
Abstract
Purpose:
This article presents evidence from surveys and ethnographic interviews addressing family home health care practices and communication between families and their childcare providers about such practices. Drawing on research supporting the value of family-centered care (FCC) and consistency of care (COC) in childcare, researchers sought to understand the nature of at-home health care and health-supportive behaviors and practices among our research participants (families with young children) and to assess the extent to which families are comfortable sharing the nature of these practices with their providers.
Results:
Our findings suggest that families seek out and use a variety of health-supportive behaviors at home that they do not necessarily share with childcare providers. Such practices include a focus on healthful foods (including alternative diets that may go against official recommendations) as well as other simple practices like regular exercise, yoga, or gardening. The article presents the research study and its findings and presents a recommendation to develop an educational curriculum designed to support families and increase both Family-centered care (FCC) and Consistency of care (COC) by encouraging better communication between families and providers. The curriculum will support an aim to educate childcare providers on the benefits of some of the most common integrative health care strategies and provide practical examples for integrating these practices in professional and family-home childcare settings.
Highlights
Families use a number of different methods to care for their health that they do not consider to be health care. Families do not tend to share complementary or integrative methods of care with childcare providers. The most common complementary and integrative methods used are healthful foods, regular exercise, and yoga. Education is needed for parents and childcare providers to communicate and provide consistency of care.
Caring for Your Family’s Health: An Evidence-Based Curriculum
Purpose of the present study
Family-centered care (FCC), in which health care practitioners honor and consider families’ preferences and practices in health care services, is fundamental to providing effective care.1,2 The American Academy of Pediatricians (AAP) supports the provision of patient- and family-centered care in recognition of the importance of family in a child’s development and health. 3 In their policy statement, the AAP identifies the benefits of FCC, which include more robust relationships with families, improved clinical decision-making for providers, greater understanding of families, and more efficient use of health care resources, among other benefits.
Similar to the AAP’s recognition of the importance of FCC, the American Academy of Family Physicians promotes the concept of “continuity of care,” in which patients and physician-led care teams are “… cooperatively involved in ongoing health care management toward the shared goal of high quality, cost-effective medical care.” 4 The childcare community also supports the “consistency of care” (COC). Consistent care between childcare and the home relies heavily on having a strong positive relationship between the parents and the childcare provider, which is developed over time by having the same provider for several years. This relationship helps to establish communication, and both the provider and the parent are more likely to have the confidence to share concerns and preferences for the care of the child, 5 including cultural preferences, developmental needs, or safety concerns, as well as integrative health care methods. When childcare providers honor parents’ preferences for caring for the child, the child feels secure in the consistency, and the parent feels supported as the primary caregiver for the child. This support further enhances the relationship between the parent and provider, opening the communication pathway. Research shows this relationship supports the child and the family. 5
Providing consistency in care and clear communication about the child’s needs between parents and providers is beneficial to caring for the whole child, ultimately supporting the overall childcare program. When providers can see the positive outcomes for the child, they are motivated to coordinate even more communication with the family. 6 Research also shows that when providers and parents communicate effectively and engage as partners in the best childcare of the child, it reduces signs of burnout among providers. 7 By sharing integrative health care methods a family is using at home, the provider may gain a better understanding of the family’s individual beliefs and how those beliefs influence the family’s and the child’s behavior. An understanding of behavior can reduce stress on the provider and is shown to increase positive teacher–child interactions. 8
One of the core principles of FCC is that providers will facilitate choice for the child and family about approaches to care,
3
which include complementary and alternative medicine (CAM) and integrative medicine (IM). The National Institute of Health
9
provides the following clarifying distinctions regarding CAM:
If a nonmainstream approach is used together with conventional [bio-] medicine, it is considered “complementary.” If a nonmainstream approach is used instead of conventional [bio-] medicine, it is considered an “alternative.” Integrative health brings conventional and complementary approaches together in a coordinated way.
10
In this context of growing interest in integrative health, there is recognition of the place for IM in pediatrics. 11 In 2018, Esparham and colleagues reported that 12% of the general pediatric population and up to 80% of children with chronic conditions used pediatric integrative medical approaches. 12 Misra and colleagues 13 studied the use of IM at a large children’s hospital. They found that most patients and their parents had used CAM in the past year. Although integrative therapy is often requested (primarily to address pain), there is an inadequate provider supply. IM is comprehensive, especially regarding the number of practices considered “alternative” or “complementary.” It is not the purpose of this paper to review the myriad health practices that could be categorized as complementary or alternative, but the National Center for Complimentary and Integrative Health (NCCIH) identifies common complementary approaches.
