
Abstract
Migraine is a prevalent and disabling neurological disorder, and a subset of patients remains refractory to standard treatments, requiring integrative therapeutic strategies. We present the case of a 57-year-old woman with chronic, treatment-resistant migraine: Acute therapies such as paracetamol, nonsteroidal anti-inflammatory drugs, and triptans provided only partial relief but were overused and caused adverse effects, while preventive treatments (including β-blockers, calcium channel blockers, anticonvulsants, antidepressants, calcitonin gene-related peptide inhibitors, and botulinum toxin) failed to provide meaningful benefit. The patient was treated with a balanced cannabis oil formulation containing tetrahydrocannabinol and cannabidiol (5 mg/mL each), titrated gradually up to 30 drops daily. After one month, she experienced a marked clinical improvement, with headache days reduced by half, lower pain intensity, better sleep quality, and enhanced quality of life. At three months, symptoms partially worsened, but further dose adjustment restored benefits, leading to sustained improvements at six months. No functional limitations or psychiatric symptoms were reported during treatment. This case illustrates the potential of cannabis oil as a promising therapeutic option for drug-resistant migraine while also emphasizing key challenges such as dose titration, treatment costs, and limited access to specialized pharmacists. Controlled clinical studies are needed to better define efficacy, safety, and optimal use of cannabis-based therapies in migraine management.
Introduction
Migraine, a primary headache disorder, is a relatively common and often debilitating neurological disorder, affecting approximately 14%–15% of the global population. 1 It is characterized by recurrent episodes of moderate to severe headache, typically unilateral and pulsating in nature, and is frequently accompanied by associated symptoms such as nausea, vomiting, photophobia, and phonophobia; in some cases, aura phenomena (transient neurological symptoms such as visual disturbances) precede the headache phase. 2 Migraine significantly impacts daily functioning, productivity, and overall quality of life and is recognized as an important cause of disability worldwide, particularly among women. 3
Acute treatments, such as paracetamol, nonsteroidal anti-inflammatory drugs (NSAIDs), or triptans, are intended to relieve symptoms during an active migraine attack and are typically used on an as-needed basis. 4 In contrast, preventive treatments is used regularly, often daily, with the goal of reducing the frequency, severity, and duration of migraine attacks over time. Preventive therapy, including β-blockers, calcium antagonists, antiepileptics, certain antidepressants, and, more recently, calcitonin gene-related peptide inhibitors, is generally considered for patients who experience frequent migraines (typically more than three headache days per month), prolonged or disabling attacks, or cases where acute medications are ineffective, overused, or poorly tolerated. 5 Even though there are different options, a subset of individuals remains refractory to standard treatment, experiencing frequent and severe attacks despite adherence to recommended medical regimens. 6 For these patients with drug-resistant migraine, the burden of disease can be profound, prompting the need for novel therapeutic strategies. 7
In recent years, increasing attention has turned toward cannabis-based products as potential therapeutic agents for various chronic pain and neurological conditions. 8 Compounds such as cannabidiol (CBD) and tetrahydrocannabinol (THC), the principal constituents of cannabis (Figs. 1–2), are known to exert complex effects on the endocannabinoid system, which plays a role in pain modulation, inflammation, and neuronal excitability.9,10 Preliminary evidence suggests that cannabinoids may offer symptomatic relief for some migraine sufferers, though clinical data remain limited and heterogeneous. 11

Botanical representation of Cannabis sativa (illustration created by Elena Mazzoleni—October 2025).

Botanical representation of Cannabis indica (illustration created by Elena Mazzoleni—October 2025).
This case report presents the use of therapeutic cannabis oil in a patient with chronic, treatment-resistant migraine who experienced significant clinical improvement.
Methods
Patient Information
The patient is a 57-year-old woman who has suffered from headaches since adolescence; however, the true migrainous pattern appears to have emerged more clearly, with more significant symptoms, starting at menopause. She is a lifelong nonsmoker, does not consume alcohol, and had one pregnancy, which was uneventful and full-term. Her height is 153 cm and weight 61 kg, corresponding to a body mass index of 26.0 kg/m2, which is slightly above the normal range. She leads a moderately active lifestyle, working as a shop assistant and engaging in 30-minute total-body training sessions twice a week.
The patient underwent a left mastectomy for breast cancer more than 10 years ago; she did not receive chemotherapy or radiotherapy and has fully recovered from the disease. She has a history of recurrent calcium oxalate kidney stones and previously experienced mild depression, which was successfully treated with paroxetine and psychological support. The patient had no history of illegal drug abuse or psychosis and has no known allergies except to ciprofloxacin and iodinated contrast agents.
The patient provided full informed consent to undergo the integrative treatment as part of her routine care and agreed to the anonymous dissemination of the clinical outcomes for scientific purposes.
