
Abstract
Background:
Dyspnea and pain are subjective sensations influenced by emotional and cognitive factors, often limiting the effectiveness of pharmacological treatments. Yoga has been explored as a non-pharmacological approach, but most studies rely on subjective reports rather than quantitative measures. This study assessed dyspnea and pain in healthy adults using respiratory resistance and thermal stimulation before and after a single yoga session to clarify its immediate sensory effects under controlled conditions.
Methods:
In this randomized crossover trial, 27 adults underwent both a 60-min yoga session and a control rest condition. The sensations of dyspnea, pain threshold, and heart rate variability (coefficient of variation of R-R intervals [CVRR]) were assessed before and after yoga and rest sessions. Dyspnea response was quantified using slope values derived from log-transformed Borg scores. Statistical analyses included t-tests, correlation coefficients, and regression models. Significance was set at p < 0.05.
Results:
Twenty-seven subjects completed both trials. Compared with the control condition, the yoga condition significantly reduced dyspnea ratings at higher resistance levels and decreased the slope of Borg scores (p < 0.001). Pain threshold did not differ between conditions overall but showed a significant positive correlation with yoga experience (ρ = 0.51, p = 0.01). CVRR increased significantly only in experienced yoga practitioners.
Conclusion:
A single yoga session may produce immediate reductions in dyspnea regardless of prior experience. Pain relief and autonomic enhancement were observed only in experienced yoga practitioners, indicating distinct mechanisms and practice-dependent effects across symptoms.
Introduction
Dyspnea and pain are subjective sensory experiences with both physical and psychological dimensions. These symptoms impair quality of life, especially in individuals with chronic conditions such as chronic obstructive pulmonary disease (COPD), heart failure, and chronic pain syndrome.1,2 Chronic pain affects approximately 20% of the global population, contributing to increased health care costs and emotional distress. 3 While pharmacological treatments such as opioids and non-steroidal anti-inflammatory drugs are commonly used, concerns regarding side effects and dependency have led to increased interest in non-pharmacological alternatives. 4 Moreover, both dyspnea and pain are modulated by emotional and cognitive factors, often limiting the efficacy of purely somatic treatments.
Yoga, a mind–body practice integrating physical postures (Asana), breathing exercises (Pranayama), and meditation (Dhyana),5,6 has been investigated for its potential effects on dyspnea and pain. Prior studies suggest benefits across various populations, including improved exercise tolerance in COPD, reduced pain or fatigue in oncology settings, and decreased headache frequency and intensity.7–10
However, many investigations rely on subjective recall or focus on specific patient groups,7,11–16 limiting generalizability and causal inference. Quantitative evaluations of yoga’s immediate effects on pain and dyspnea remain scarce, and few studies have assessed these sensations concurrently within an integrated framework. To address these gaps, this randomized crossover trial was conducted in healthy adults to objectively evaluate yoga’s effects on dyspnea sensation and pain thresholds. Studying a healthy population helped control confounding factors such as disease and medication, enabling clearer assessment of physiological responses. This design may help clarify the potential role of yoga as a non-pharmacological intervention in rehabilitation medicine.
Materials and Methods
Study design
This single-center randomized crossover trial was conducted between June 2023 and September 2024. The study was approved by an institutional committee (approval number: 2023-1-632) and registered with the University Hospital Medical Information Network (UMIN-CTR#000051208). Written informed consent was obtained from all subjects. All procedures were conducted in accordance with the Declaration of Helsinki as revised in 2013. We used the CONSORT reporting guideline 17 to draft this article and the CONSORT reporting checklist 18 when editing, included in Supplementary Data S1.
Inclusion and exclusion criteria
Healthy adults aged 18–65 years were recruited via social media and flyers distributed at yoga studios and community centers in Miyagi Prefecture. Exclusion criteria included respiratory, cardiovascular, renal, hepatic, neurological, musculoskeletal, or psychiatric disorders; malignant tumors; chronic pain; pregnancy or postpartum period; and cognitive impairment or mental health conditions that could affect study participation. Individuals who smoked were also excluded. Any condition deemed unsuitable by a physician was an additional exclusion criterion.
Based on prior studies assessing sensation of dyspnea and pain thresholds, 19 a sample size of 19 was calculated (effect size = 0.7, α = 0.05, power = 0.80). To account for potential dropouts, the target enrollment was set at 24 subjects. Because several individuals had already completed preliminary screening when the target was reached, enrollment continued until 34 eligible subjects were included (Fig. 1).
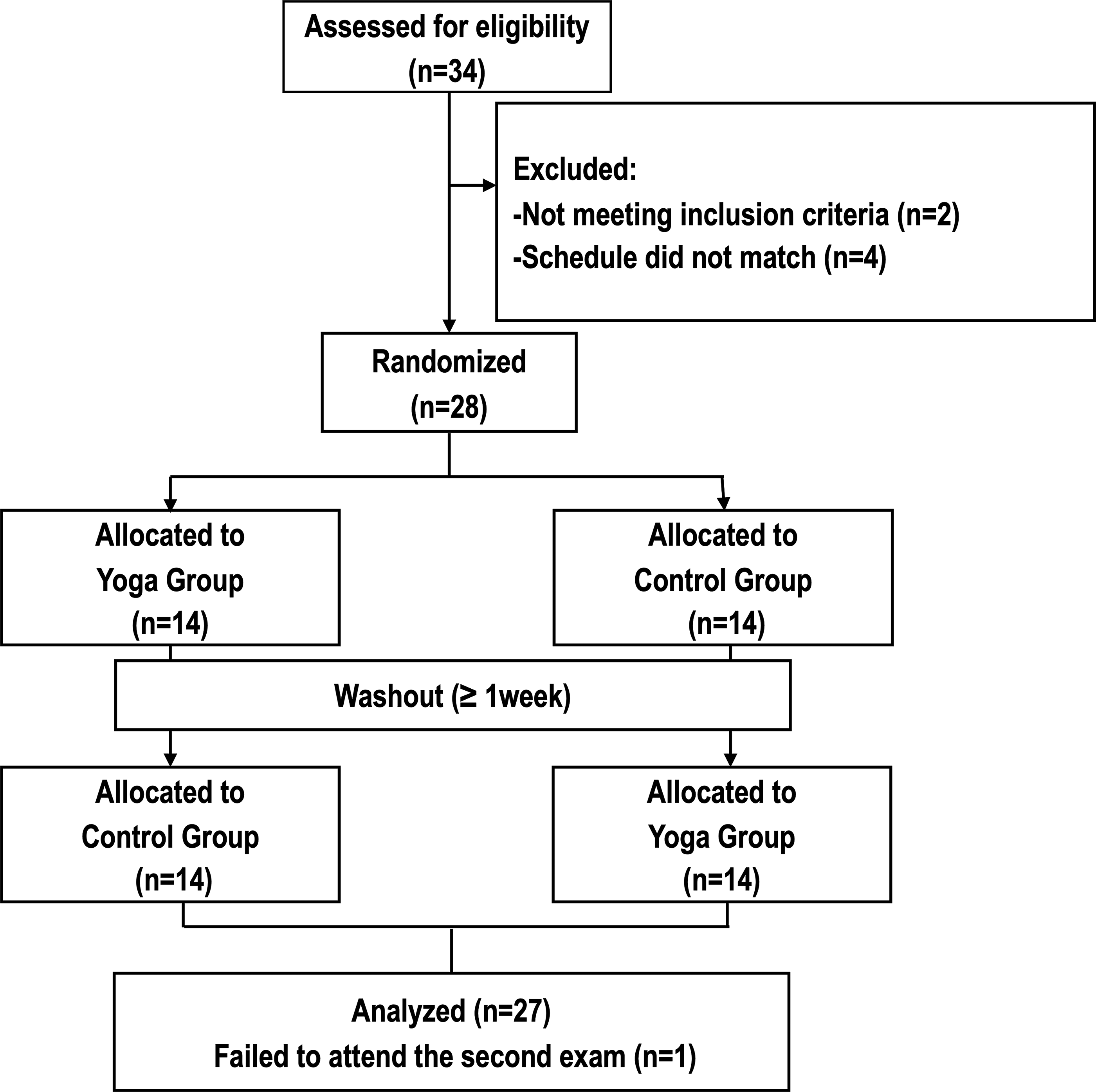
CONSORT flow diagram of participant enrollment and analysis. Of the 34 healthy Asian adults who expressed interest in participating, 6 were excluded for not meeting inclusion criteria. One additional individual did not complete the second session and was excluded. The remaining 27 participants met all inclusion criteria and completed both yoga and rest sessions and assessments and were therefore included in the final analysis.
