in Africa (Figures 3 and 4), while out-of-pocket payment for purchasing health services is among the highest in the world (Figure 5).17,19,33 This is clearly an unsustainable model of health care financing and stands the risk of catastrophic health expenditures and inaccessibility to health services among a significant proportion of the population.

Proportion (in percentage) of government's contribution to total health expenditure in some African countries (2020 data, extracted from WHO global health observatory data repository 19 ).
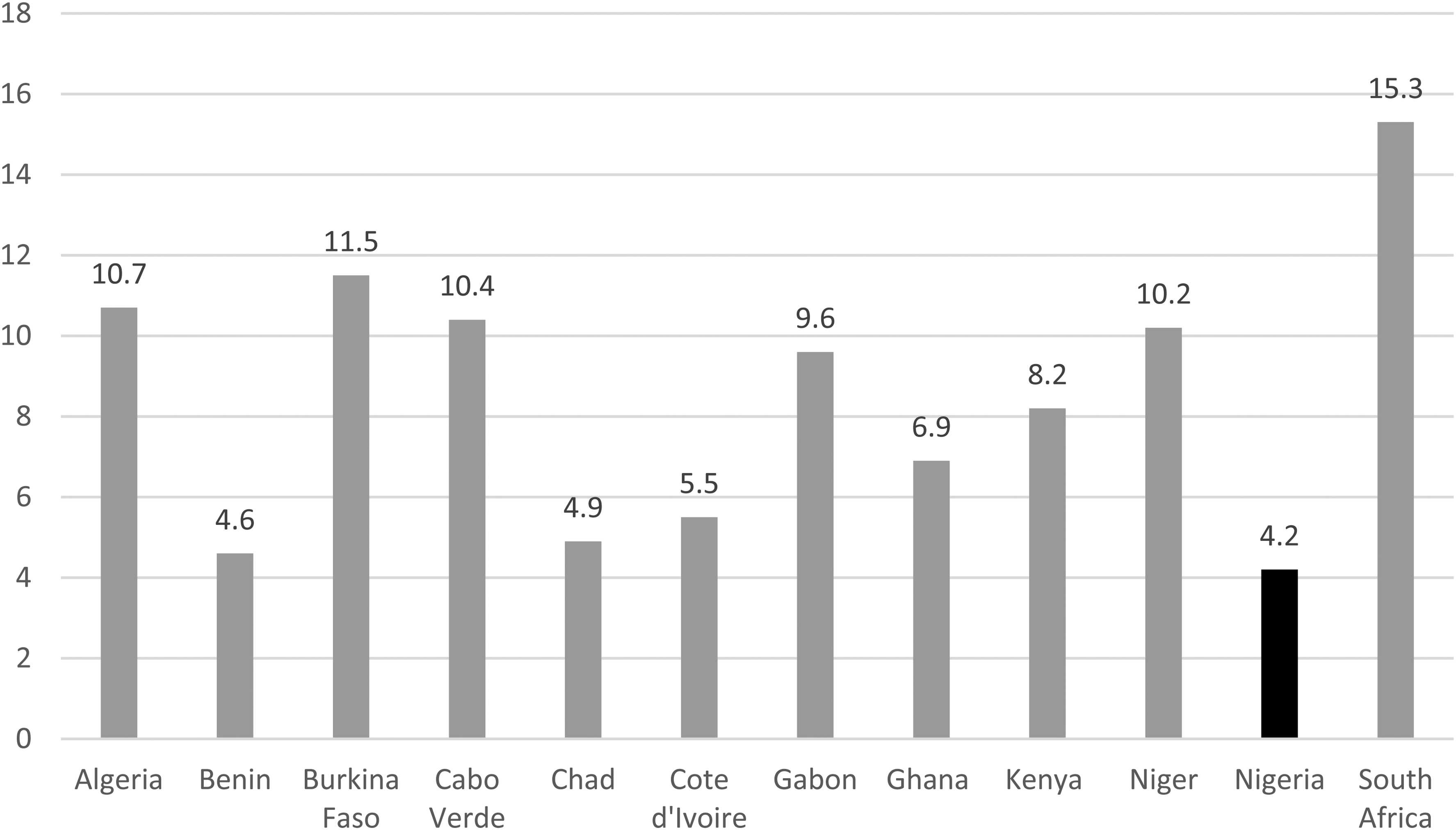
Some African governments’ contribution to health as a proportion (in percentage) of total government expenditure (2020 data, WHO global health observatory data repository 17 ).