Diagnostic Assessment
The CAse REports (CARE) guidelines were followed in the reporting of this clinical case. 12
The patient consulted a licensed physician with experience in integrative medicine (M.A.) in mid-April 2025 to evaluate her health status and seek assistance with therapeutic cannabis for her clinical condition. The diagnosis of migraine was made several years ago at the “IRCCS Istituto delle Scienze Neurologiche di Bologna” (Italy), a specialized neurology referral center, following the exclusion of secondary causes of headache, such as tumors or vascular malformations, through comprehensive brain and neck imaging. At the initial visit, the patient reported suffering from symptoms of chronic migraine (headache episodes were lateralized and sometimes preceded or accompanied by visual aura and nausea), with an average of 18–20 headache days per month. Most attacks occurred predominantly at night, significantly impairing her sleep quality. She had attempted various nonpharmacological approaches, including physical therapies such as massage, osteopathy, neck physiotherapy, and acupuncture, as well as dietary modifications like a low-carbohydrate ketogenic diet. However, these interventions provided only transient relief and limited long-term benefit. Over time, she developed acute medication overuse, particularly with triptans, necessitating their discontinuation. Given her history of recurrent kidney stones, NSAIDs had to be minimized, and paracetamol proved poorly effective, even when combined with caffeine. The patient reported experiencing mental fog and digestive side effects (such as nausea and constipation) while using opioid medications, which significantly limited their tolerability.
The following preventive pharmacological treatments were subsequently tried but failed to provide adequate symptom control:
Flunarizine: Not effective. Propranolol: Not effective and not tolerated (caused dizziness, fatigue, hypotension, and bradycardia). Atenolol: Not effective and not tolerated (caused the same side effects as propranolol). Amitriptyline: Not effective. Topiramate: Limited efficacy; discontinued due to recurrent kidney stones. Sertraline: Not effective. Alprazolam: Not tolerated (caused excessive sedation even at low doses). Clonazepam: Not effective. Galcanezumab: Poorly effective (transient partial improvement after the initial dose, followed by a quick return to baseline symptom pattern). Botulinum toxin injections (six sessions): Not effective.
During the initial assessment, all relevant clinical information was collected to evaluate the presence of any specific contraindications to the proposed therapeutic program and to determine the patient’s eligibility for medical cannabis treatment. At the time of the first clinical evaluation (April 2025), the patient was taking paroxetine 20 mg daily, prescribed to support long-term mood stability, and ospemifene 60 mg/day, which had been recently recommended by her gynecologist for the treatment of postmenopausal genitourinary symptoms. The patient was administered the Numeric Pain Rating Scale (NPRS), the Single-Item Sleep Quality Scale (SQS), and the EuroQol-5 Dimension (EQ5D) questionnaires at baseline and subsequently at one, three, and six months during clinical assessments; she was also asked to keep track of the number of headache days per month throughout the observation period (Table 1). Patient contact via phone call was conducted at weeks 1 and 2 after initiating therapy to guide medication titration and monitor for potential side effects.
The NPRS is a simple, widely used tool for assessing pain intensity during migraine attacks: Patients rate their pain on a scale from 0 to 10, where 0 means “no pain” and 10 represents “the worst pain imaginable.” 13 It is quick to administer and sensitive to changes over time, making it useful for tracking pain progression. The SQS is a brief, one-question tool used to assess subjective sleep quality: Patients are asked to rate the overall quality of their sleep over the past 7 days on a scale from 0 (terrible) to 10 (excellent). 14 The EQ5D is a standardized instrument for measuring health-related quality of life that evaluates five key dimensions (rated at five levels of severity): Mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. 15 This questionnaire also includes a visual analogue scale where patients rate their overall health on a 0–100 scale, with 100 indicating the best possible health status.