Protocol and interventions
Subjects were randomly assigned to either the yoga session or the control condition for the first trial. Randomization was performed by generating a random number for each subject using the RAND function in Excel (Microsoft Corp., Redmond, WA, USA), sorting the list, and allocating subjects in a 1:1 ratio to the yoga-first or control-first condition (Fig. 1). A 1-week washout period was implemented with reference to a prior crossover study examining sensory and pain-related outcomes. 20
Trials were conducted in a controlled laboratory environment where humidity was maintained below 60%, temperature between 20°C and 25°C, and adequate lighting and ventilation were ensured.
To minimize variability across the two trials, subjects were instructed to refrain from alcohol and caffeine before each visit and to avoid major changes in their usual lifestyle, including diet (e.g., markedly increasing or decreasing caloric intake or adopting a restrictive diet), physical activity (e.g., starting a new exercise routine or substantially changing daily activity levels), medication use, and sleep duration. For female subjects, testing was scheduled to avoid menstruation whenever possible. To reduce diurnal variation, the first and second trials were scheduled at similar times of day for each subject.
At the first visit, medical history, smoking history, medication use, baseline lung function (VC, FEV1, FVC, FEV1/FVC%) assessed by spirometry using the HI-701 device (CHEST M.I., Tokyo, Japan), height, weight, body fat percentage measured using the Omron HBF-702T (Omron Corporation, Kyoto, Japan), and yoga experience were recorded.
Each trial consisted of pre-assessments of dyspnea, pain threshold, and heart rate variability (HRV) followed by a 10-min rest period and then the assigned condition (yoga or rest). Post-assessments of the same parameters were conducted immediately after the assigned condition. The content of each condition was as follows:
Yoga session
Each participant completed a 60-min one-on-one yoga session. The Hatha yoga-based program included a 10-min warm-up (stretching), followed by 40 min of physical postures, 5 min of breathing exercises, and 5 min of meditation. All components were delivered according to a standardized manual (Supplementary Data S2) that included elements for which no serious adverse events have been reported.21,22 Instruction was provided by a certified Yoga Alliance instructor, who offered verbal guidance and hands-on adjustments as needed. Modifications such as knee flexion during forward bends and the use of yoga blocks were suggested to accommodate individual physical limitations and ensure comfort and safety.
Control condition
Subjects rested for 60 min in the laboratory setting. During this period, they were allowed to engage in quiet, non-strenuous activities (e.g., reading or using personal electronic devices) but were instructed to refrain from meditative exercises such as yoga or tai chi.
Outcome measures and equipment
The primary outcomes were the sensation of dyspnea and pain threshold. Secondary outcomes included HRV and safety during study participation. For these outcomes, assessments were conducted in a fixed order (HRV, dyspnea, pain threshold). HRV was recorded for 7 min according to the predefined posture sequence, followed by the dyspnea assessment (approximately 8–10 min) and the pain threshold assessment (approximately 1 to 2 min). Transitions between assessments involved only brief repositioning without additional rest periods.
All assessments of dyspnea, pain threshold, and HRV were performed by trained examiners (licensed physical therapists and a licensed nurse) following standardized procedures to ensure measurement reliability.
Details of the measurement procedures are as follows.
Dyspnea
Following a previously established protocol, 19 dyspnea was assessed using a dedicated device capable of applying external inspiratory resistance as a viscous load. The device allowed linear resistance settings of 0, 10, 20, and 30 cmH2O/L/s. Subjects breathed orally through a respiratory filter (Spiro Filter 999M; CHEST M.I., Tokyo, Japan), simulating clinical triggers of dyspnea by reproducing the sensation of increased breathing resistance. The initial resistance was set to 0 cmH2O/L/s. Subjects wore a nose clip and continued breathing for up to 1 min, and immediately afterward they rated their perceived dyspnea using the modified Borg scale,23,24 ranging from 0 (none) to 10 (maximum). The resistance was then gradually increased up to 30 cmH2O/L/s, with the same measurement procedure repeated at each level. A 1-min rest was provided between levels.
Pain threshold
Based on previously reported methods, 19 pain threshold was measured using a thermal stimulator (UDH-105; Unique Medical Co., Tokyo, Japan). The probe was placed on the volar surface of the participant’s left forearm, and the temperature was increased from 35°C at a rate of 0.25°C/sec. Subjects pressed a remote switch upon first perceiving pain from the heat stimulus. At that moment, heating stopped automatically, and the corresponding temperature was recorded as the pain threshold. To ensure safety, heating was automatically limited to a maximum of 51°C.
Heart rate variability
HRV was measured using a portable ECG device (Kiritsu Meijin; Crosswell Co., Kanagawa, Japan), with the coefficient of variation of R-Rintervals (CVRR) used as the evaluation index. ECG electrodes were attached to the left wrist and left ankle. To ensure standardized resting conditions recommended for HRV measurement, participants were instructed to sit comfortably, avoid unnecessary movement, and maintain a relaxed gaze without closing their eyes. R-R intervals were continuously recorded across four postures: seated (2 min), during and immediately after standing (2 min), standing (2 min), and seated again after standing (1 min).
Safety
Safety was evaluated based on the number of adverse events that occurred during or after the study trials. In addition, a brief post-session contact via email was made with participants, and any symptoms mentioned in their replies were documented as adverse events.
SpO2 was continuously monitored using a fingertip pulse oximeter, with additional checks during the intervention and measurement periods if desaturation was suspected; the trial was discontinued if severe dyspnea occurred or if SpO2 fell below 90%.
The study was conducted under the safety oversight of a rehabilitation medicine physician.
Statistical analysis
Data were analyzed using IBM SPSS Statistics v26. Normality was assessed via the Shapiro–Wilk test. Paired t-tests or Wilcoxon signed-rank tests were used for within-subject comparisons between the yoga and rest conditions. Unpaired t-tests or Mann–Whitney U tests were used for between-subject comparisons involving individual characteristics such as yoga experience. All intervention effects were analyzed using paired procedures appropriate for a two-period crossover design. For each outcome, changes from baseline values were calculated and used for statistical comparisons. Percentage change was used instead of absolute change to normalize inter-individual variability in baseline values.
