
Abstract
Background:
Therapeutic inertia is a significant challenge to optimal blood pressure control, resulting in prolonged exposure to high blood pressure and increased cardiovascular risk, especially among older patients in low- and middle-income countries.
Objectives:
The current study assessed the impact of interventions by pharmacists on the time to antihypertensive treatment intensification among older patients with uncontrolled hypertension in Northwest Ethiopia.
Design:
A multicenter prospective cohort study was conducted from January to July 2025 in three tertiary hospitals in Northwest Ethiopia.
Methods:
A total of 422 older hypertensive patients with uncontrolled blood pressure were enrolled and followed up either in the pharmacist-led care or usual care. The interventions by pharmacists included recommendations for treatment intensification, medication review, adherence, and resolution of drug-related problems. The primary outcome was time to antihypertensive treatment intensification. Kaplan–Meier survival analysis and Cox proportional hazards regression were employed to evaluate the time-to-event outcomes and factors.
Results:
Patients receiving pharmacist-led care experienced significantly faster treatment intensification than those receiving usual care, with a median time of 28 days versus 63 days. A higher proportion of patients in the pharmacist-led group achieved treatment intensification within 30, 60, and 90 days. Faster treatment intensification (adjusted hazard ratio (AHR) 2.18) was independently linked to pharmacist-led care. The intervention group showed greater systolic and diastolic blood pressure reductions, as well as a higher percentage of patients who achieved blood pressure control at follow-up. In addition, higher baseline systolic blood pressure was linked to faster intensification of treatment.
Conclusion:
Pharmacist-led interventions significantly reduced therapeutic inertia by accelerating antihypertensive treatment intensification and improving blood pressure control. Integrating pharmacists into multidisciplinary hypertension care may represent an effective and scalable strategy to improve hypertension outcomes in resource-limited settings.
Plain language summary
High blood pressure is common among older adults and can lead to serious health problems like stroke and heart disease if not properly controlled. Sometimes, treatment is not adjusted quickly enough when blood pressure remains high. This study followed 422 older patients with uncontrolled hypertension in three hospitals in Northwest Ethiopia. Patients who received pharmacist-led care had their medications adjusted much faster than those receiving usual care (28 days vs. 63 days). They also had greater reductions in blood pressure and more often achieved good blood pressure control. These findings show that involving pharmacists in hypertension care can reduce treatment delays and improve patient outcomes, especially in resource-limited settings.
Introduction
Hypertension is a major global public health challenge and a leading modifiable risk factor for cardiovascular morbidity and mortality. More than 1.28 billion adults worldwide are affected, with nearly two-thirds living in low- and middle-income countries. 1 Uncontrolled hypertension markedly increases the risk of stroke, ischemic heart disease, heart failure, and chronic kidney disease, resulting in substantial preventable premature mortality. 2 The burden is rising rapidly in sub-Saharan Africa due to population aging, urbanization, unhealthy lifestyles, and limited access to healthcare. 3 Ethiopia has a 15% to 30% prevalence of hypertension; however, despite the availability of efficient antihypertensive medications, blood pressure control is still subpar, especially in older adults and those with comorbidities.4 –7
One of the most important contributors to suboptimal BP (blood pressure) control is clinical (therapeutic) inertia, defined as the failure of healthcare providers to initiate or intensify antihypertensive therapy when treatment goals are not achieved. 8 Several studies have shown that antihypertensive treatment intensification is frequently delayed, even after repeated documentation of uncontrolled BP.9 –11 Such delays expose patients to prolonged periods of elevated BP, increasing the risk of stroke, myocardial infarction, renal failure, and all-cause mortality.12,13 Evidence from cohort studies in high-income countries indicates that the median time to treatment intensification often exceeds 6 months, with even longer delays observed in LMICs (low- and middle-income countries) due to fragmented care systems, workforce shortages, and limited follow-up mechanisms. 14 In Ethiopia, although uncontrolled hypertension is highly prevalent, there is limited empirical evidence assessing the timeliness of treatment intensification and its determinants.15,16