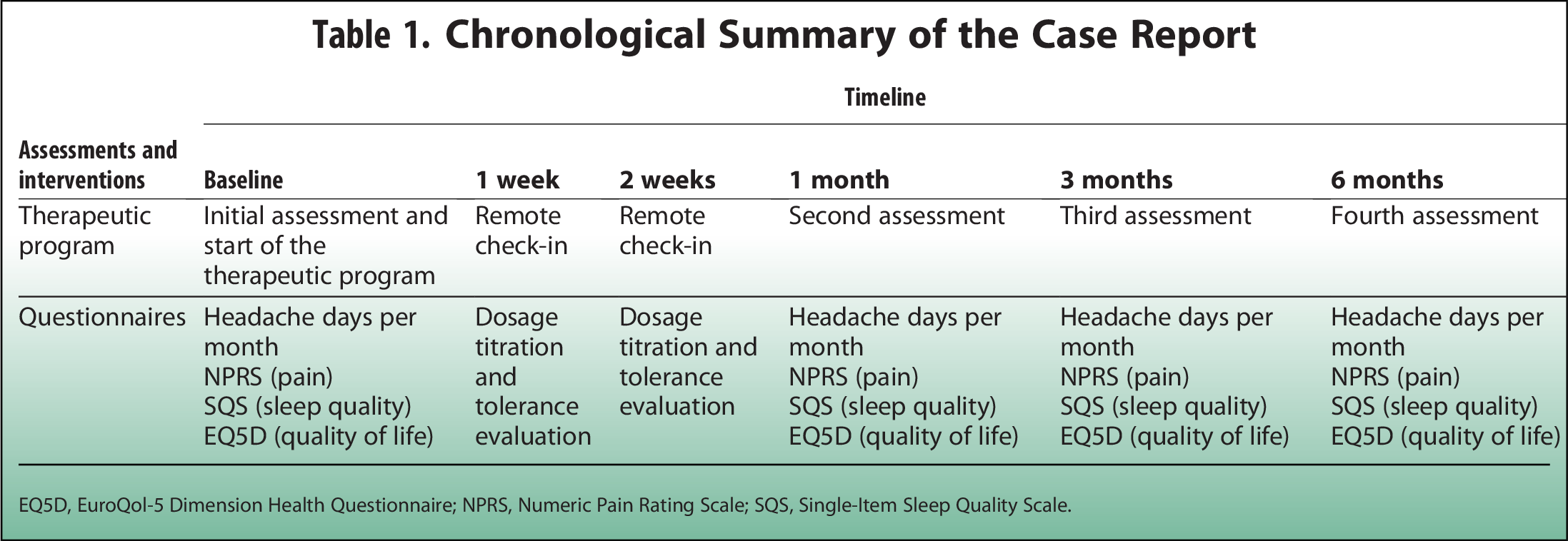
EQ5D, EuroQol-5 Dimension Health Questionnaire; NPRS, Numeric Pain Rating Scale; SQS, Single-Item Sleep Quality Scale.
Therapeutic Intervention
The patient was prescribed a cannabis oil formulation containing 5 mg/mL of THC and 5 mg/mL of CBD, custom-prepared by a compounding pharmacy. The product was obtained by diluting Tilray® 10:10 (10% THC and 10% CBD) in a 1:2 ratio with an MCT vegetable oil. This extract is derived from a standardized blend of Cannabis sativa, C. indica, and hybrid strains, ensuring a consistent cannabinoid profile. The treatment was initiated at a dose of 5 drops in the evening after dinner, before going to sleep, with a gradual titration schedule: The dosage was increased by 5 drops per week, up to a maximum of 40 drops per day, based on tolerability and clinical response. The patient received written instructions outlining the dosage schedule and was advised to contact the physician by telephone or email in case of any adverse effects or concerns during treatment.
Results
The patient’s clinical assessment results over the course of treatment are summarized in Table 2. At baseline, the patient reported 20 headache days per month, with an NPRS pain score of 6/10, SQS sleep quality score of 6/10, and EQ5D quality-of-life score of 70/100. In the initial phase of treatment, the patient progressively reached a dosage of 30 drops of cannabis oil. After one month, there was a marked improvement, with headache frequency halving to 10 days per month, pain reduced to 2/10, sleep quality rated at 10/10, and quality of life increasing to 95/100. At the three-month assessment, the clinical condition worsened, with headache days rising to 14 per month, pain increasing to 4/10, and sleep quality declining to 7/10, with EQ5D decreasing to 75/100. In response, the patient was advised to increase the dosage to 40 drops daily. At six months, clinical outcomes showed renewed improvement, compared to the three-month evaluation. Headache frequency decreased to 8 days per month, pain was reduced again to 2/10, sleep quality improved to 9/10, and quality of life increased to 90/100. Throughout the entire follow-up period, the patient reported no limitations in mobility, self-care, or daily activities. Perceived pain and discomfort showed a fluctuating course: It was severe at baseline, improved substantially to mild at one month, then worsened slightly to moderate at three months before improving again to mild by the six-month mark. In contrast, levels of anxiety and depression remained stable, with the patient consistently reporting no symptoms at any point during the observation period.