Different practices are used for different reasons, and in health care delivery, health care providers must understand what practices (if any) a family chooses. This is an essential element of FCC, as it allows families to feel supported in their health decisions. Nonetheless, many people who employ complementary and alternative methods at home, including practices with perceived or measurable benefits for both physical and mental health, may be unlikely to inform their childcare providers about these home-based practices, in part because they may not define them as health care practices. 14 Most patients disclose CAM use when prescribed by a specific provider and directed at a specific medical condition. 15
COC is best achieved through relationship-building, trust, and communication between the family and the childcare provider. Children who receive inconsistent care regarding their health, specifically diet and physical activity, show unhealthy outcomes. 16 Consistent sweet drinks being offered, for example, in one location but not allowed in another creates confusion in the child and disrupts their ability to make healthy choices later in life. This type of situation, where either the childcare program or the parent is perceived to be undermining the other in decisions related to the care of the child, has an impact not only on the relationship between the parent and the caregiver but also between the child and the parent or caregiver. 17 Without that strong relationship, the child may display challenging behaviors stemming from insecurity in those relationships and may experience difficulty adjusting to the childcare setting due to inconsistencies. If the parent does not trust the caregiver, the child will also not. 7 According to Kelty and Wakabayashi, 18 withholding judgment regarding family decisions is one key element that lends itself to strong relationships and open communication. Across 10 focus groups, researchers found that participants frequently cited fear of judgment as a reason for not communicating family decisions or information about the child to the caregiver. Developing trust and communication helps the relationship form, allowing for more parent involvement in the program. Increasing parental involvement provides parents with another setting to share family beliefs about health, further solidifying the lifestyle behaviors modeled for the child and showing that these activities are valued not only at home but also in other settings. 19
In recognition of the importance of FCC and COC, as well as maintaining consistent relationships and routines between home and childcare settings, and in the context of the emergence of CAM, our study sought to examine the varied practices, beliefs, and preferences that families embrace as means to support health and well-being in their families and the perceived support they receive from their childcare providers to maintain their preferred practices. Families may need to communicate with their providers about the practices that are important to them for various reasons. Despite the rise of CAM and FCC, not all childcare providers may embrace the full range of practices families ascribe to, especially when it requires the provider to make accommodations for the child in their program. It might be easier, for example, to make accommodations when there is a prescribed medical reason, such as a peanut allergy, rather than for a parental preference, such as eliminating dyes in foods given to the child. Our study attempted to measure and evaluate FCC in a northeastern US state relative to family use of CAM so that we could target education and professional development for childcare providers to address the specific needs of diverse families in our region. The expectation is that the information from the study can be used to justify the development of a curriculum specifically aimed at childcare providers to educate on some common CAM practices as well as coach providers on how to begin conversations with individual families on this topic.
We hypothesized that childcare providers in this region are unaware of the wide range of practices that families use to support their health and well-being and that families are reluctant to share their priorities with their providers. However, with an increased understanding of the practices that families use in their daily routines, childcare providers will have the knowledge and tools to be more family-centered. Improving FCC will improve health outcomes for families in the region.
Hypotheses summary
Parents employ various beneficial complementary strategies that they do not necessarily consider health care strategies. Childcare providers are unaware of families’ strategies. Childcare providers, unaware of the importance of integrative health care, do not ask about strategies that families employ that may be considered “complementary” or “alternative.” When families share “complementary” or “alternative” strategies to support their children’s well-being, they do not feel supported by their childcare providers. When families use “complementary” or “alternative” strategies to support their children’s well-being, they encounter barriers in the childcare community. When childcare providers better understand families’ strategies, providers can increase FCC and continuity of care, thereby improving patient outcomes.
Methods
Sample
Research participants were recruited by email through two not-for-profit agencies that support families in three counties in a northeastern US state. One agency assists families in finding childcare based on the specific needs of the family while also providing direct support to childcare programs in achieving a high quality of care. The other agency provides direct care for children in a group childcare setting and supports families in providing developmentally appropriate experiences for their children. The two agencies sent recruitment emails to 1236 families to participate in this study. Of those 1236 families, 549 (44%) are identified as low-income. A “family” was defined as at least one adult head of household with at least one child under 12. The population of families in the area is culturally diverse due to the region’s attraction to immigrants and refugees. For example, approximately 25% of the region’s population in one urban area are immigrants or refugees. 20 Therefore, while the agencies utilized for recruitment do not have measures of their patient demographics beyond income, the expectation was that we would collect a culturally and socioeconomically diverse sample.
Instrument
Researchers developed survey questions using a Google Form. The first question was the indication of informed consent, and the final question was a place for respondents to enter their contact information if they wished to participate in an interview. The remaining questions included
demographic information on household size and income, respondents’ knowledge and use of various standard integrative health methods and questions about the respondents’ health insurance and family physician(s).
The researchers piloted the survey with five individuals, and feedback was used to adjust the wording of several questions for clarity and to increase face validity.