Based on prior reports of a linear relationship between load and dyspnea, log-transformed Borg scores across all resistance levels (0–30 cmH2O/L/s) were plotted on semi-log graphs to calculate a single slope for comparing pre- and post-intervention responses. The dyspnea–load relationship was confirmed to be sufficiently linear across resistance levels, supporting the use of a single slope for each session.
Spearman’s rank correlation coefficients were used to examine associations between yoga experience and dyspnea or pain, as well as between dyspnea and pain. Multiple regression analysis was conducted to assess the impact of yoga experience on pain perception.
Subgroup analyses based on yoga experience were conducted as exploratory analyses. Because prior studies have not established a consistent definition of experienced practitioners, the practice durations reported in studies cited by three systematic reviews were examined.25–27 Reported durations varied widely (1 month to 12 years), with a mean of 4.22 years; therefore, subjects with ≥5 years of regular practice (at least once per week) were classified as practitioners, and those with <5 years as beginners.
Descriptive statistics are presented as mean ± standard deviation. Statistical significance was set at p < 0.05.
Language editing
Portions of the article were refined using Microsoft Copilot (accessed October 2025) to improve clarity and consistency. All AI-generated suggestions were reviewed and edited by the authors.
Results
Twenty-seven healthy adults who met the inclusion criteria (mean age 40.7 ± 12.8 years; 74% female) completed both trials and all measurements and were included in the final analysis (Fig. 1). All subjects demonstrated normal pulmonary function within the expected range (Table 1), and smoking exposure was minimal: 70% were never-smokers, and former smokers had very low exposure (mean pack-years: 0.3 ± 1.2).
Subject Characteristics
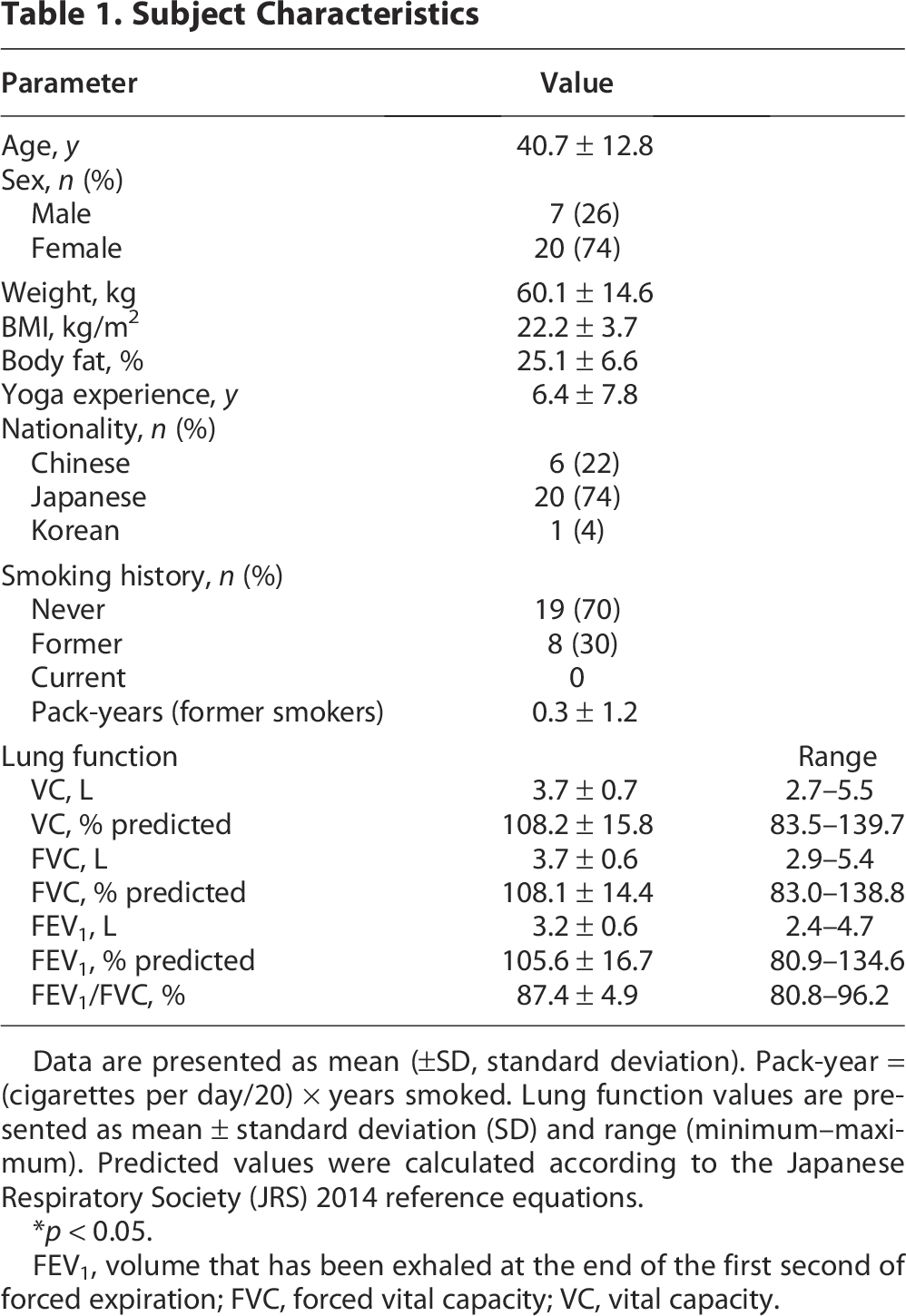
Data are presented as mean (±SD, standard deviation). Pack-year = (cigarettes per day/20) × years smoked. Lung function values are presented as mean ± standard deviation (SD) and range (minimum–maximum). Predicted values were calculated according to the Japanese Respiratory Society (JRS) 2014 reference equations.
*p < 0.05.
FEV1, volume that has been exhaled at the end of the first second of forced expiration; FVC, forced vital capacity; VC, vital capacity.
Pre-intervention values in the second session did not differ between the yoga-first and control-first sequences for either pain threshold (43.4 ± 3.0 vs. 44.2 ± 0.9, p = 0.07) or dyspnea slope (0.1 ± 0.1 vs. 0.1 ± 0.1, p = 0.44), indicating that the 1-week washout period was adequate.
At baseline, no significant differences were observed between the yoga and control conditions in dyspnea ratings, pain thresholds, or HRV (Table 2).
