
Abstract
Introduction:
Ankylosing spondylitis (AS) is a chronic inflammatory disease characterized by pain, stiffness, and progressive joint deformities. While pharmacological treatments remain the standard approach, adjunct therapies like whole-body cryotherapy (WBC) have gained attention for their potential benefits in reducing pain and inflammation. However, the effectiveness of WBC in AS remains unclear.
Methods:
A systematic search was conducted in PubMed, Scopus, Web of Science, and Embase for studies published up to November 2024. The study followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and was registered in PROSPERO (CRD42024620792). Primary outcomes included disease activity (Bath Ankylosing Spondylitis Disease Activity Index [BASDAI], Ankylosing Spondylitis Disease Activity Score [ASDAS]) and pain intensity (VAS), while secondary outcomes assessed function (Bath Ankylosing Spondylitis Functional Index [BASFI]) and inflammation (C-reactive protein [CRP]). Effect sizes were calculated using Cohen’s d, with heterogeneity evaluated through Cochrane’s Q-test and Tau2 variance.
Results:
Five studies involving 310 patients met the inclusion criteria. Tau-squared was estimated as zero, indicating a common effect size across studies with no dispersion of true effects. Intervention protocols varied in temperature (−60°C to −10°C) and session duration (80 sec to 3 min). WBC significantly improved BASDAI (p < 0.001), ASDAS (p = 0.015), BASFI (p = 0.006), and VAS pain scores (p = 0.005), demonstrating a strong therapeutic effect. However, no significant impact was observed on CRP levels (p = 0.684).
Conclusion:
WBC significantly improved pain, function, and disease activity in patients with AS. As a promising nonpharmacological adjunct therapy, further research is needed to optimize protocols and evaluate its tolerance and long-term efficacy.
Introduction
Chronic rheumatic diseases such as spondyloarthritis represent a major public health concern. 1 Although the emergence of recent therapeutics, including biological disease-modifying antirheumatic drugs (bDMARDs), has revolutionized the management of patients with spondyloarthritis, these therapies remain expensive and not without risks, especially infectious risk. 2 In this context, the development of adjunct therapies was necessary.
Among adjunct therapies, cryotherapy was tested in a wide range of musculoskeletal diseases including osteoarthritis,3,4 fibromyalgia,5,6 shoulder capsulitis, 7 and rheumatic diseases such as rheumatoid arthritis8,9 and ankylosing spondylitis (AS).10–14
Cryotherapy is defined by the application of superficial cold as a therapeutic agent. Cryotherapy application might be local, involving ice bags, ice baths, gel packs, ice massages, vapocoolant sprays, or chemical cold packs. 15 It might as well be nonlocal such as whole-body cryotherapy (WBC). WBC is represented by a large chamber fitting up to four, spreading cold by injecting cooled nitrogen with oxygen into the chamber or by circulating nitrogen within the chamber walls. 15
Cryotherapy has been recognized as a pain reliever for both acute and chronic pain. 15 Since then, physicians still prescribe it today as an effective way to alleviate pain. While the exact mechanisms underlying these benefits are not yet fully elucidated, several theories have been proposed, including reduction of oxidative stress, modulation of inflammation and edema, and alteration of nerve transmission in pain fibers. 16
A systematic review published in 2014 has suggested the efficacy of cryotherapy in inflammatory rheumatic diseases as an adjunct therapy to DMARDs, targeted biological treatments, nonsteroidal anti-inflammatory drugs (NSAIDs), and corticosteroids by decreasing the level of pro-inflammatory cytokines. 17
The aim of the present systematic review with meta-analysis was to assess the efficacy of WBC for pain, disease activity, and function in patients with AS.
Methods
A systematic review with meta-analysis was reported in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 18 It has been registered in PROSPERO under the number CRD42024620792.
Strategy search
Two authors (S.B. and O.S.) independently performed an online literature systematic search using the PICO (Patient, Intervention, Comparison, Outcome) strategy on the efficacy of WBC in A.S. The following online databases (PubMed, Scopus, Web of Science, and Embase) were investigated for potentially eligible studies published until November 2024.
The search strategy combined both MeSH terms and free-text keywords to ensure a comprehensive retrieval of relevant studies. The following combination was used: (“Cryotherapy” [MeSH] OR cryotherapy) AND (“Spondylarthritis”[MeSH] OR “ankylosing spondylitis” OR spondylarthritis). The two authors (S.B. and O.S.) also performed a supplementary hand search of the references of the retained articles and the references of the other systematic reviews to gather additional articles.