Pharmacist-led interventions have emerged as an effective strategy to improve hypertension management and reduce therapeutic inertia, particularly in primary care and resource-limited settings. Pharmacists can contribute by identifying uncontrolled BP early, conducting medication reviews, recommending treatment intensification, addressing drug-related problems, improving medication adherence, and providing patient education. 17 Task-sharing and collaborative care models that integrate pharmacists into multidisciplinary healthcare teams have been shown to improve medication optimization and clinical outcomes. 18 Meta-analyses and randomized controlled trials consistently demonstrate that pharmacist-led interventions significantly increase the proportion of patients achieving target BP and reduce systolic BP by approximately 5–9 mmHg compared with usual care.19 –21
In Ethiopia, doctors and nurses have typically been in charge of managing chronic illnesses, while pharmacists have historically been restricted to dispensing and inventory management responsibilities. 21 The National Strategic Action Plan for the Prevention and Control of Non-Communicable Diseases is one recent national health sector reform that acknowledges the growing role of pharmacists in maximizing drug use and enhancing treatment results. Pharmacist-led services, including pharmaceutical treatment management, patient counseling, and adherence support, may enhance BP control and medication adherence, according to new research from Ethiopian hospital settings.22,23 However, there are still a few prospective cohort studies assessing how pharmacist-led interventions affect clinical inertia and time to antihypertensive treatment intensification, two important quality indicators of hypertension care that reflect real-time clinical decision-making.24,25
Given the high burden of uncontrolled hypertension, the shortage of specialized healthcare providers, and the need for scalable and cost-effective interventions, evaluating pharmacist-led models is particularly important in the Ethiopian context. Therefore, this multicenter prospective cohort study aimed to assess the effect of pharmacist-led interventions on the timeliness of antihypertensive treatment intensification among older adult patients in Northwest Ethiopia. By generating real-world evidence on reducing therapeutic inertia, this study seeks to inform policy, support integration of pharmacists into chronic care teams, and strengthen team-based approaches to improve BP control and reduce cardiovascular risk.
Methods
Study setting, design, and period
A multicenter prospective cohort study was conducted in Northwest Ethiopia at three tertiary-level public hospitals: University of Gondar Comprehensive Specialized Hospital, Felege Hiwot Comprehensive Specialized Hospital, and Debre Tabor Comprehensive Specialized Hospital. These hospitals serve as major referral centers for their respective catchment areas and provide comprehensive outpatient and inpatient care, including chronic disease management services for older adult patients with hypertension.
The study employed a pharmacist-led intervention model aimed at improving the timeliness of antihypertensive treatment intensification among older adult patients receiving routine hypertension care. Eligible participants were prospectively followed to assess treatment intensification practices and related outcomes. The study was conducted over a seven-month period, from January 1, 2025, to July 2025.
Eligibility criteria
Patients 60 years of age or older who had been diagnosed with hypertension and had uncontrolled BP (systolic BP ⩾140 mmHg and/or diastolic BP ⩾90 mmHg) despite receiving antihypertensive medication were included in the study. Patients with secondary hypertension, insufficient medical records, critical illness, or incapacity to participate in follow-up, or refusal to give informed consent were excluded from the study.
Sample size determination and sampling techniques
The sample size for this multicenter prospective cohort study was 422 older adult patients with hypertension. The sample size was determined using the single population proportion formula, assuming a 50% proportion to maximize sample size, a 95% confidence level, and a 5% margin of error, with an allowance for potential loss to follow-up.
The study was conducted at three comprehensive specialized hospitals: University of Gondar Comprehensive Specialized Hospital, Felege Hiwot Comprehensive Specialized Hospital, and Debre Tabor Comprehensive Specialized Hospital. The total sample size was proportionally allocated to each hospital based on the average monthly number of older adult hypertensive patients attending follow-up clinics.
A consecutive sampling technique was employed in each study site, whereby all eligible older adult patients presenting to the hypertension follow-up clinics during the data collection period were enrolled consecutively until the allocated sample size for each hospital was reached. Group assignment was based on the current treatment paradigm at each study site (pharmacist-led care versus usual care), instead of using random assignment.