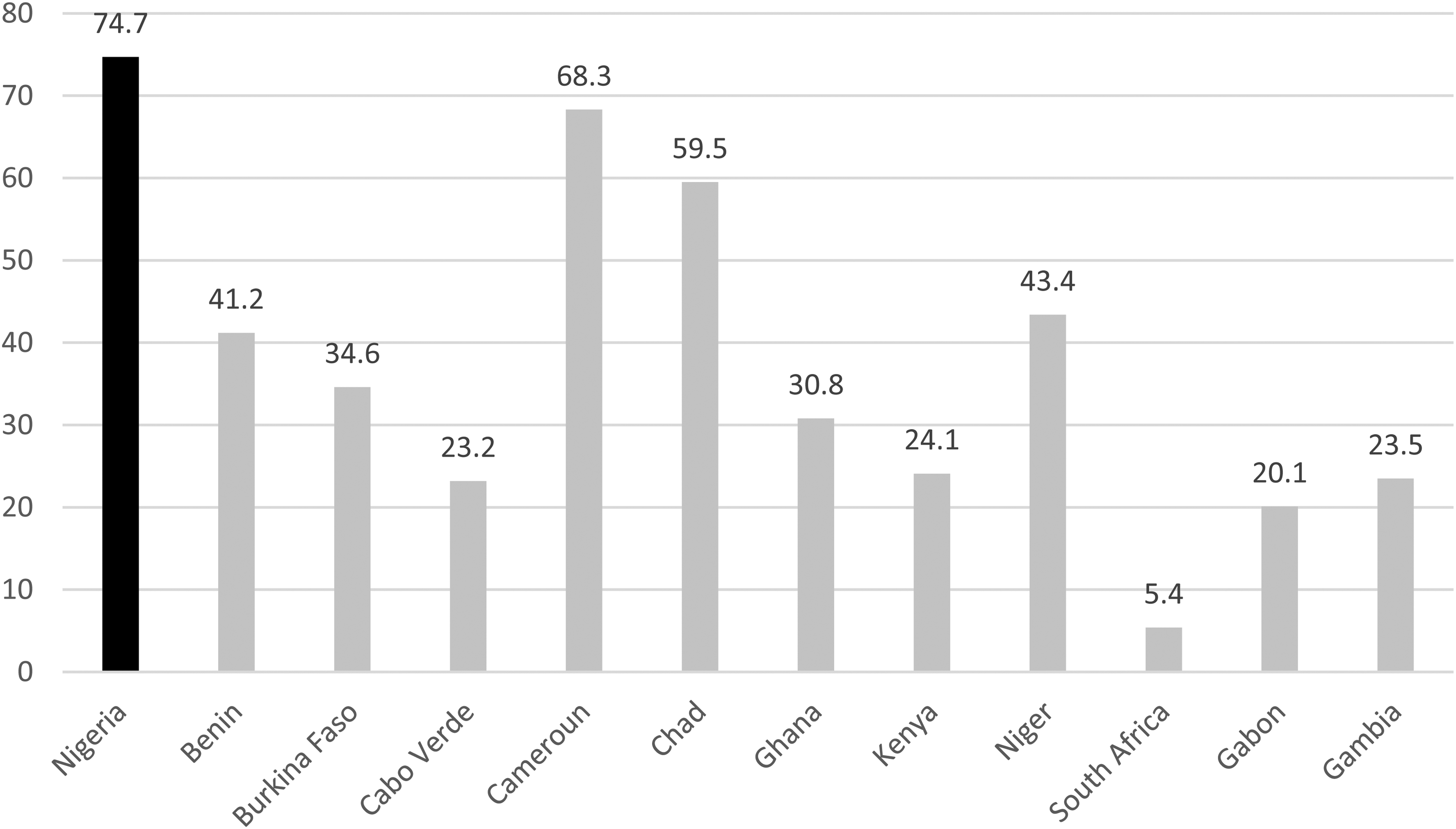
Out-of-pocket payment in some African countries as a proportion (in percentage) of total health expenditure (2020 data, WHO global health observatory data repository 33 ).