Studies selection
The two authors (S.B. and O.S.) independently reviewed all the generated articles for relevance. Articles not in the topic, duplicate publications, cohort studies, case reports and case series, letters, editorials, comments, systematic literature reviews, and meta-analysis were excluded. Then, supplementary screening was consecutively done by title, abstract, and full text to determine the final eligible articles. Discrepancies in the selection process were resolved through discussion and consensus. All authors agreed on the final decision of the included studies.
Outcome measurements
The primary outcome measures were disease activity, assessed by the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) 19 and the Ankylosing Spondylitis Disease Activity Score (ASDAS), 19 and pain intensity, measured using the visual analogue scale (VAS) (0–10).
The secondary outcome measures included function, assessed by the Bath Ankylosing Spondylitis Functional Index (BASFI), 20 and inflammation, assessed by C-reactive protein (CRP) levels.
Study quality assessment
Both randomized controlled trials (RCTs) and non-RCTs were included to comprehensively evaluate the efficacy of WBC. The quality of RCTs was assessed using the Cochrane Risk of Bias tool (RoB 2),202 which evaluates five domains including the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. For nonrandomized studies, we used the ROBINS-I tool,203 which assesses risk of bias across seven domains including confounding, participant selection, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of reported results. Two authors (S.B. and O.S.) independently evaluated the studies and resolved disagreements through consensus with a third reviewer (S.B.D.).
Data extraction