Data collection instruments, procedures, and quality control
Data were collected using a structured and pretested data collection instrument developed after an extensive review of relevant literature and international hypertension management guidelines. The tool was designed to capture sociodemographic characteristics, clinical and treatment-related variables, BP measurements, pharmacist-led intervention components, and timeliness of antihypertensive treatment intensification. During routine follow-up visits, data were collected using a structured and pretested tool through patient interviews, medical record reviews, and standardized BP measurements conducted by trained personnel.
BP was measured by trained healthcare professionals using validated and calibrated sphygmomanometers, in accordance with standard clinical guidelines. Measurements were taken after the patient had rested for at least 5 min in a seated position, and the average of two readings was recorded. Information on medication regimens, treatment adjustments, comorbidities, and laboratory findings was extracted from patient medical records using a standardized abstraction checklist.
Data collection was carried out by trained clinical pharmacists and nurses under close supervision. Prior to data collection, comprehensive training was provided to ensure a uniform understanding of study objectives, data collection procedures, and ethical considerations. The data collection tool was pretested on 5% of the sample in a non-study setting, and necessary modifications were made to improve clarity and consistency.
To ensure data quality, daily supervision and on-site monitoring were conducted throughout the data collection period. Completed questionnaires were reviewed for completeness and accuracy before data entry (Supplemental File). Double data entry and consistency checks were performed to minimize entry errors. Any discrepancies identified were resolved through cross-verification with source documents. Standard operating procedures were strictly followed across all study sites to maintain consistency and reliability of the collected data.
Statistical analysis
Data were entered, cleaned, and analyzed using the Statistical Package for the Social Sciences (SPSS), version 27. Descriptive statistics were used to summarize participants’ sociodemographic characteristics, clinical profiles, and treatment-related variables. Categorical variables were presented as frequencies and percentages, while continuous variables were summarized using means with standard deviations or medians with interquartile ranges, as appropriate.
The primary outcome was the time to antihypertensive treatment intensification, measured in days from the identification of uncontrolled BP to the initiation or escalation of antihypertensive therapy. Patients who did not experience treatment intensification during the follow-up period were considered censored at their last clinic visit.
Time-to-event analysis was employed because the primary outcome was the time from detection of uncontrolled BP to treatment intensification. Kaplan–Meier survival analysis was used to estimate time to treatment intensification, and differences between groups were compared using the log-rank test. Potential confounding variables were taken into account during the analysis by assessing baseline comparability between groups and incorporating clinically significant variables in the multivariable Cox proportional hazards regression model. Based on statistical significance in bivariable analysis and clinical relevance, variables were selected for the multivariable model. Factors associated with the timeliness of treatment intensification were evaluated using the Cox proportional hazards regression model. Variables with a p-value <0.25 in bivariable Cox regression analysis were included in the multivariable model.
Results were reported as crude hazard ratios (CHR) and AHR with corresponding 95% confidence intervals (CIs). To find variables associated with the time to treatment intensification while taking censored observations into account, Cox proportional hazards regression analysis was used. Schoenfeld residuals and graphical techniques were used to evaluate the proportional hazards assumption. To guarantee model stability, multicollinearity among independent variables was assessed using the variance inflation factor (VIF). A p-value <0.05 was considered statistically significant for all analyses.
Results
Baseline characteristics participants
Baseline characteristics of participants were well balanced between the Pharmacist-Led Care and Usual Care groups. The mean age was similar (67.8 ± 6.1 vs 68.1 ± 6.4 years, p = 0.62), with comparable proportions of females (55.9% vs 57.3%, p = 0.78) and urban residents (59.7% vs 57.8%, p = 0.69). Baseline BP, prevalence of stage 2 hypertension, diabetes mellitus, chronic kidney disease, and use of ⩾2 antihypertensive drugs were also similar between the two groups, with no statistically significant differences (all p > 0.05), indicating successful group comparability before the intervention (Table 1).
Baseline characteristics of older adult participants (N = 422).

SD: standard deviation; SBP: systolic blood pressure; DBP: diastolic blood pressure; mmHg: millimeters of mercury.