Design
The first consulting agency sent a recruitment email to 687 families across three counties in the region of study. The email included an overview of the project, a consent letter, participation requirements, and a link to the Google Form survey. A follow-up email to remind families of the opportunity to participate in the research was sent by the same agency to the same 687 families one week later, and the survey closed one week after that follow-up email. The second agency later sent a recruitment email to 549 families in two of the same counties and a follow-up email one week later, with the survey closing one week after that. Survey results were not associated with names or contact numbers. However, at the end of the survey, participants were invited to share such details if they would be contacted and interviewed for additional information.
One of the researchers conducted follow-up interviews via Zoom with two voluntary participants using a semi-structured method. Each interview was approximately an hour long and used an open-ended interviewing strategy. The researcher asked each participant to describe their family (number of household members and any demographic information such as education level, work, language spoken in the home, religious preferences, health concerns, or any other particularities that affected attitudes to health or health care). The interviewer also asked participants about their childcare arrangements and to describe their relationship with caregivers, including childcare and health care specialists, family members, and anyone else responsible for giving or making decisions about health and childcare for the family and children.
Results
Response rates
Of the 1236 families who received the survey, 51 families responded, and 4 of the 51 families indicated an interest in the interview portion of the research, resulting in just two individual interviews after multiple attempts to contact all 4 participants. The low survey response rate of 4% may suggest that families are not familiar enough with integrative health care practices to respond to such a survey, that they have different priorities, or perhaps that they do not identify practices they ordinarily employ as “integrative health care,” even if these might meet the definitions used in this study. The small number of respondents who also indicated an interest in a follow-up interview might indicate a lack of familiarity with this type of research or maybe a representation of the population—working families with small children at home, with little time to spare.
Demographics
Of the 51 families who responded, more than 90% have at least some college education (Fig. 1), and almost 65% have a household income over $75,000 (Fig. 2). This indicates that those confident and knowledgeable enough in integrative practices to respond to the survey are educated and in a higher income bracket than the same proportion of the population surveyed. At least 44% of the population who received the surveys are considered low-income. Participants ranged in age from 22 to over 50, with most respondents (61%) between 30 and 39 years old.

Education. Note: The tables were generated by Google Forms (2023).
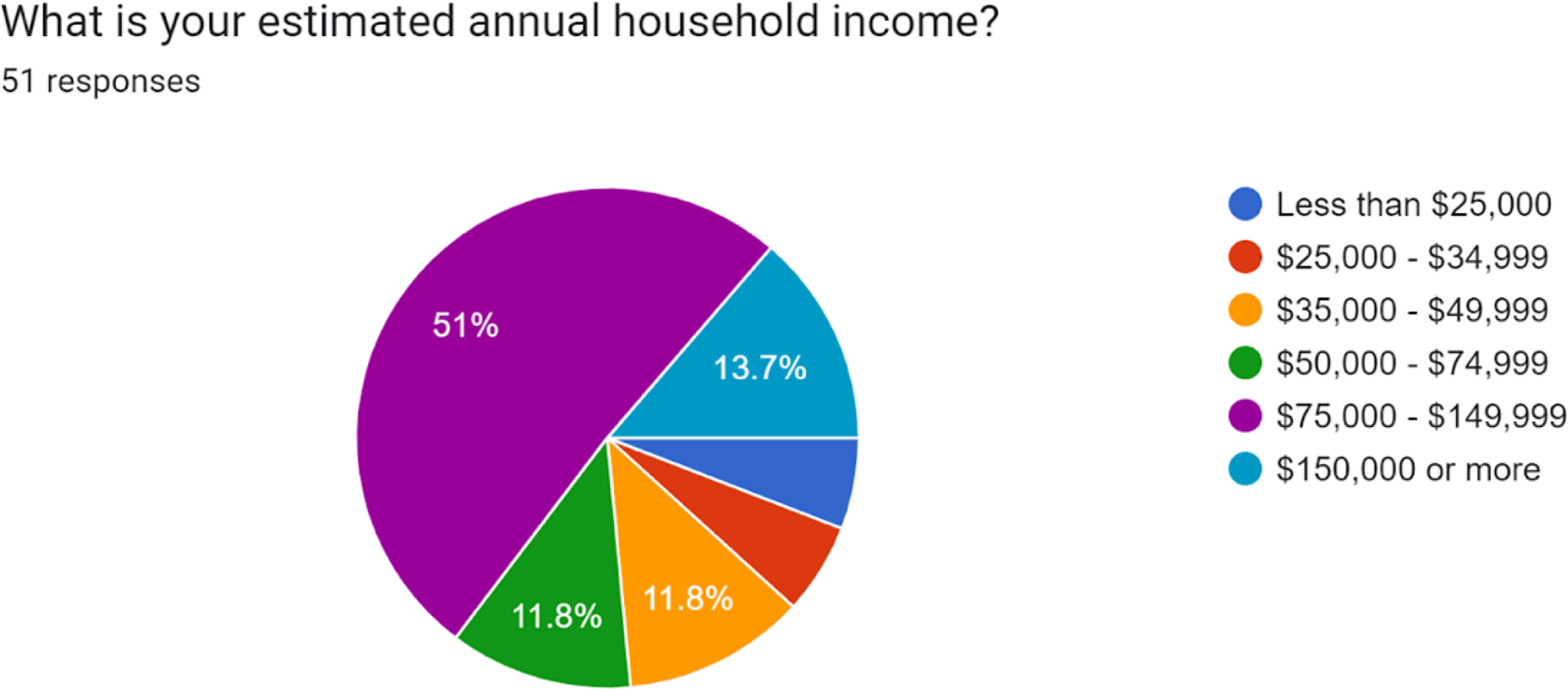
Income.