Two authors (S.B. and O.S.) independently extracted the data from the retained studies. Disparities were settled after discussion with a third author (S.B.D.). Data from the eligible articles were extracted based on the following categories: (1) Study characteristic (date of publication, year, country, study design, and recruited sample size); (2) population characteristics (gender, mean age); (3) disease characteristics (disease duration, phenotype, treatment); and (4) data related to cryotherapy (technique, temperature applied, protocol duration).
Evaluation of effect size
Overall estimates of the effect were calculated using Cohen’s d index. Cohen’s d index (the standard difference in mean) was used to calculate the effect size of continuous data. It is defined as the raw difference in means divided by the standard deviation (computed within groups and pooled). This index transforms the outcomes into a common metric.

Forest plots summarized the data using a random model.
Publication bias was evaluated using the Funnel plot and Egger’s test, followed by the Duval and Tweedie’s Trim and Fill methods, and sensitivity analysis was performed with the “One study removed method.”
Assessment of heterogeneity
We calculated the Cochrane χ2 test (Q-test), variance Tau2, and 95% predictive interval (PI). Comprehensive meta-analysis software version 4 was used for all calculations.
Results
Retrieved articles
We identified 53 potentially eligible studies. We excluded 32 studies after screening the title. Five additional studies were excluded after the screening of the abstract. Full-text screening led to the exclusion of one study. Finally, we included five eligible studies in our review. The PRISMA flow diagram illustrating the review selection process is shown in Figure 1.
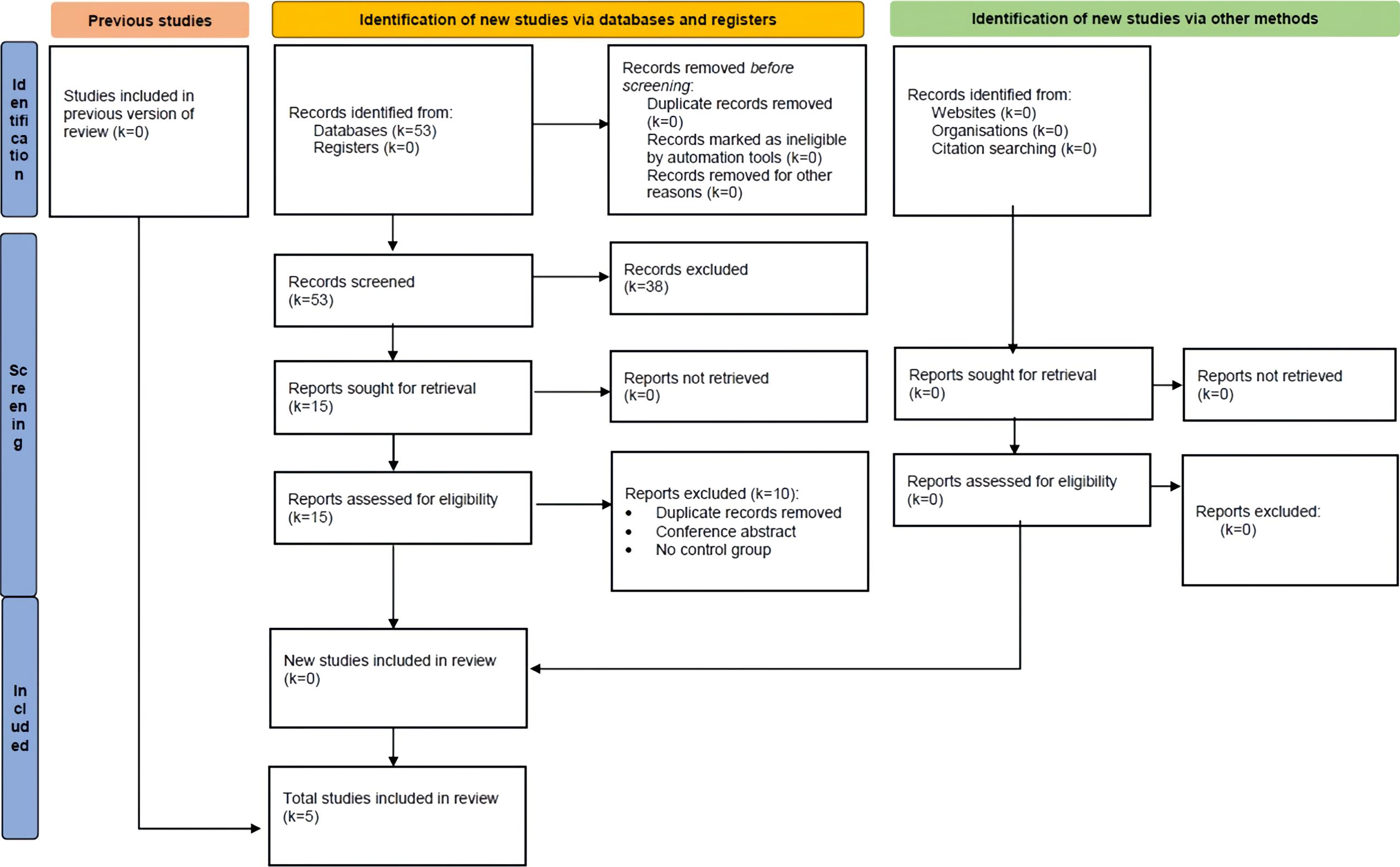
Flowchart illustrating the number of included and excluded articles at different steps.
Quality assessment of the included studies
The results of the risk of bias assessment for the included studies are summarized in Table 1.
Quality Assessment of Selected Studies
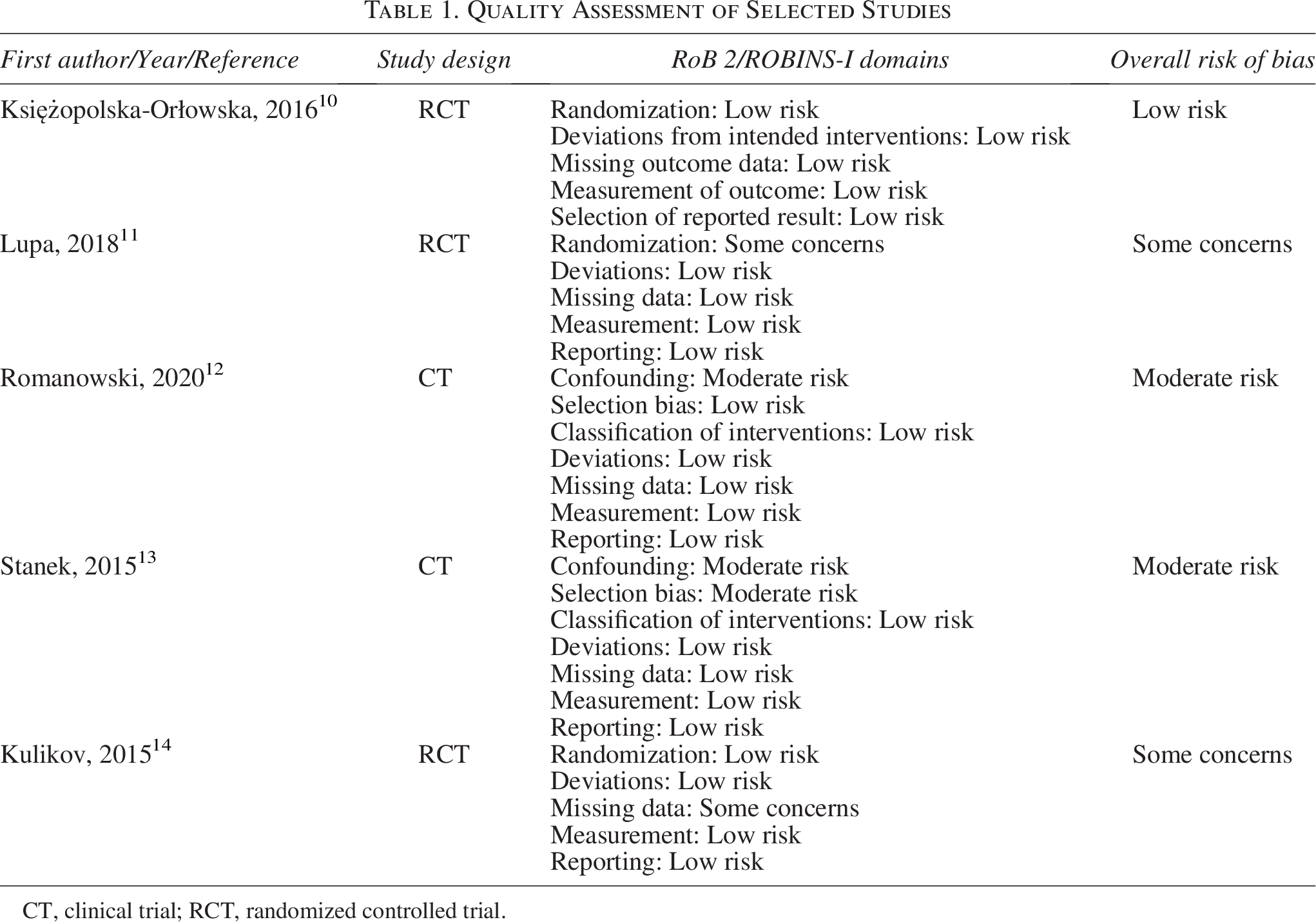
CT, clinical trial; RCT, randomized controlled trial.