Policy Goals on Revenue Generation
The NHP 2016 aims to increase health funding by advocating for increased budgetary allocation to the health sector by all levels of government; exploring additional sources of revenue generation, such as earmarked taxes on alcohol and tobacco, aviation, value-added tax, and telecommunications; and promoting the revision of the act setting up the National Health Insurance Scheme (NHIS) to make it mandatory for all Nigerians. 13
Revenue Pooling and Allocation
Since most of Nigeria's health expenditure is sourced from out-of-pocket payments, pooling is managed individually by households. Other sources of health funding also pool their revenues separately, making it difficult to accurately analyze. For instance, there is no central pooling mechanism for external donors who prefer to donate directly to the health programs or government agencies they wish to fund. 30
The contribution of the federal government to the health sector is pooled in the federation account and disbursed quarterly to the Ministry of Health through the finance ministry and the Central Bank. 30 However, a new pooling mechanism called the Basic Health Care Provision Fund (BHCPF) was recently instituted as a provision of the National Health Act 2014. The fund aims to avail a basic minimum package of health services (including preventive, protective, promotive, curative, and rehabilitative) to all Nigerians by pooling health resources from an annual grant from the federal government of “not less than” 1 percent of the Consolidated Revenue Fund (a federal government-owned account where all its revenues are paid), counterpart funding from the state governments, grants by international donor agencies, and funds from “any other sources” (not specified).1,23 The federal government's contribution to the BHCPF was captured for the first time in the 2018 national budget, where 55 billion Nigerian Naira (US$152 million at the then-exchange rate) was approved by the federal legislature for payment into the fund. 34
Allocations from the BHCPF are to the NHIS (50%), the National Primary Health Care Development Agency (45%), and the National Emergency Medical Treatment Committee (5%) for achieving UHC, strengthening PHC, and treating medical emergencies, respectively. 34
Health insurance is also a type of pooling mechanism, and ensures equitable and affordable access to health care for all members of the society. 23 Three main modalities are in operation in Nigeria: social health insurance through the NHIS, community-based health insurance, and private health insurance. Their uptake and penetration in the country remain low. Since its launch in 2005, only 5 percent of the population, mainly employes of the federal government, are covered by the NHIS.23,35 In 2017, it contributed less than 1 percent to total health expenditure. 29 Contributions from community-based and private health insurance in the country are also meager. Less than 1 percent of the population own private health insurance. Community-based insurance models have failed to be upscaled and sustained across the country. 23
Policy Goals on Revenue Allocation and Pooling
The NHP 2016 initiatives on improving revenue allocation and pooling include facilitating budgetary provisions for the BHCPF, streamlining the different health insurance mechanisms in the country into one pool at the federal level and one in each state, and pushing for mandatory enrollment into the NHIS by all Nigerians. 13
Expenditure
Most (over 70%) of Nigeria's expenses on health care are spent on purchasing health goods (such as medicines) and services through out-of-pocket payments by individuals at the point of care.30,36 Grants and aids from donor organizations and charities are often spent on preventive services such as the Global Alliance for Vaccines and Immunization and the Bill & Melinda Gates Foundation, whose focus includes polio eradication and reduction of child and maternal mortality.
Most of the government's expenses on health care are on recurrent expenditures (such as payment of salaries) and overhead or administrative costs (such as purchase of office supplies), rather than on capital projects, such as building new hospitals or purchasing new medical equipment, that lead to more appreciable improvements in health service delivery. 37 In the 2019 national budget of the federal government, 84.7 percent of the total health-sector budget was allocated for recurrent and administrative expenses while 15.3 percent was allocated for capital projects. 38
Policy Goals on Health Spending
The NHP 2016 is silent on how funds should be spent in the health sector. 23 Its health spending policy goals include eliminating inefficiencies, improving accountability in health spending, and promoting strategic purchasing mechanisms. 13 It lacks specific details on how these are to be achieved or what the monies are to be spent on.
Discussion
Nigeria, like every other country, funds its health system from multiple sources. However, the heavy reliance on out-of-pocket payments, an unsustainable and inequitable method of financing health care, is impoverishing. 30 No meaningful progress can be made in developing a health system using out-of-pocket payments.
A plausible explanation for the Nigerian government's poor funding of health care is the sheer lack of political will to do so. Successive governments have paid only lip service to improving health care financing in the country despite juicy campaign promises.