Between-Condition Comparison of Dyspnea, Pain Threshold, and CVRR at Baseline and Following Intervention
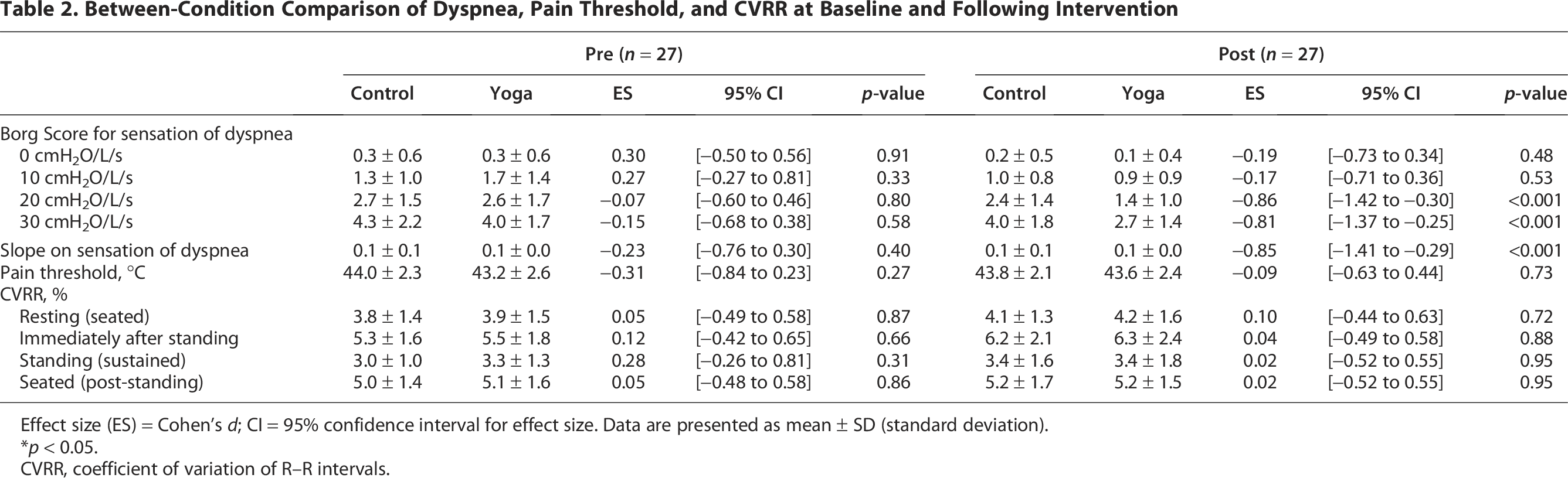
Effect size (ES) = Cohen’s d; CI = 95% confidence interval for effect size. Data are presented as mean ± SD (standard deviation).
*p < 0.05.
CVRR, coefficient of variation of R–R intervals.
Dyspnea
Figure 2 demonstrates percentage changes in perceived dyspnea before and after the yoga and control conditions across all resistance levels (Fig. 2A–D) and slope (Fig. 2E). Compared with the control condition, the yoga condition showed significantly greater percentage reductions in Borg scores at 10, 20, and 30 cmH2O/L/s (−44.0 ± 36.6% vs. −14.5 ± 52.8%, p = 0.02; −47.0 ± 31.9% vs. −2.5 ± 57.2%, p < 0.001; −31.8 ± 30.7% vs. 0.05 ± 33.5%, p < 0.001; Fig. 2B–D). At 0 cmH2O/L/s, the reduction was not statistically significant (−19.8 ± 37.0% vs. −2.77 ± 31.3%, p = 0.07; Fig. 2A). In addition, the yoga condition showed a significantly greater reduction in the slope of dyspnea ratings compared with the control condition (−32.2 ± 32.3 vs. −0.39 ± 37.8, p < 0.001; Fig. 2E).
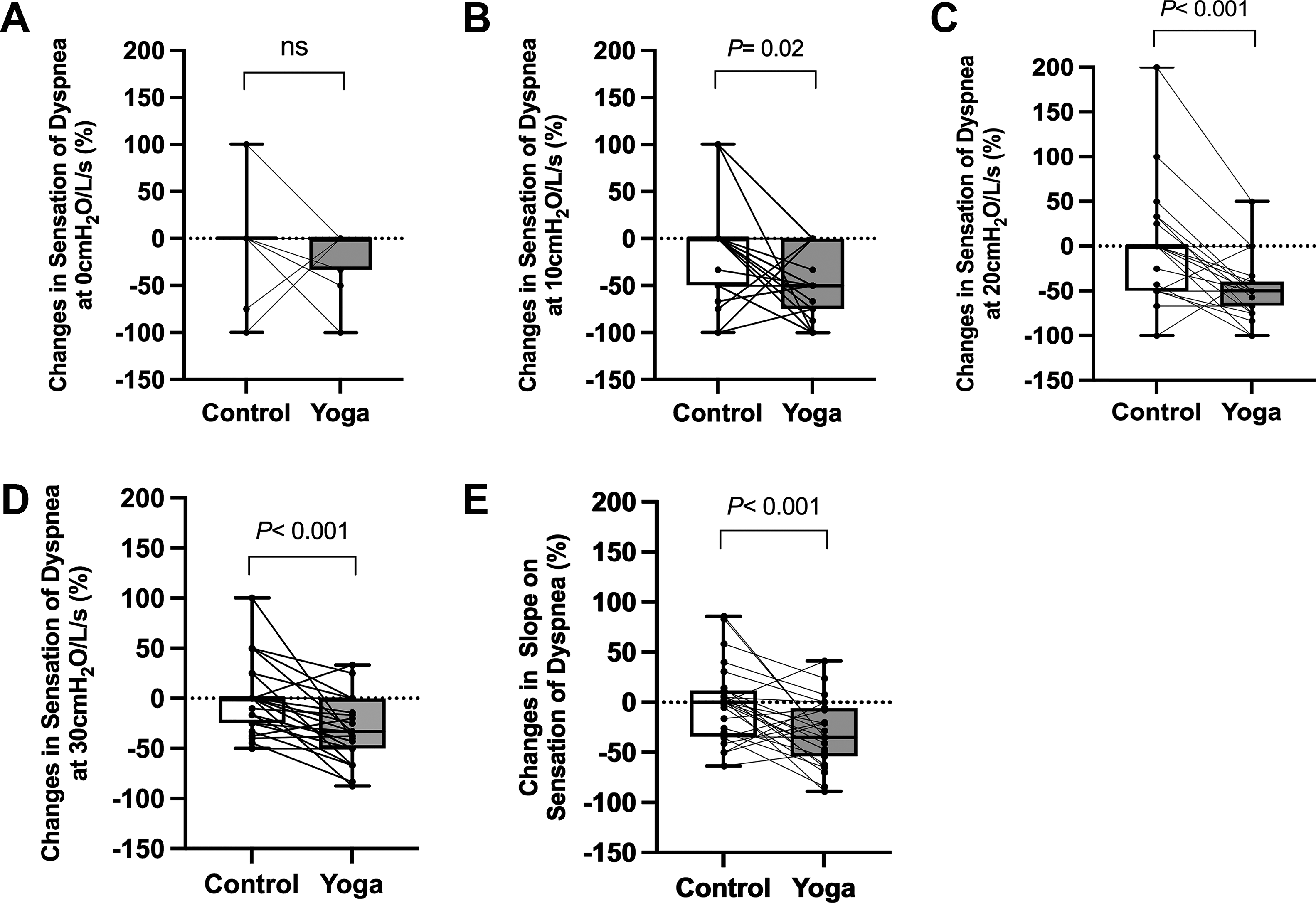
Condition comparison of percentage changes in the sensation of dyspnea across inspiratory loads. Panels A–D show percentage changes in the sensation of dyspnea before and after each condition at inspiratory resistances of 0, 10, 20, and 30 cmH2O/L/s, comparing the yoga and control conditions (n = 27 per condition). Percentage change was calculated relative to each subject’s baseline value. The 0 cmH2O/L/s condition represents breathing without inspiratory resistance. Compared with the control condition, the yoga condition exhibited greater reductions at resistance levels of 10, 20, and 30 cmH2O/L/s. No significant difference was observed at 0 cmH2O/L/s. Panel E shows between-condition comparisons of slopes derived from semi-log linear regression between inspiratory resistance and Borg scores. The yoga condition demonstrated lower slopes than the control condition, indicating a reduced perception of dyspnea across increasing inspiratory loads. Lines connecting dots represent paired values from the same subject across conditions.