In addition to the responses on household income and educational attainment, almost all the respondents indicated they are employed: 86% indicated that they work full-time, and 12% work part-time. The remaining 2% indicated that they are currently retired. 80% of respondents reported having another household member contributing to the household income. When asked about the size of the immediate household, most respondents reported three or four people, including themselves (32% each). A small number of respondents (6%) reported having a household size of six or more, while the remaining indicated a family size of two or five (14% and 16%, respectively). Only three respondents indicated a large family of four or more children when asked about the number of children in the family unit. Most respondents indicated one, two, or three children (Fig. 3).

Number of children in family unit.
Most children included in the family unit were preschool aged (70% between the ages of 2 and 5). This is consistent with the populations served by the two agencies, as one assists families with locating childcare, and the other serves children in a group childcare setting. Because most families have more than one child, children under 2, 6–8 years old, 9–12 years old, and 13 years and older are also included in the data collected (Fig. 4).

Ages of children in family unit.
Health care Costs and Childcare Circumstances
Following the demographic questions, survey respondents were asked about their health insurance and whether adults and children regularly see a physician. The purpose of these questions was to gain an understanding of health care provided to families and payment arrangements. All respondents indicated that they have health insurance, with the majority having employer-supported insurance (75%). Twenty-four percent (24%) responded that they receive insurance through public assistance, which is higher than the 13% who reported a household income under $50,000. Ninety percent (90%) of the respondents have a primary health care provider they visit regularly. When asked, “Under what circumstances, in general, do you visit your physician or primary health care provider?” the majority of parents visit “as needed” while their children visit almost equally “as needed” or for “preventative care.”
Interestingly, the three families with four or more children only take their children to the health care provider “as needed.” A few families indicated that they or their children visit for chronic conditions (Fig. 5). Most respondents also reported that their children see a different practice or physician than the adults in the household.

Circumstances for visiting primary care provider.
Given that the data were collected through two agencies serving families alongside childcare programs, it is unsurprising that 70% of those who responded access some childcare (Fig. 6). The majority of those who responded that they access childcare indicated that they use an informal provider such as a relative, friend, or neighbor (24%) or through a licensed childcare center (18%). The remaining families access care through in-home registered or licensed families or group family providers, a nursery school, or a mixture of childcare types. For this survey, the following definitions were used: Informal Care (a relative, neighbor, or other individual who cares for a child and 1 or 2 other children, not licensed or registered); Registered Family Home (1 provider in his/her own home); Group family home (1 provider in his/her own home with an assistant); and Licensed Childcare Center (children cared for outside of a home, separated into groups by age).

Accessing child care.
Use of Integrative Healthcare
The final set of survey questions explicitly referred to types of integrative healthcare methods used by families, how often the methods are used, and how they are shared with their health care provider. From the initial list of integrative healthcare methods (acupuncture, animal-assisted therapy, aromatherapy, chiropractic care, cupping, herbal medicines and supplements, homeopathy, massage therapy, meditation, music therapy, reiki, and yoga), most families indicated that they had never tried any of them (Fig. 7).

Frequency of use of integrative practices.
For families who have used some integrative health care practices regularly, herbal medicines and supplements (which may include diet and nutrition) were indicated most frequently (20%), followed by chiropractic care (14%) and music therapy (10%). For those who indicated they used the methods “a few times,” 20% indicated that to be true for chiropractic care, 16% for massage therapy, 14% for yoga, and 10% for herbal medicines and supplements. For those who indicated they used the methods “when able,” 12% indicated that to be true for massage therapy, 10% for aromatherapy, and 8% each for chiropractic care, herbal medicines and supplements, meditation, and yoga. Respondents also could enter any additional practices they used for their families. Two people indicated they exercise, and two indicated “talk therapy.” Others wrote practices such as “fasting,” “mental therapy,” “speech OT,” “self-care,” and “stem-cell treatments.” When asked about the integrative health care methods listed on the survey or the ones they listed themselves, the majority (55%) reported that they do not consider any of those methods part of their health care routine. Respondents were also asked whether their health care provider recommended any of the practices. Eight percent (8%) reported that their provider recommended chiropractic care. Twenty-two percent (22%) reported sharing that they use the methods with their provider.