Studies characteristics
Of the five included studies, four were conducted in Poland10–13 and one in Russia. 14 All studies were published between 2015 and 2020. Sample size ranged from 50 to 92. Overall, 310 patients were included. Mean age of participants ranged from 42.34 to 50.8 years. Male-to-female ratio was 6.38. Two studies were based on male patients.10,13 All patients had their diagnosis confirmed based on the modified New York criteria for A.S. Three studies were randomized controlled trials.
The intervention used in all studies was WBC administered in a cryogenic chamber.
Four studies11–14 used −110°C; in two of them,11,12 both −110°C and −60°C were assessed in separate subgroups. One study 10 did not report the exposure temperature.
The duration of WBC sessions ranged from 80 sec to 3 min daily. The length of the session was not recorded in one study. 10 Participants had had an 8- to 10-day intervention with a break on Saturday and Sunday in three studies.11–13 WBC was administered three times a week during 3 weeks in one study. 10 The number and frequency of sessions were not recorded in one study. 14 In addition to WBC, both intervention and control groups underwent the same physical therapy program. Patients on pharmacologic therapy had their treatment unchanged during the period of the study.
Disease parameters were assessed at the end of the intervention for all studies.
The main characteristics and results of the included studies are shown in Table 2.
Characteristics of Studies and Population
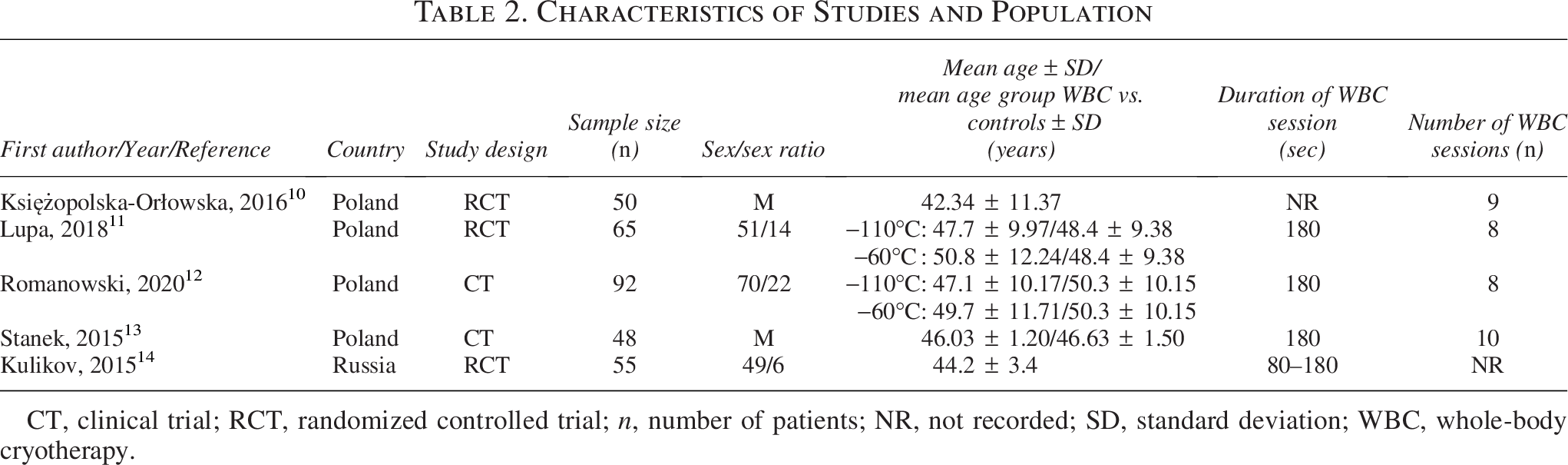
CT, clinical trial; RCT, randomized controlled trial; n, number of patients; NR, not recorded; SD, standard deviation; WBC, whole-body cryotherapy.