Given the variability in yoga experience (years of practice) among subjects, the influence of practice duration on the percentage change in Borg scores was examined. No significant correlation was found between yoga experience and dyspnea reduction at any inspiratory resistance level or for the slope of dyspnea ratings. To further explore this, subjects were categorized into practitioners and beginners as defined in the Methods. In the yoga condition, both practitioners and beginners showed reductions in Borg scores across all resistance levels except 0 cmH2O/L/s and in the slope of dyspnea ratings (Tables 3 and 4), whereas no consistent reductions were observed in the control condition.
Pre- and Post-Intervention Comparison by Experience Level Within Yoga Conditions

Effect size (ES) = Cohen’s d; CI = 95% confidence interval for effect size. Data are presented as mean (±SD, standard deviation).
*p < 0.05.
CVRR, coefficient of variation of R-R intervals.
Pre- and Post-Intervention Comparison by Experience Level Within Control Conditions
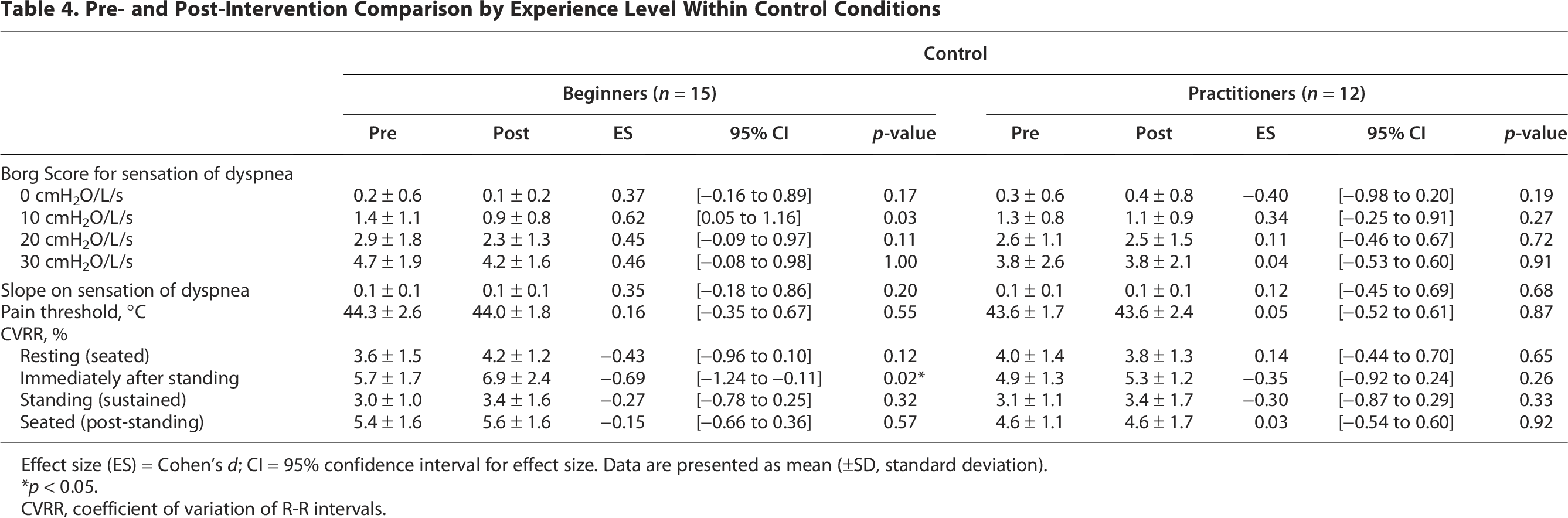
Effect size (ES) = Cohen’s d; CI = 95% confidence interval for effect size. Data are presented as mean (±SD, standard deviation).
*p < 0.05.
CVRR, coefficient of variation of R-R intervals.
No significant correlations were observed between improvements in dyspnea and lung function indices, smoking history, or other subject characteristics.
Pain
No significant difference in pain threshold was observed between the yoga and control conditions (Fig. 3).
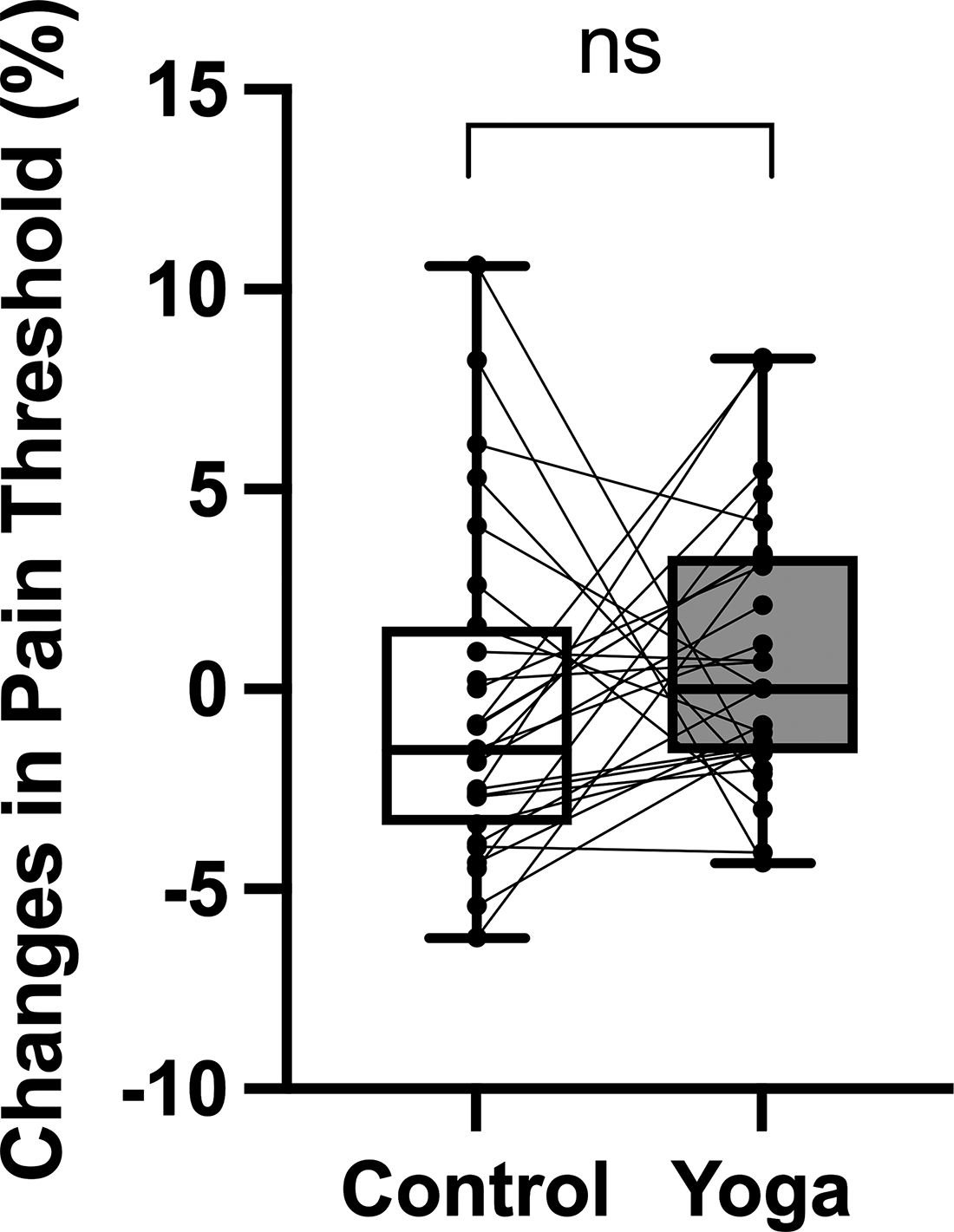
Changes in pain threshold (%) after yoga and rest sessions. Box plots show percentage changes in pain threshold before and after each condition, with the rest condition on the left and the yoga condition on the right (n = 27 per condition). Lines connecting dots represent paired values from the same subject across conditions. No significant difference was observed between conditions. ns = not significant.