Interviews
While only two respondents were successfully engaged for the follow-up ethnographic interviews planned for this project (despite repeated attempts to contact all four volunteers), the information obtained here illustrated some critical trends in the survey data. Other information provided in the interviews, particularly the emphasis on food and nutrition, proved valuable because it was not specifically evident in the surveys. The two respondents were college-educated women—one a college graduate and the other with some college. Both were identified as White, with their religion unspecified, and English was the first and only language spoken at home. Both had male partners at home who shared responsibility for household expenses and child-rearing. Both had health insurance, but one, using the pseudonym Mary, had insurance through her employer, while the other, using the pseudonym Sarah, depended on public assistance. The two respondents offered differing characterizations of their family’s health situation, but both emphasized food habits and diet as central to this. Mary viewed herself and her family as having a relatively healthy lifestyle, having made recent health-promoting changes to diet and lifestyle. Sarah regarded herself and her family as still struggling to move toward a state of health but discussed several examples of dietary choices and habits playing a role in this journey and outlook. Both mentioned exercise and specifically yoga as supplemental tools they had used, along with diet, to improve health. Both respondents also had an arms-length relationship with primary care providers, using such services only when necessary and mainly in the context of pediatric routine visits or the case of specific health problems for their children, and both said they rarely shared details about their health-related routines with biomedical care providers. Both women also communicated with childcare providers for continuity of care, mainly in diet and food choices. Finally, both respondents referred to anomalous health problems as provocative of their turn to complementary or alternative approaches.
When asked to identify anything particular about her family that would help us understand her background, experiences, or attitudes toward health care, the first respondent, Mary, spoke about her adult younger brother’s autism. Watching her mother seek out different types of care and navigate the US health care system during their childhood greatly influenced her view of mainstream or biomedicine. “It was challenging to get him diagnosed in the first place, and then just having to kind of … not fight… but like really… have to push, to get the services that he needed, or get the doctors to understand what she was concerned about …. It… always felt like it was an uphill battle when it came to anything with him….”
Mary further explained her dissatisfaction with mainstream health care, saying: “I feel like nutrition is way overlooked when it comes to maintaining health and diagnosing stuff … .” She follows a low-inflammation or ketogenic diet (significantly reduced carbohydrate and increased fat consumption) and spoke at length about how she and her husband had used significant dietary changes to reduce weight and improve overall health. When asked about her family’s overall relationship with health care, she described herself as: “suspicious or questioning…. Like, I want to… go home and do all the research and see what other… people are saying, and what other options are there.” Mary also sees a chiropractor, whom she sought out due to back pain, and a mental health counselor, whom she sought out to address pent-up emotions that had resulted from having a newborn during the early phases of the COVID-19 pandemic. She works out (sometimes with a personal trainer), practices yoga, and rarely sees a mainstream biomedical provider. Mary had recently had a healthy pregnancy, with normal blood pressure and weight gain and “no swelling, no inflammation” while following a strict ketogenic diet. However, she still avoided sharing this information with her physician because “doctors are skeptical if you tell them that that is how you eat…. So I think I told my OB that I was more paleo….”
The second respondent, Sarah, struggles with weight and is working to make healthy changes to her own and her family’s diet but is also considering what she described as “weight loss surgery.” When asked about her general health care choices, she described avoiding most providers. “I still do not like going to the doctors and avoiding it at all costs. I am pretty sure I have two cavities, and I am not going to the dentist. It is not that I am scared of the dentist. I just… do not like going. I do not like what that bill will look like.” Recently, Sarah was diagnosed with diabetes, which gave her a scare and helped her decide to have weight loss surgery, so she is currently seeing a provider who will perform the surgery once she is ready.
Regarding health care expenses, Sarah mentioned concern about dental bills but was also careful to note, after a follow-up question, that cost has not been a factor in her health care choices. “It is not that I could not afford it. It is just ingrained.” She explained that she has other, higher priorities and would rather spend money on those than on health care bills. Sarah emphasized several times that while she does not budget or plan for health care expenses, she generally finds them manageable. “I am pretty spontaneous with things that I do,” she remarked and might find it easy to spend more money on an impulsively chosen activity, even if she is putting off having a couple of cavities filled. Sarah is not physically active. When asked about physical activity, she said: “Not that … dedicated towards exercise. I will go to the zoo with my daughter, walk to get ice cream, or… I’m not a couch potato, but… I do not usually do things just for exercise….”