Antihypertensive drugs prescribed and intensified
Among the 422 participants, ACEIs (33.2%), CCBs (23.7%), and ARBs (21.3%) were the most prescribed drugs. Treatment intensification mainly involved dose increases or adding new agents, with the highest for combination therapy (19.0%), followed by CCBs (14.2%) and ACEIs (10.7%), reflecting guideline-based escalation for uncontrolled hypertension (Table 2).
Types of antihypertensive drugs prescribed and intensified (n = 422).

Types of pharmacist-led interventions
In the pharmacist-led group, the most frequent interventions were treatment intensification (79.6%) and adherence counseling (73.9%), with additional actions including resolving drug-related problems (57.3%), adding new agents (49.3%), and dose escalation (43.6%). Physician acceptance was high (91.7%), indicating effective collaboration (Table 3).
Types of pharmacist-led interventions (n = 211).

Outcome and time to antihypertensive treatment intensification
Pharmacist-led care led to faster and more frequent treatment intensification (median 28 vs 63 days, p < 0.001) and greater BP reductions (SBP −18.6 vs −10.4 mmHg; DBP −8.9 vs −4.7 mmHg), with more patients achieving controlled BP at follow-up (62.6% vs 40.8%, p < 0.001; Table 4).
Time to antihypertensive treatment intensification.

DBP: diastolic blood pressure; SBP: systolic blood pressure; HR: hazard ratio.
Kaplan–Meier curve for time to antihypertensive treatment intensification
The Kaplan–Meier curve shows that patients in the pharmacist-led group achieved treatment intensification faster and more consistently than usual care, with the probability of no intensification declining more rapidly over time (Figure 1).

Kaplan–Meier curve for time to antihypertensive treatment intensification among older adults.
Factors for the time to treatment intensification
After adjustment, pharmacist-led intervention (HR 2.18; 95% CI 1.74–2.74; p < 0.001) and higher baseline systolic BP (per 10 mmHg, HR 1.52; 95% CI 1.01–1.85; p = 0.03) were independently associated with faster antihypertensive treatment intensification (Table 5).
Cox proportional hazards regression for time to treatment intensification (N = 422).
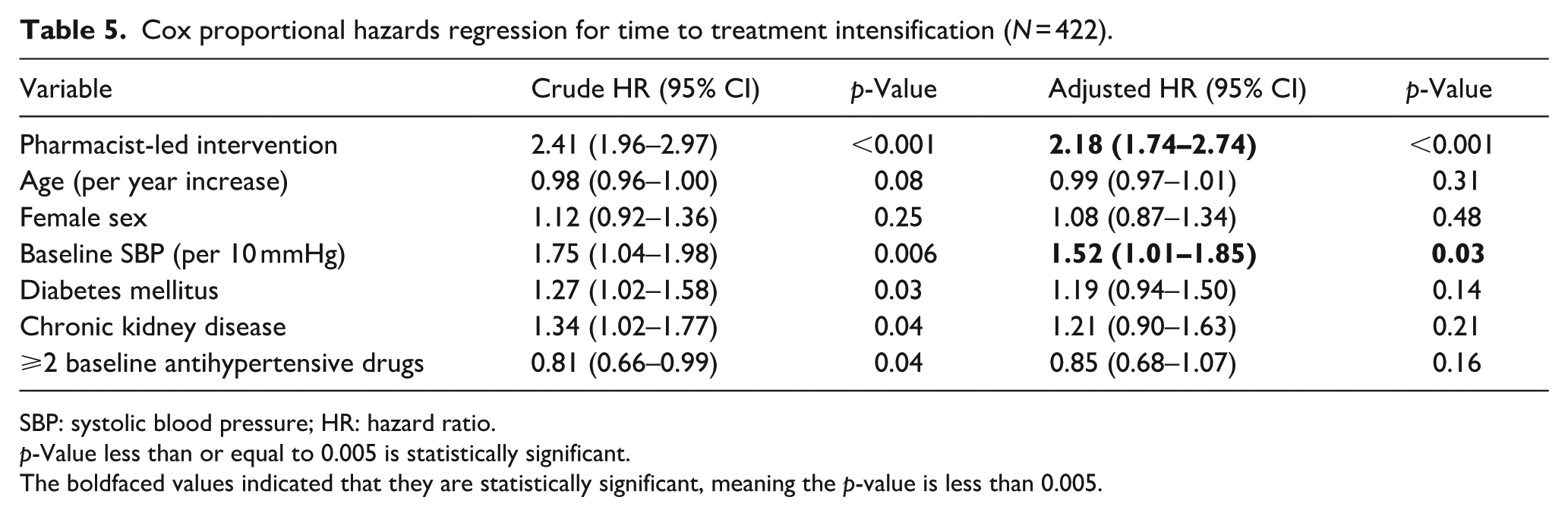
SBP: systolic blood pressure; HR: hazard ratio.