The rising spate of insecurity of lives and property in the country, which has direct and indirect consequences on health care funding, aggravates the situation. Worsening insecurity means more funding for the defense forces at the expense of other sectors such as health. In the proposed 2022 budget, the defense and internal policing allocation was about a quarter of the total budget, while health sector allocation was only roughly 4 percent. Other sequalae of insurgency, such as internal displacements, unemployment, poverty, and hunger, worsen health care financing by straining the health system further.
The NHP 2016 is ineffective in several aspects. It fails to provide clear guidance on how to improve health funding in the country. Although alternate sources of health funding are suggested in the policy, it does not specify targets and timeframes for achieving this, making further evaluation of the policy difficult in the future.
The NHP 2016 is also advisory at best. The language of the policy, such as “advocate,” “explore,” “facilitate,” and “promote,” is mostly suggestive rather than cogent. The policy lacks SMART (specific, measurable, achievable, realistic, timebound) aims and objectives. Health laws are also weak in the country. The National Health Act 2014 failed to enact strong health financing laws. Apart from Section 11 of the Act, which establishes the BHCPF, no other part addresses the inadequacies in health care financing in the country, such as mandating health insurance or statutory government allocations to the health sector at all levels.
Nigeria also faces huge problems with expenditure in the health sector and little analysis has been done in this regard. Most of the Nigerian government's expenditure on health care goes into recurrent expenses, as mentioned earlier. 39 The NHIS is poorly funded: 1.1 percent of the total health capital expenditure or 0.2 percent of the total health budget was allocated to the scheme in 2019. 38 Clearly, this mode of expenditure cannot address the country's high out-of-pocket payment and the prospects of achieving UHC.
China's example may be useful to Nigeria. China has similar socio-demographic structures (a huge population and a large informal sector) as Nigeria. It adapted its health spending to reflect changes in its population and disease burden by changing its expenditure from directly subsidizing government-run health providers to providing subsidies for households to enroll in social health insurance. That is, moving from subsidizing the “supply” side to the “demand” side of health care. 40 The long-term result was a dramatic increase in life expectancy from 35–40 years in 1949 to 77.4 years currently.20,40 In more recent years and with a steady push to achieving UHC through strategic spending and mandating health insurance, China reduced its out-of-pocket payment by almost 100 percent (60% to 35.9%) in less than two decades (2000 to 2016) and quadrupled its health insurance coverage (22% to 95%) in one decade (2003 to 2013). 41
Conclusion and Recommendations
The immediate conclusion from the discussion above is a health system neglected by the government at all levels, evidenced by the heavy dependence on out-of-pocket payment for funding health care. In addition, expenditure of scarce health resources is inefficient and does not reflect a system intent on achieving UHC. Risk pooling is almost nonexistent as only 6 percent of the population have a form of health insurance, a far cry from requirements for UHC. There are no signs in place to show that this trajectory is about to change. The NHP 2016 has been unable to bridge the wide gaps in health funding deficiencies and health spending inefficiencies. The policy is nonspecific on strategies and mechanisms to improve health care financing in the country.
Perhaps what Nigeria needs more urgently is a strong health care financing law (such as seen with the BHCPF) rather than a policy, that will compel the government as well as the citizens into action. At the time of concluding this manuscript, it was announced that the Nigerian president has signed a National Health Insurance Authority Act into law. 42 This act is expected to ensure compulsory health insurance for all Nigerians. The details of the law are still sketchy and not yet in the public domain.
A more concerted effort should be geared toward achieving UHC. Health insurance is currently optional for most Nigerians, hence the low penetration and poor buy-in. Evidence shows that no country has been able to achieve UHC with a voluntary health insurance scheme.43,44
A more focused health financing policy that is SMART should follow on the back of stronger health laws. The policy objectives should be specific and time-bound to enable continued re-evaluation of these targets. The health financing system should also be restructured with clearly defined sources of funding that are sustainable as well as efficient risk-pooling mechanisms.
In conclusion, a lack of political will, an undefined and unstructured system, and an absence of strong health laws are the most important factors responsible for Nigeria's poor health financing system. Systematic and bold strategies through erecting a strong system, setting measurable targets, and enacting health laws are key steps in re-engineering a system that would set the country on the right path to achieving UHC. As global health systems struggle to recover from the strain caused by the COVID-19 pandemic, the call to build stronger health financing systems has become even more dire.
Footnotes
Declaration
An expanded version of this review was submitted to the Department of Public Health, Torrens University Australia in fulfillment for the award of Master in Public Health to the first author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.