When asked about continuity of care related to childcare, Sarah focused on food. She mentioned preparing fruit and vegetable trays to leave out at home to encourage healthy snacking. She also shared that she had recently planted a garden with a family member to support her mental health. With her daughter’s caregivers, Sarah asks that there be a vegetable provided at each meal; she encourages the same kind of healthy snack tray she uses at home, and she could only think of one time when she had needed to provide instructions for doctor-prescribed medications (for a time-limited issue).
Mary, too, mentioned a continuity of care issue about food with her child’s daycare during an aside about whether it has been difficult to follow a ketogenic diet while having a child at home. Mary said she wants to offer healthy choices but finds it more complicated when he is out of her care for part of the time. “They have all the fun stuff at daycare, and… he will say, like, oh, ‘breakfast bar,’ and I [say] ‘No, sorry, mommy does not have breakfast bars here, but when you go to daycare, you can have one. You can have scrambled eggs today here.’” Moments later, the interviewer asked: “[Have you ever] had the need… to communicate about practices that you do at home… with your childcare provider?” Sarah replied:
We’ve just kind of gone with the flow… Like, we realize he’s going to eat different stuff there, and… he’s three, [so] he’s gonna… eat whatever is there. We also recognize that the direction we go with our nutrition is very opposite to the standard American diet and what federal regulations require, like schools and daycare, and anything like that, to feed and provide to kids.
Though the interview sample size here is small, the two interviews, taken together, point to a vital overlap: diet and nutrition were seen as a primary supplemental or complementary health care practice by both respondents, and both saw mainstream health care providers as, at best, a low priority in their overall health maintenance and, at worst, an interference. Communicating about health-supporting behaviors with caregivers was an issue for both. Sarah was trying to make new healthy choices for herself and her family. She found it most straightforward to distill her preferences to “one vegetable per meal” as an instruction for childcare providers. On the other hand, though she and her husband had more established habits around their dietary choices, she chose to go “with the flow” and temporarily suspend her family’s values while her son was with childcare providers. She also recognized that her family’s preferences went against federal recommendations for pediatric nutrition and did not want to impose this on professional caregivers.
While seemingly of little consequence, Mary’s and her husband’s compromise represents precisely the obstacle to communication or continuity of care that this study and resulting curriculum are intended to address. Both participants’ health needs and interests suggest that diet, exercise, and practices to support mental health (e.g., counseling, exercise, gardening) can all be considered necessary supplemental or complementary health-promoting practices but may not be discussed with providers. Both participants mentioned having tried yoga at home. Mary had also worked with a personal trainer and received regular massages. At the same time, Sarah sought out yoga “mommy and me” classes on YouTube and had newly taken up gardening for support with ongoing mental health challenges. Both participants also mentioned having worked with counselors for mental health support.
Our curriculum is designed to support families’ empowerment around dietary choices and to support the view of these choices as health care practices and health care values. Combined with this, our curriculum supports mindfulness and restorative movement with yoga practice to encourage healthy body weight and positive mental health. A curriculum to support childcare providers’ knowledge and understanding of alternative diets and the health-supporting benefits of certain foods can help us to ensure that the educational pathways here are back and forth, with childcare providers and families both having the opportunity to learn about more supportive habits.
Discussion
Implications for practice
The survey response rate of 4% could indicate that families do not use complementary or alternative strategies to support their families’ health or that they did not see value in completing the survey. Both possibilities support the development of a curriculum to teach parents and caregivers about integrative health care. Moreover, teaching families and providers about the relationship between the identified integrative practices and positive health outcomes is an essential goal since most respondents reported that they did not consider the identified practices part of their “health care” routine. The survey results suggest to us that a curriculum designed for childcare providers to teach about integrative health care practices could help to achieve the following goals:
Caregivers will identify practices as integrative health care: What practices are considered “complementary,” “alternative,” and “integrative,” and why are they identified as such? Caregivers will identify specific practices families may be using or could use at home and that can be carried into the childcare settings that support the health and well-being of children and families. Childcare providers will learn ways to ask appropriate questions that create space for parents to share integrative health care practices that will achieve improved outcomes related to COC and FCC.
In addition to the justification for these specific goals based on the survey results, the researchers aimed to develop a strong support for a curriculum by agencies that support families and childcare providers. These agencies continually seek evidence-based practices and information to keep families informed about strategies to support family/child well-being, and the research team saw value in exploring this topic with the community.