p-Value less than or equal to 0.005 is statistically significant.
The boldfaced values indicated that they are statistically significant, meaning the p-value is less than 0.005.
Pharmacist-led intervention and higher baseline SBP were significantly associated with treatment intensification, while other factors showed no significant association (Figure 2).

Forest plot of adjusted hazard ratios for timely antihypertensive treatment intensification among older adults.
Discussion
This multicenter prospective cohort study revealed that pharmacist-led interventions substantially improved the timeliness of antihypertensive treatment intensification among older adults with uncontrolled hypertension in Northwest Ethiopia. By reducing delays in treatment escalation, pharmacist involvement directly addressed therapeutic inertia, a well-recognized barrier to effective hypertension control worldwide, particularly in LMICs.3,26,27
Therapeutic inertia remains a persistent challenge in hypertension care and is associated with prolonged exposure to elevated BP and increased cardiovascular risk. Previous studies have consistently reported delayed treatment intensification despite repeated documentation of uncontrolled BP, reflecting gaps in clinical decision-making and follow-up systems.9,11,28,29 In resource-limited settings such as Ethiopia, high patient load, limited consultation time, and workforce shortages may further exacerbate this problem.16,25,30
The faster treatment intensification observed in the pharmacist-led care group highlights the critical role of pharmacists in overcoming clinical inertia. Pharmacists are uniquely positioned to systematically identify uncontrolled BP, review current therapy, and recommend timely treatment escalation based on guideline targets. Similar improvements in treatment optimization have been reported in both high-income countries and LMICs following the integration of pharmacists into multidisciplinary care teams.18 –20,31
The high acceptance rate of pharmacist recommendations by physicians observed in this study reflects effective interprofessional collaboration. Collaborative practice models enhance trust, streamline clinical decision-making, and reduce fragmentation of care, all of which are essential for managing chronic conditions such as hypertension. Evidence suggests that such team-based approaches lead to more consistent application of treatment guidelines and improved patient outcomes.19,21
In addition to improving treatment timeliness, pharmacist-led care resulted in greater reductions in systolic and diastolic BP and a higher proportion of patients achieving controlled BP at follow-up. These findings are consistent with prior randomized trials and meta-analyses demonstrating that pharmacist interventions lead to clinically meaningful improvements in BP control.20,32 Even modest reductions in BP are known to substantially lower the risk of stroke, myocardial infarction, and heart failure, particularly in older adults.12,33
Higher baseline systolic BP was associated with faster treatment intensification, suggesting that clinicians may prioritize patients perceived to be at higher immediate cardiovascular risk. While this approach is understandable, it may inadvertently delay appropriate escalation in patients with moderately elevated BP. Pharmacist-led interventions can help standardize care by ensuring that treatment decisions are driven by evidence-based thresholds rather than subjective risk perception alone.34 –36
The pattern of antihypertensive intensification observed in this study, including increased use of combination therapy and first-line drug classes, aligns well with international hypertension management guidelines. Guideline-concordant prescribing is particularly important in older adults, who often have multiple comorbidities and require careful medication selection to balance efficacy and safety.37 –39
Medication adherence counseling was a key component of the pharmacist-led interventions. Poor adherence is a major contributor to apparent treatment resistance and may falsely reinforce therapeutic inertia. By addressing adherence barriers, pharmacists help differentiate true uncontrolled hypertension from pseudo-resistance, enabling appropriate and timely treatment escalation.40,41
The findings of this study are especially relevant to the Ethiopian healthcare system, where the burden of non-communicable diseases is rising rapidly amid limited human and financial resources. National health strategies increasingly recognize the expanded clinical role of pharmacists, and this study provides strong real-world evidence supporting their integration into chronic disease management services.22,42