Meta-Analysis
BASDAI
The analysis included five studies10–14 (Fig. 2). In practice, the analysis is based on seven studies (five included studies with two subgroups). The mean effect size was the standardized difference in means. The random-effects model was employed for the analysis, which will be used to make an inference to that universe. The studies in the analysis are pulled from the literature; this is the model we should be using. This model allows us to generalize to the universe of comparable studies. The mean effect size was −0.526, with a 95% confidence interval ranging from −0.738 to −0.313 (p < 0.001). The variance of the true effect size Tau2 was zero, and the PI corresponded to one point. All indices of heterogeneity (I-squared, tau-squared, and tau) are set to zero. In practice, there is no heterogeneity. However, given the limited number of comparisons (n = 7), the estimation of heterogeneity (Tau2 = 0) should be interpreted with caution, as the meta-analysis may be underpowered to detect true between-study variability.

Forest plot of the effect of whole-body cryotherapy on mean BASDAI scores. Results favor cryotherapy. Lupa et al. 11 and Romanowski et al. 12 contributed two subgroups each, corresponding to treatment arms with different cryotherapy temperatures: −60°C and −110°C. These subgroups were analyzed as independent comparisons. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index.
ASDAS
The analysis was based on two studies)11,12 (Fig. 3), providing four subgroup comparisons, corresponding to distinct cryotherapy treatment arms (−60°C and −110°C). The mean effect size was −0.342, with a 95% confidence interval of −0.617 to −0.067 (p = 0.015). No heterogeneity was mentioned.
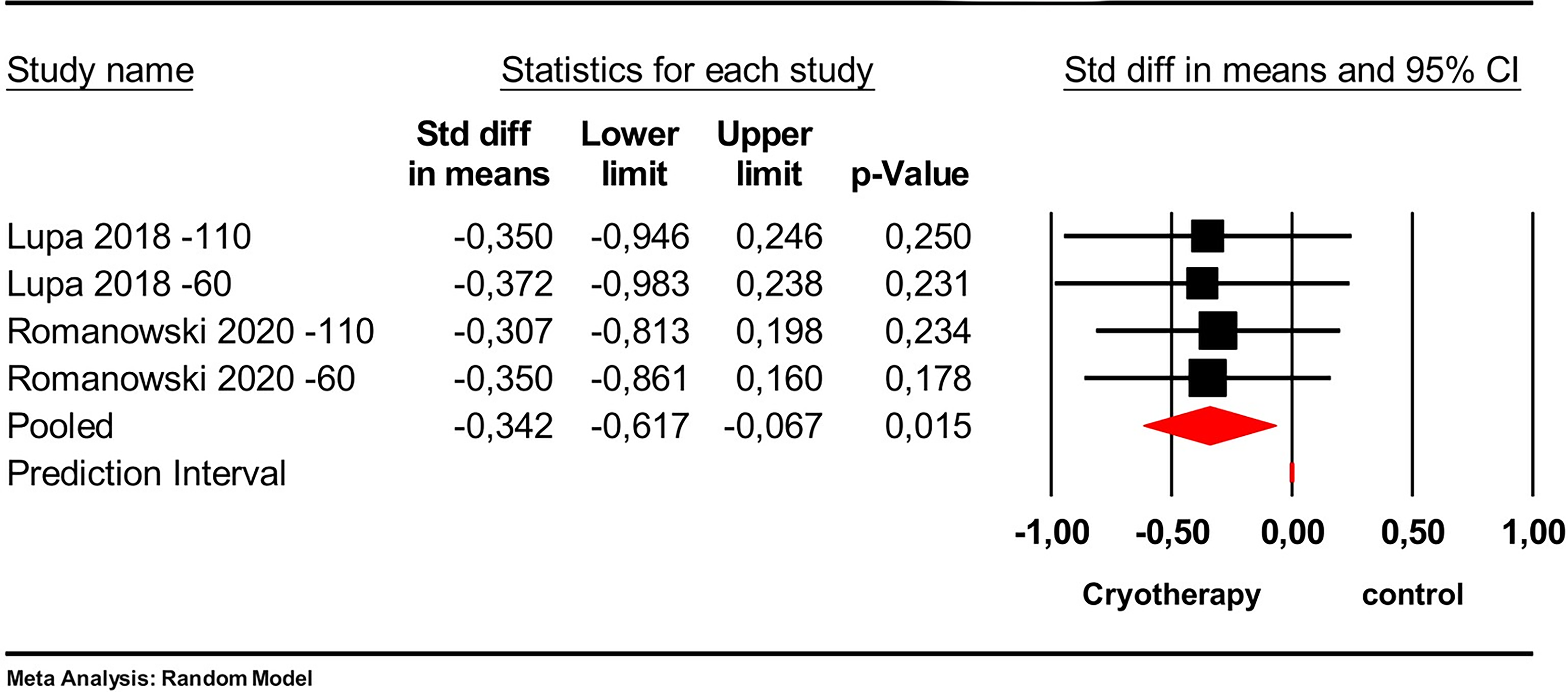
Forest plot of the effect of cryotherapy on mean ASDAS favors cryotherapy. Std, standard deviation. Lupa et al. 11 −60: −60°C treated subgroup. Lupa et al. 11 −110: −110°C treated subgroup. Romanowski et al. 12 −60: −60°C treated subgroup. Romanowski et al. 12 −110: −110°C treated subgroup. ASDAS, Ankylosing Spondylitis Disease Activity Score.