Curriculum development
Considering the implications identified above, the researchers met to discuss the findings and the specific practices that could be taught to families in their homes and childcare settings that support their children’s and their families’ health and well-being. The researchers agreed on three practices: (1) diet/nutrition practices, (2) yoga postures and breathing exercises, and (3) meditation/mindfulness practices. These were selected because they are practices adults can implement with children without adding a third party and intensive special training, which could be cost-prohibitive.21,22 Second, they are practices for which evidence supports their effectiveness. Moreover, “herbal medicine/supplement” use (which may include nutrition/diet since that was not a specific practice mentioned in the survey) was one strategy that 10 survey respondents said they used “regularly” already. Diet was a key theme discussed in interviews (as described above). Therefore, we included diet/nutrition in the curriculum. Finally, given the strong evidence that supports meditation and yoga as helpful for coping with stress, which is often elevated for families with fewer resources and can have adverse long-term effects on health, these yoga and meditation were logical additions to the curriculum.
Moreover, one of the researchers is a yoga instructor with many years of experience teaching children and families, making yoga, meditation, and mindfulness an obvious choice for addition to the curriculum. For our purposes, we briefly discuss the literature supporting the three practices we chose to include in the curriculum. The order in which they are presented below is not meant to suggest a hierarchy of effectiveness or preference. It is meant to provide some narrative and empirical support for the practices selected for the curriculum.
Evidence and justification for choice of specific integrative health practices
Meditations/mindfulness practices
As indicated earlier, IM has already emerged in pediatric hospitals; it is often used to control pain and improve mood. 13 Jong and colleagues 23 found that both hypnotherapy and transcendental meditation were effective techniques for children coping with stress, which is a headache trigger. Pandya 24 found that meditation improved the self-control of children who had been diagnosed with attention deficit hyperactivity disorder. In addition to helping children, meditation has also been shown to be effective for parents. Kirby and Laczko 25 found that parents who practiced loving-kindness meditations had more positive and less negative emotional responses, such as frustration or anger, in responding to challenging behavior with children.
Yoga
The NCCIH reports that the American Academy of Pediatrics recommends yoga for children and adolescents to address emotional, mental, physical, and behavioral health conditions. 10 Fukuhara and colleagues 26 found that yoga, used as a therapy for children with cancer or a blood disorder, was adequate to decrease pain in children and decrease anxiety for adolescents and their parents. In addition, Saxena and colleagues 27 found that yoga improves attention and hyperactivity in high school students and suggests that adolescents could benefit from yoga in their daily routines to mitigate stress. According to the Centers for Disease Control and Prevention, childhood anxiety and depression are rising at alarming rates. From 2016 to 2019, 9.4% of children aged 3–17 years (approximately 5.8 million) had been diagnosed with anxiety, and 4.4% of children in the same age group (approximately 2.7 million) had been diagnosed with depression, 28 —and those figures were pre-COVID-19 pandemic! These figures alone justify the importance of teaching children and families strategies such as yoga to help improve their overall well-being.
Diet, nutrition, and supplements
The survey of families in Central New York reflects the usage of herbal supplements (20% of those surveyed reported “regular” usage), which is consistent with the nearly 20% (17.7%) of “natural products” reported by NCCIH at the national level. Because the regular usage of herbal medicine/supplements far exceeded all other practices, and because families may not consider this practice to be part of health care, which they report to their health care provider, there is an opportunity to educate families and caregivers about the use of natural products, and how dietary supplements, as well as nutrition and dietary choices, can impact overall well-being. New research in “culinary medicine” suggests that giving families and caregivers simple tools, skills, and knowledge to prepare healthy meals can transform health.29,30 Moreover, some families may target specific developmental challenges or medical/developmental diagnoses with diet and supplements. Trudeau and colleagues 31 found that 75% of children with Autism Spectrum Disorder in their study (n = 210) consumed supplements, including supplements such as adrenal cortex extract, that do not have product safety information related to their use. Trudeau and colleagues 31 also report that 33% of parents should have disclosed their child’s supplements to their physician. As indicated earlier, many families use CAM to control pain. Groenewald and colleagues 32 estimated that as many as 26.6% of children had pain conditions in the past year of their study, and of those, 21.3% used CAM, with special diets and herbal supplements being the practice most frequently used. Despite the lack of oversight by the Federal Food and Drug Administration of dietary supplements, it is evident that many people, including families with young children, use dietary supplements. This is justification for including diet and nutrition practices into the curriculum; the topic calls for family and provider education—not necessarily to promote the practice of taking dietary supplements, but to educate families about the importance of communicating about their use with their providers. Continuity of care can also be improved with a curriculum that empowers families to consider their dietary choices and nutrition as “health care” and to communicate their values and preferences to health care and childcare providers.