From a health systems perspective, pharmacist-led care represents a scalable and potentially cost-effective strategy to improve hypertension outcomes. Task-sharing models that leverage pharmacists’ expertise may help address physician shortages, improve continuity of care, and enhance quality of service delivery in both tertiary and primary care settings.43,44 In addition to factors related to the healthcare system, new evidence shows that psychosocial and patient-related factors are also important for managing high BP. Recent research indicates that psychological factors, including alexithymia, may affect BP regulation, treatment adherence, and overall clinical outcomes in patients with hypertension.45,46 In addition, studies involving specific populations, such as pregnant women, suggest that disparities in emotional processing may influence variations in hypertension patterns and disease progression. 47 These findings highlight the necessity for a more holistic, patient-centered methodology in hypertension management, augmenting pharmacist-led initiatives to enhance treatment outcomes.
Limitations and strengths
This study has notable strengths, including a multicenter prospective design across tertiary hospitals in Northwest Ethiopia, which enhances generalizability, and prospective follow-up with standardized data collection and objective BP measurements, ensuring reliable results. High physician acceptance of pharmacist recommendations also demonstrates strong interprofessional collaboration and real-world feasibility.
Although baseline characteristics between groups were comparable, the observational design and non-random group assignment mean that residual confounding and selection bias cannot be completely ruled out, even after multivariable adjustment. In addition, the study was limited to older adults attending tertiary hospitals in Northwest Ethiopia, which may restrict the generalizability of the findings to primary care settings. Furthermore, the study did not assess cost-effectiveness or patient-reported outcomes. Nonetheless, the multicenter design and prospective follow-up enhance the robustness and real-world relevance of the findings.16,34
Conclusion
Pharmacist-led interventions significantly reduced therapeutic inertia by accelerating antihypertensive treatment intensification and improving BP control among older adults. These findings support integrating pharmacists into multidisciplinary hypertension care teams as a practical and scalable strategy to enhance the quality of hypertension management in resource-limited settings.
Supplemental Material
sj-docx-1-taj-10.1177_27558428261452289 – Supplemental material for Improving timeliness of antihypertensive treatment intensification through pharmacist-led interventions among older adult patients in Northwest Ethiopia: Multicenter prospective cohort study
Supplemental material, sj-docx-1-taj-10.1177_27558428261452289 for Improving timeliness of antihypertensive treatment intensification through pharmacist-led interventions among older adult patients in Northwest Ethiopia: Multicenter prospective cohort study by Samuel Berihun Dagnew, Tigabu Eskeziya Zerihun, Desalegn Addis Mussie, Tilaye Arega Moges, Samuel Agegnew Wondm, Fasil Bayafers Tamene, Getachew Yitayew Tarekegn, Woretaw Sisay Zewdu and Abel Temeche Kassaw in Sage Open Chronic Disease
Footnotes
Acknowledgements
For their cooperation during the study, the hospital administration and study participants are greatly appreciated by the authors.
ORCID iDs
Ethical considerations
Ethical clearance was obtained from the Debre Tabor University Ethical Review Committee (IRERC) with approval number DTU/Re/214/2024, and a letter of authorization was given by the medical director of the three hospitals. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from all participants before enrollment. Participants were adequately informed about the purpose of the study, procedures involved, potential risks and benefits, and their right to refuse or withdraw from the study at any time without any effect on their routine medical care. Confidentiality of participant information was strictly maintained by using anonymous data collection tools and restricting access to the data to the research team only.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Data availability statement
The dataset used to support the findings of this investigation is described in the article and the Supplemental Files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.