To examine the effect of yoga experience, a significant positive correlation was identified between experience duration and pain threshold change rate in the yoga condition (ρ = 0.51, p = 0.01; Fig. 4). Conversely, no correlation was found in the control condition (ρ = –0.06, p = 0.78). A comparison between beginners and practitioners indicated a significant increase in pain threshold only among the practitioners in the yoga condition (p = 0.04; Table 3), while no significant change was observed in the control condition (Table 4).
Correlation between yoga experience and pain threshold change. A Spearman correlation analysis was conducted to examine the association between yoga experience and percentage change in pain threshold. A significant correlation was observed only in the yoga condition (ρ = 0.51, p = 0.01, n = 27).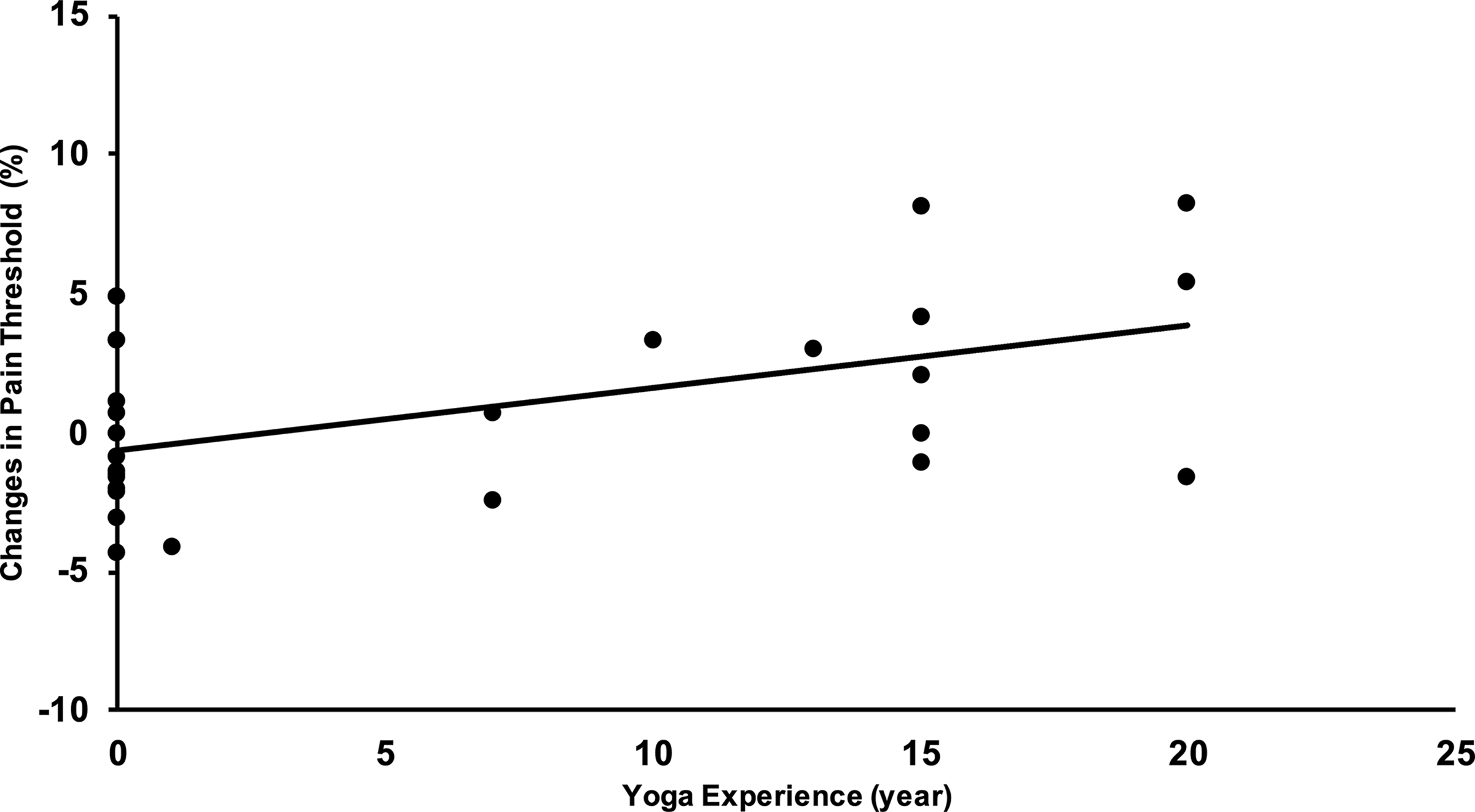
Based on previous reports indicating that age, sex, and body fat percentage influence tolerance to thermal stimuli,28–30 a multiple regression analysis was conducted using the pain threshold change rate as the dependent variable and yoga experience as the independent variable. The following models were tested:
Adjusted for age; Adjusted for age and sex; and Adjusted for age, sex, and body fat percentage.
Yoga experience showed a significant positive effect in all three models within the yoga condition (Table 5). No significant effect was observed in the control condition under any model (Table 5).