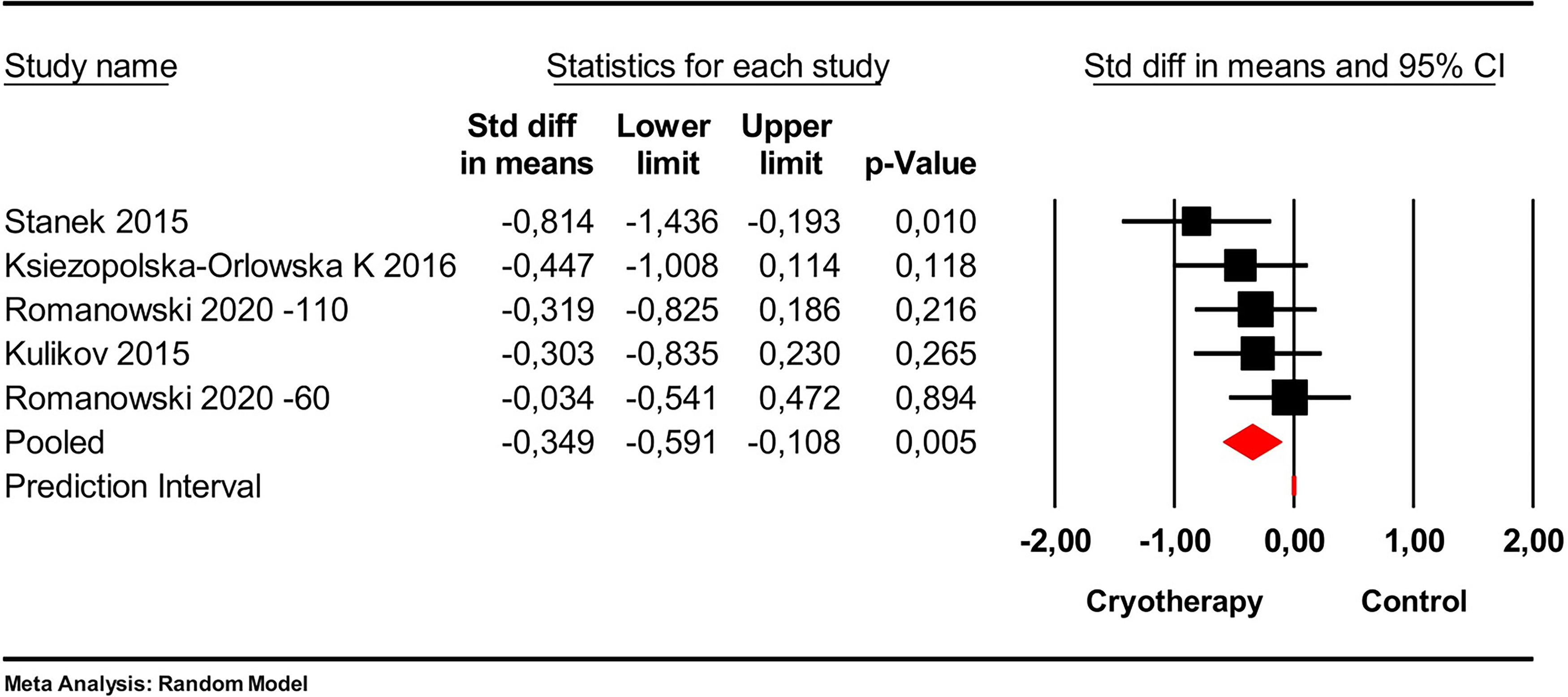
Pain
The analysis included four studies10,12–14 with five comparisons, including two subgroups from Romanowski et al. 12 corresponding to different WBC temperatures (−60°C and −110°C), which were analyzed independently. The mean effect size was −0.349 with a 95% confidence interval of −0.591 to −0.108 with p = 0.005 (Fig. 4). No heterogeneity was mentioned.