As the acceptance of IM and health care has grown, consumers should expect to see evidence of strategies such as meditation, yoga, and dietary supplements to grow. There is already a broad evidence base for many practices. However, the question remains: Do families understand these practices to be part of their health care routine, and do they communicate their practices to their childcare and health care providers to benefit COC and family-centered practice? The curriculum from this study aims to address these questions and support families and childcare providers to understand complementary and alternative health care practices as part of a health care routine that should be communicated to both health care and childcare providers for the sake of family-centered practice and COC.
Next steps (future research)
The survey data confirmed our initial hypothesis regarding families’ use of integrative health care at home and their need for greater communication with childcare providers about these practices. Two ethnographic interviews supported our hypothesis and provided additional insight into diet and nutrition as at-home strategies that families employ to support health but do not share with health care or childcare providers. As noted above, diet or nutrition may count under the integrative health care heading “herbal medicines and supplements.” However, since the initial survey did not ask directly about food or dietary choices, this would be something to spell out in future research. A survey including a separate category for diet/nutrition as one of the listed types of integrative health care would have yielded even more positive responses or may have prompted survey participants to think about other at-home strategies they use. Since part of the study’s findings include that families may not conceive of some of their at-home practices as “health care,” even if they might legitimately be claimed as such, future studies could perhaps employ additional language in the initial call for participants, including the words “diet” or “nutrition” as part of the invitation or references to other known health-promoting behaviors that families engage in, like exercise, gardening, or mental-health counseling, rather than referring more generally to “strategies that parents use to support their children’s health”.
Given the small sample size for interviews and since both interview participants were of similar age and demographic (college-educated, white women with male partners at home, raising one child each, on a relatively comfortable budget), additional interviewing encompassing a more diverse population would help us to understand how people of various backgrounds feel about and communicate their home practices about mainstream providers, if any. Snowball sampling, drawing on the recommendations of people already interviewed, might help boost response, though more might be needed to directly address the problem of the limited demographics. Posting flyers or using social media to recruit, survey, or interview participants through local ethnic community centers or markets may be a better way to achieve more diversity in the responses. They could also expand the number of practices considered integrative health care, which would help make the curriculum more robust.
Finally, future research should seek to substantiate the notion that doing what is best for children is what is best for the childcare program. This is a widely accepted concept among child and family scientists and was an underlying assumption of our research. However, our review of recent literature has identified a potential gap in research studies that support this notion with evidence.
Conclusion
Our hypothesis at the start of this study was that parents employ a range of strategies they do not consider “health care” strategies, that childcare providers in this northeastern US state do not know about the wide range of practices that families use to support their health and well-being, and that families are reluctant to share their priorities with their providers, or when they do, they feel unsupported. While our survey did not attempt to ascertain provider knowledge, it did confirm our hypothesis about families’ reluctance to discuss alternative health care approaches from home with their childcare providers. Ethnographic interviews further supported the finding that families with young children engage in a range of practices that they only minimally distill into simple instructions for childcare providers, as necessary. One family indicated reluctance to share practices that go against official recommendations, such as alternative diets, even when they had experienced personal health benefits from these practices. Another pointed to weight-loss surgery as the next step in managing a recent diabetes diagnosis, suggesting a physician-managed approach (even one as costly and risky as surgery) was preferable to behavioral or lifestyle adaptations that might be less clearly mapped to health care and receive less support or require more personal initiative. While the sample size here was small, both conversations along with the survey results suggest the potential benefits of a curriculum designed to: First, help families understand and value diet, nutrition, yoga, and mindfulness as health care; and, second, help families feel supported pursuing diet, nutrition, yoga, and mindfulness practice at home and in communicating this home health care and the associated values to both health care and childcare providers.
We further hypothesized that with an increased understanding of families’ practices in their daily routines, health care and childcare providers will have the knowledge and tools to be more family-centered. In addition, improving FCC will improve health outcomes for families in the region. A second aim of the curriculum is to introduce childcare providers to simple techniques they can use to teach and support mindfulness, yoga, and healthful eating to children, offering support and continuity for what is happening at home. Given the importance of communication and relationships between parents and providers, there is an opportunity for education and training designed specifically for childcare programs on how to open lines of communication with parents and how to integrate health care practices to create a COC between home and childcare. Families caring for their health and creating opportunities for COC will benefit all!
Authors’ Contributions
All authors were responsible for the conceptualization, investigation, funding acquisition, methodology, project administration, resources, validation, visualization, and writing of the original draft, review, and editing. Dr. Hallock and Dr. Scienza were primarily responsible for data curation and formal analysis of the quantitative data, and Dr. Klepinger was primarily responsible for the qualitative data.
Footnotes
Author Disclosure Statement
The authors have no known conflict of interest to disclose.
This research was exempt from full IRB review for the protection of human research subjects.
Funding Information
This study was supported by Utica University’s Institute for the Study of Integrative Healthcare.