Effect of Yoga Experience on Pain Threshold (Multiple Regression Analysis)
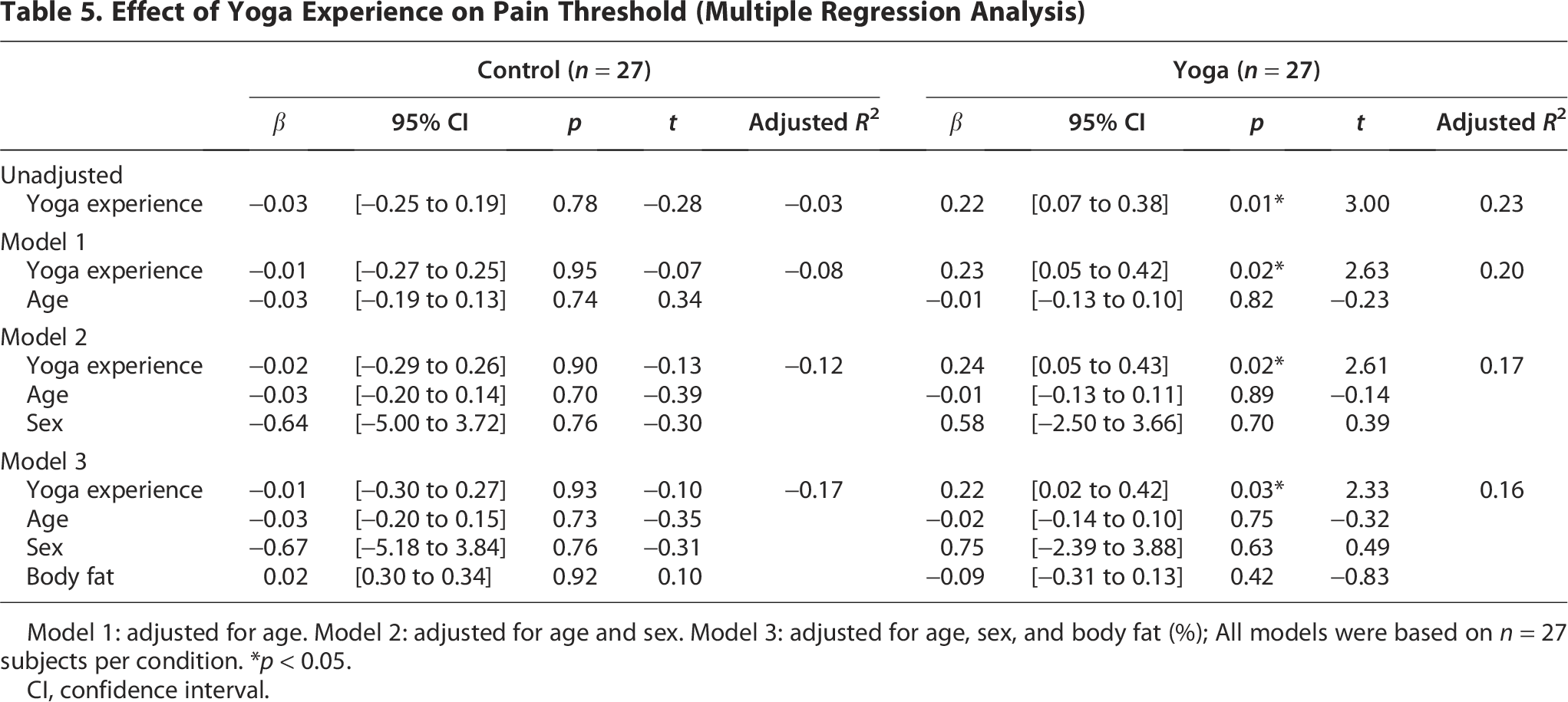
Model 1: adjusted for age. Model 2: adjusted for age and sex. Model 3: adjusted for age, sex, and body fat (%); All models were based on n = 27 subjects per condition. *p < 0.05.
CI, confidence interval.
Dyspnea and pain
Correlation analyses were conducted to examine the relationship between dyspnea and pain threshold across inspiratory resistance levels (0–30 cmH2O/L/s). No significant correlations were found in either condition. Detailed results for the yoga condition were as follows: 0 cmH2O/L/s: ρ = 0.13, p = 0.51; 10 cmH2O/L/s: ρ = –0.32, p = 0.11; 20 cmH2O/L/s: ρ = 0.26, p = 0.20; 30 cmH2O/L/s: ρ = –0.15, p = 0.47.
No significant correlations were observed between the slope of dyspnea ratings and pain threshold in either condition.
Coefficient of variation of R-R intervals
CVRR increased significantly after the yoga intervention in practitioners at several time points (immediately after standing: 4.4 ± 1.2% to 5.7 ± 1.6%, p = 0.02; sustained standing: 2.9 ± 0.9% to 3.6 ± 1.3%, p = 0.04; seated after standing: 4.5 ± 0.9% to 5.1 ± 1.3%, p = 0.02), whereas no significant changes were observed in beginners (Table 3).
No significant correlation was observed between changes in pain threshold and changes in CVRR.
Adverse events
Two subjects reported mild muscle soreness, but no serious adverse events were observed.
Discussion
This study examined the immediate effects of yoga on dyspnea and pain sensations themselves. Quantitative analysis enabled objective evaluation of these sensations, while pre-/post-intervention assessments minimized recall bias.
A single 60-min yoga intervention significantly reduced the sensation of dyspnea under inspiratory resistance in healthy adults. This effect was observed regardless of prior yoga experience, indicating that symptomatic relief may be achievable even after a single session, irrespective of yoga proficiency. In contrast, an immediate increase in thermal pain thresholds was found only among individuals with prior yoga experience, suggesting that pain modulation may require sustained yoga practice.
Since no significant correlation was found between dyspnea and pain perception, the findings suggest that these symptoms may be regulated by distinct mechanisms. No adverse events were reported.
Dyspnea
The yoga program combined physical postures, breathing exercises, and meditation. Several postures resembled thoracic mobility exercises used in pulmonary rehabilitation, potentially facilitating easier breathing. 31 For instance, Parsva Tadasana may activate the rhomboid and serratus anterior muscles to promote chest expansion, while Supta Matsyendrasana may stretch the pectoralis minor and reduce internal rotation of the shoulder, thereby improving thoracic mobility. These physical components might contribute to both mechanical and perceptual improvements.
A previous study reported that physical postures can induce immediate changes in thoracic mobility and trunk muscle activity, 32 and these muscle groups also function as accessory inspiratory muscles. Improved thoracic movement efficiency and postural adjustments may therefore reduce the perceived load during inspiratory resistance.
Moreover, a previous study showed that even beginners demonstrate similar directional patterns of muscle activation during basic yoga postures, 33 which is consistent with the present finding that dyspnea reduction occurred regardless of experience level. Given that the postures used in this study did not require advanced flexibility and were accessible to beginners, it is plausible that the immediate reduction in dyspnea primarily reflects physiological changes elicited by the physical postures themselves.
These findings align with reports showing that breathing-focused rehabilitation can rapidly modulate dyspnea perception and thoracic mechanics, even in clinical populations, supporting the plausibility of immediate perceptual change through respiratory–motor pathways. 34 Given this mechanistic background, dyspnea is often conceptualized as a multidimensional symptom shaped by both physiological and psychological factors. It occurs across respiratory and cardiovascular diseases and in conditions such as panic disorder, and its perception is strongly influenced by emotional and cognitive processes. Psychological interventions such as cognitive behavioral therapy (CBT) and mindfulness-based stress reduction (MBSR) have been shown to alleviate symptoms. 35 CBT targets maladaptive thoughts; MBSR enhances breath and body awareness.35,36 However, both approaches require cognitive engagement and sustained self-observation, which may limit their applicability. 37
Conversely, yoga offers a more accessible alternative, featuring a wide range of postures that can be adapted to suit varying physical abilities and age groups, requiring less cognitive effort—making it suitable for older adults or those with limited cognitive flexibility. The present findings, which showed a reduction in the sensation of dyspnea regardless of yoga experience, support the feasibility of yoga as a low-barrier intervention. Furthermore, this reduction supports previous reports that yoga may influence both the physical and perceptual dimensions of respiratory discomfort.7,11 However, many studies that focused on the sensation of dyspnea relied on subjective ratings or psychological scales and did not quantitatively evaluate dyspnea immediately under respiratory load in the context of yoga interventions. In the present study, respiratory discomfort was assessed more objectively by applying inspiratory resistance and analyzing the slope of dyspnea ratings. In addition, immediate post-intervention measurement helped minimize recall bias.