C-reactive protein
The analysis was based on three studies (one study with four subgroups)11,12,14 (Fig. 5).

Forest plot of the effect of cryotherapy on mean C-reactive protein (CRP) showed no significant change. Std, standard deviation. Lupa et al. 11 −60: −60°C treated subgroup. Lupa et al. 11 −110: −110°C treated subgroup. Romanowski et al. 12 −60: −60°C treated subgroup. Romanowski et al. 12 −110: −110°C treated subgroup.
The mean effect size was −0.050 with a 95% confidence interval of −0.293 to 0.192 (p = 0.684). No heterogeneity was mentioned.
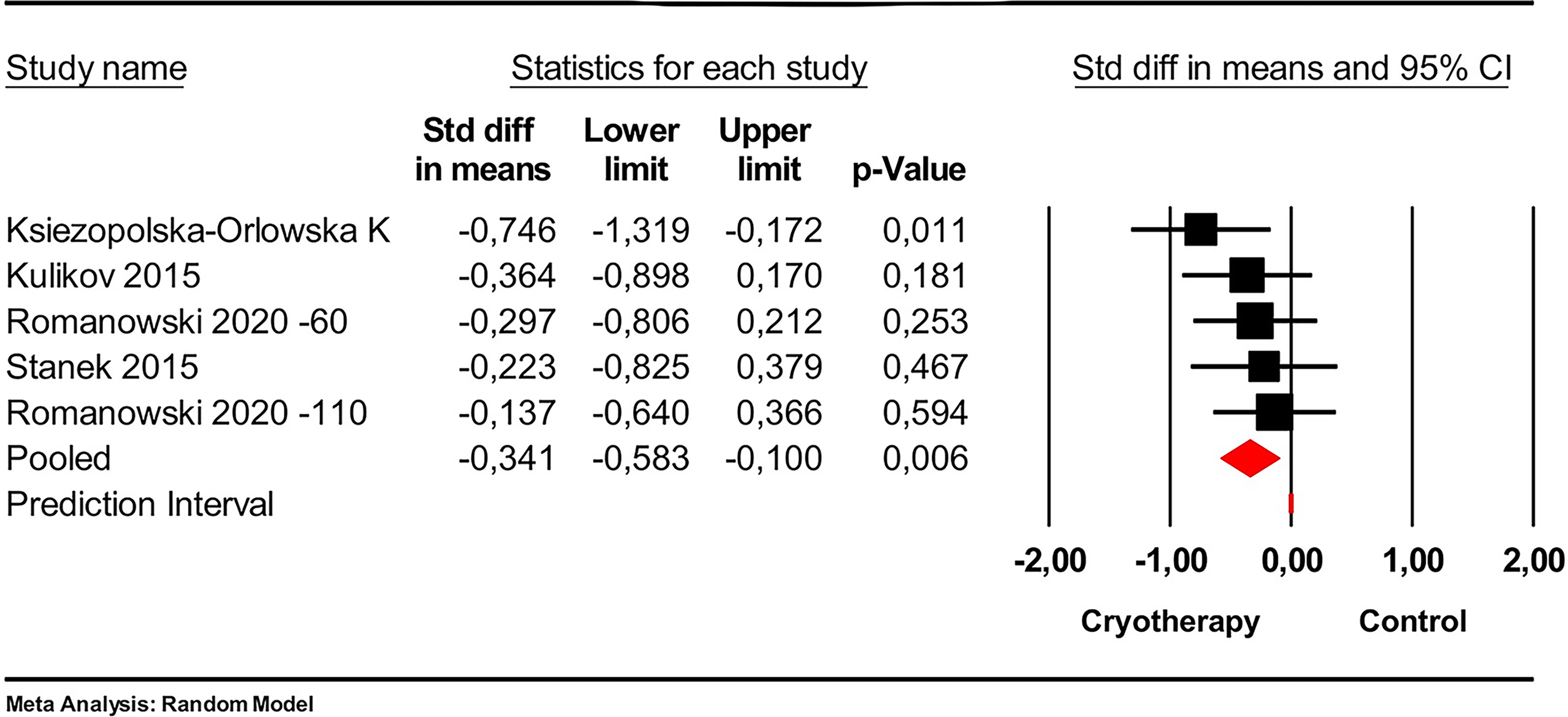
BASFI
The analysis was based on four studies (three studies with two subgroups).10,12–14 The mean effect size was −0.341 with a 95% confidence interval of −0.583 to −0.100 with p = 0.006 (Fig. 6). No heterogeneity was mentioned.