Results of Clinical Assessments

Discussion
Critical Overview of the Available Evidence
Nociplastic pain, a mechanism involving altered nociceptive processing without clear evidence of tissue damage or inflammation, is increasingly recognized in certain forms of primary headache, such as chronic migraine. 16 This form of pain is hypothesized to be potentially linked to a deficiency or dysregulation of the endocannabinoid system, 17 which plays a key role in modulating pain, mood, and inflammation. In this context, administering exogenous, plant-derived cannabinoids may help restore endocannabinoid balance and reduce the frequency or severity of symptoms, particularly in patients who do not respond adequately to conventional therapies. 18 Furthermore, therapeutic cannabis extracts may provide clinical benefits through the “entourage effect,” a synergistic interaction among the plant’s active compounds 19 : These include cannabinoids, terpenes, and flavonoids, which act on diverse pharmacological targets, including cannabinoid receptors, serotonin pathways, and ion channels. In general, phytocannabinoids (such as THC and CBD) interact with the endocannabinoid system to modulate nociceptive signaling and reduce neuronal hyperexcitability, 20 which are key features in migraine pathophysiology. Additionally, CBD has been shown to exert anti-inflammatory and anxiolytic effects,21,22 which may further mitigate migraine severity and improve overall well-being. In addition to cannabinoids, terpenes and flavonoids contribute to the therapeutic potential of cannabis extracts through their analgesic, anti-inflammatory, antioxidant, anxiolytic, and neuroprotective properties, thereby reinforcing the multimodal efficacy of the treatment in migraine. This wide-ranging mechanism of action may amplify the benefits of cannabis extracts, positioning them as a useful therapeutic option for treatment-resistant headache disorders.
In the present case, the initial response to cannabis therapy was followed by a recurrence of symptoms, which is consistent with the patient’s clinical history of migraine worsening during summertime, when increased light exposure and higher ambient temperatures typically exacerbated attacks. This seasonal pattern required an adjustment in the cannabis oil dosage to maintain effective symptom control: The titration strategy successfully restored clinical benefit, with renewed improvements in pain, headache frequency, sleep quality, and quality of life observed at six months. Careful dose adjustments were implemented to address the potential development of cannabinoid tolerance, 23 which may contribute to a partial loss of efficacy over time, while aiming to maintain the minimal effective dose and closely monitoring the patient to prevent both overdose and diminished therapeutic effect. One of the major challenges in clinical cannabis therapy lies in the identification of the optimal extract composition and dose titration. 24 This process requires time, careful follow-up, and clinical experience, as interindividual variability can significantly influence therapeutic outcomes. Consequently, effective use of cannabis-based treatments not only demands patient adherence but also adequate training of health care professionals to guide dose adjustments and monitor efficacy and safety over time. Other important limitations may include the costs of treatment and the difficulty in finding pharmacists with specific expertise in cannabis formulations, which can complicate access to the drug after a medical prescription. Nevertheless, this case report underscores that cannabis may represent a promising therapeutic option in drug-resistant migraine, offering meaningful benefits where conventional therapies have failed.
With regard to safety and tolerability, cannabis oil was administered solely in the evening, and the patient reported only mild sedation, which was perceived as beneficial rather than adverse, as migraine attacks predominantly occurred at night and the treatment appeared to support improved sleep quality. Importantly, no daytime sedation, cognitive impairment, or alterations in sensorium were reported. This favorable tolerability profile may be partly attributable to the balanced cannabinoid ratio, 25 as well as to the cautious and gradual dose titration adopted, 24 both of which may have mitigated typical THC-related side effects.
Patient Perspective
The patient initially expressed some skepticism about using cannabis oil as a therapeutic option, having no prior experience with cannabis-based treatments. However, after enduring years of persistent migraine symptoms with nonsignificant relief from standard therapies, she was open to exploring this approach. Throughout the follow-up period, the treating physician (M.A.) provided continuous support, answering questions, addressing concerns, and guiding the patient through the titration process to determine an effective and well-tolerated dosage; this collaborative care played a key role in the patient’s willingness to adhere to the treatment.
Study Limitations
This case report describes the clinical experience of a single patient, and, as such, its findings are inherently limited in terms of generalizability. The subjective nature of symptom reporting, including pain intensity, frequency, and associated features, introduces potential recall bias. To partially address this limitation, the patient was asked to maintain a structured headache diary throughout the observation period to track symptom patterns and treatment response more accurately.
Conclusions
This case report illustrates the potential role of therapeutic cannabis oil as a valuable option for patients with chronic, treatment-resistant migraine. In this patient, cannabis treatment was associated with a clinically meaningful reduction in headache frequency and pain intensity, as well as improvements in sleep quality and overall quality of life. Importantly, the observed benefits were sustained over several months of follow-up after careful titration of dosage. Future controlled studies are warranted to confirm efficacy, refine dosing strategies, and better define the role of cannabis in the broader therapeutic landscape of migraine management.
Footnotes
Author Disclosure Statement
M.A. is a member of the Clinn network, a professional network of physicians prescribing therapeutic cannabis. The Clinn network management had no role in the collection, analysis, or publication of the data presented in this case report. The other authors declare no conflicts of interest.
Funding Information
This research received no external funding.▪