Considered together, these methodological features may offer preliminary insights into the clinical relevance of yoga-based interventions for other conditions where dyspnea is a prominent symptom but has not been objectively studied. Although the present study focused on healthy adults, dyspnea is a common feature across many clinical conditions, and clarifying the immediate physiological effects of yoga in controlled healthy subjects may help inform future investigations in clinical populations.
Pain
Following the yoga intervention, increased thermal pain thresholds were observed only among practitioners. The thermal stimuli primarily activate transient receptor potential vanilloid 1 (TRPV1), an ion channel sensitive to temperature. TRPV1 is activated by heat stimuli above 43°C. 38 Sustained TRPV1 activation has been implicated in the maintenance of chronic pain, and pharmacological antagonists targeting TRPV1 have been investigated in conditions such as neuropathic pain. 39 However, side effects such as impaired thermoregulation have limited their use. 40 In light of these limitations, non-pharmacological approaches to modulate TRP channel function have been considered as potential alternatives. Unlike previous cross-sectional studies, this research adopted a pre–post design to assess the immediate and direct effects of yoga on sensory processing.
Although TRPV1-mediated nociception is one possible pathway through which yoga might influence thermal pain thresholds, pain processing can be modulated at multiple levels, including peripheral receptor responsiveness, spinal gating, descending inhibitory control, autonomic regulation, and cognitive or attentional processes. Given that the present study did not directly assess neural activity or receptor-level function—and that no significant group-level differences in pain thresholds were observed—these interpretations should be regarded as hypothetical. The exploratory association between yoga experience and pain threshold changes suggests that long-term practice may engage cognitive or autonomic mechanisms, but this possibility requires confirmation in future studies using neurophysiological measures.
CVRR increased only among practitioners in the yoga condition. CVRR reflects respiratory-driven HRV, with RR intervals shortening during inhalation and lengthening during exhalation in healthy individuals. This pattern suggests that breathing style—particularly abdominal breathing with prolonged exhalation commonly used in yoga (inhalation:exhalation = 1:2)—may enhance autonomic regulation and pain tolerance. 41 Such breathing patterns are also known to promote relaxation, which may further contribute to pain modulation. Consistent with this hypothesis, prior research indicates that simply slowing the respiratory rate is insufficient for analgesia; instead, a lower inhalation/exhalation ratio is associated with greater pain relief.42,43 This breathing pattern is linked to increased baroreflex sensitivity, enhanced vagal activity, and greater HRV during exhalation, changes consistent with elevated CVRR and improved autonomic function. Importantly, relaxation itself is considered essential for pain modulation. 44
Interpretation of these HRV changes requires caution. Breathing rate was not recorded during the intervention, making it difficult to determine how much respiratory patterns contributed to CVRR increases. In addition, HRV segments were not analyzed with posture-normalized or artifact-corrected procedures recommended in recent guidelines, and individual differences in baseline vagal tone may also have influenced the results. These considerations suggest that the observed CVRR increases likely reflect an interaction between breathing behavior, autonomic flexibility, and individual physiological traits rather than a uniform yoga-specific mechanism.
Taken together, while these findings should be interpreted in light of the study’s methodological constraints, the increases in thermal pain thresholds and CVRR among practitioners point to a plausible interaction between sensory modulation, breathing quality, autonomic regulation, and relaxation effects.
Relationship between dyspnea and pain
No significant correlation was found between changes in dyspnea and pain thresholds. While dyspnea improved across all yoga subjects, pain modulation was limited to practitioners. These findings suggest that pain and dyspnea may be regulated through distinct mechanisms, and the therapeutic effects of yoga may emerge along different temporal and experiential trajectories for each symptom.
Limitations
The study has several limitations. The subjects included only East Asian adults, limiting generalizability. Cultural familiarity with yoga and population-level differences in sensory perception, respiratory discomfort, or autonomic reactivity may influence responses to the intervention, restricting applicability to populations with different cultural or physiological backgrounds.
The yoga intervention included multiple components (postures, breathing, and meditation), and the contribution of each to pain and dyspnea remains unclear. Dyspnea assessment focused solely on inspiratory resistance and did not evaluate discomfort during expiration. Breathing patterns were not directly monitored, so adherence to diaphragmatic or slow breathing cannot be confirmed. Moreover, the absence of an exercise-only control condition (e.g., stretching) limits the ability to determine whether the observed effects are specific to yoga practice rather than general physical activity.
Pain thresholds and dyspnea ratings were assessed only once, and the study did not evaluate the stability of these measures across repeated sessions or the persistence of the effects beyond the immediate response to a single yoga session. Regarding pain thresholds, the effect size observed in this study may have been small, and the statistical power may have been insufficient to detect subtle changes. In addition, psychological factors such as anxiety, depression, fear of pain, and expectancy were not assessed, and these unmeasured variables may have influenced changes in pain thresholds. Subgroup comparisons were limited by small sample sizes, and future research should include larger cohorts to validate these findings. Clarifying whether these immediate changes translate into sustained benefits will require future clinical studies.
The mechanistic interpretations discussed in relation to pain and dyspnea—such as TRPV1 involvement and autonomic regulation—remain hypothetical, as the present study did not directly assess neural activity or receptor-level function. Therefore, it remains unclear whether individuals who experience chronic dyspnea and pain would be able to perform the same protocol, and the generalizability of the findings to clinical populations is limited.
Conclusion
This study quantitatively demonstrated that a single yoga session significantly reduced the sensation of dyspnea under inspiratory load, regardless of prior yoga experience. Increases in thermal pain threshold were observed only in experienced yoga practitioners, with no significant correlation between the sensations of dyspnea and pain, suggesting distinct regulatory mechanisms. By employing immediate post-intervention assessments and quantitative measures in healthy adults, the study offers preliminary insights into symptom-specific physiological modulation and may inform future clinical research.
Authors’ Contributions
H.M.: Conceptualization, funding acquisition, data curation, formal analysis, methodology, project administration, visualization, writing—original draft, and writing—review and editing. T.O.: Resources and supervision. T.M.: Supervision. M.M.: Supervision. X.W.: Investigation and methodology and project administration. U.P.: Investigation and project administration. T.K.: Investigation. S.E.: Conceptualization, funding acquisition, methodology, resources, supervision, and writing—review and editing.
Ethical Considerations
This study was approved by the Ethics Committee of Tohoku University Graduate School of Medicine (Ethics Code: 2023-1-632) on June 13, 2023. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to Participate
All participants provided written informed consent prior to enrollment in the study.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Acknowledgments
The authors thank all the yoga instructors and participants for their generous time and commitment to this research. The authors also thank Bradley A. Morrison for his assistance with English proofreading.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Science and Technology Agency (JST) and the establishment of university fellowships toward the creation of science technology innovation (JPMJFS2102). In addition, partial support was received from the Research Funding for Longevity Sciences from the National Center for Geriatrics and Gerontology (22-1), Japan Society for the Promotion of Science (JSPS) KAKENHI (22K19760, 24K02778, and 25K22899), the Japan Agency for Medical Research and Development (AMED) (25zf0127001h0005), and the JST Strategic International Collaborative Research Program (SICORP) (JPMJSC2308).
Supplemental Material
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.