Discussion
This systematic review with meta-analysis showed the efficacy of WBC on pain, disease activity, and function in AS. This meta-analysis concluded that WBC significantly improved BASDAI (p < 0.001), ASDAS (p = 0.015), BASFI (p = 0.006), and pain VAS (p = 0.005) with no significant effect on CRP level (p = 0.684). No heterogeneity was reported.
AS is a chronic inflammatory rheumatic disease-causing pain and stiffness in the spine and eventually peripheral joints, potentially leading to irreversible deformation. Treatment of AS includes pharmacological treatment (NSAIDs, corticosteroids, DMARDs, and analgesics) along with various adjunct therapies. 21
Cryotherapy is a form of adjunct therapy defined by the application of superficial cold as a therapeutic agent. It has been recognized as a pain reliever for both acute and chronic pain. 22
Out of 53 potentially eligible studies, five studies were included in this systematic review. All studies evaluated WBC administered in a cryogenic chamber in patients with AS compared to control groups who only underwent regular physiotherapy programs. Owing to the lack of consensus on treatment duration and session frequency, duration of WBC sessions, intervention periods, and applied temperatures were variable. Pharmacological treatment was described in all the studies with no change of medication during the intervention, helping ensure that observed effects could be attributed to WBC. However, the type of DMARDs (biological or conventional) was not specified in the study of Lupa et al. 11 Patient groups differed in their pharmacological treatments. Thus, in the study of Stanek et al., all patients took only NSAIDs, while 72.7% took mainly NSAIDs without specifying DMARDs status in the study of Kulikov et al.13,14 In the RCT of Romanowski et al., 12 the intervention and control groups were not comparable with regard to bDMARDs and csDMARDs, as a higher number of patients undergoing WBC were on bDMARDs or csDMARDs compared to the control group. 12 Detailed description of patients in intervention and control groups was not provided in the studies of Orlowska et al. and Kulikov et al.10,14
By pooling patients from intervention groups, we found that WBC improved disease activity (BASDAI, ASDAS), pain intensity (VAS), and function (BASFI) with a significant effect size. However, it had no significant impact on CRP level.
Similar findings were demonstrated in the systematic review published in 2014, 17 which evaluated the efficacy of cryotherapy in inflammatory rheumatic diseases, including rheumatoid arthritis and patients with AS. This review showed that both local cryotherapy and WBC significantly improvemed pain VAS and disease activity assessed with the 28-joint Disease Activity Score (DAS28). 17 Also, a narrative review published in 2021 showed that both local and nonlocal cryotherapy applications were effective in reducing chronic pain, not only in rheumatic diseases, but also in degenerative origin (osteoarthritis, chronic low back pain, adhesive capsulitis, myofascial pain syndrome, and fibromyalgia). 23 From these results, we can conclude that WBC could positively impact the perception of pain and stiffness and overall patient-reported outcomes with no effect on inflammation markers according to the pooled analysis. Studies have shown that cryotherapy can alleviate pain, reduce inflammation, and improve joint function through different mechanisms. Initially, cryotherapy induces a rapid skin vasoconstriction followed by reflexive vasodilation, reducing blood flow in the inflamed area. It reduces VEGF expression, inhibiting angiogenesis and infiltration of inflammatory cells. Cold stimuli activate cold receptors, triggering the release of norepinephrine and acetylcholine that bind to macrophage receptors, inhibiting NF-κB activation, which reduces pro-inflammatory cytokines (Interleukin (IL)-1β, IL-6, IL-8, tumor necrosis factor-α) and intercellular adhesion molecules while promoting the production of the anti-inflammatory cytokine IL-10. In addition, cryotherapy reduces nerve excitability, alleviates muscle fatigue and stiffness, and lowers intra-articular temperature to inhibit collagenase activity. 24
While our study showed promising results of WBC as an adjunct therapy in patients with AS, it has a few limitations. The heterogeneity in terms of pharmacological treatment of pooled patients, along with higher frequency of bDMARDs intake in the intervention group of the study of Romanowski et al. 12 could act confounders. In addition, insufficient reporting and imbalance in background therapies (NSAIDs and DMARDs) across groups may have confounded the observed effects. The interventions were conducted over a short duration, and there was no long-term follow-up. Additionally, WBC did not significantly affect CRP levels. This suggests that its mechanism of action may be more related to neuromodulation or symptomatic relief rather than systemic anti-inflammatory effects. Reducing disease activity scores remains a critical objective in the treat-to-target strategy. Therefore, WBC serves as a valuable adjunct therapy to NSAIDs and DMARDs, but not a substitute, helping achieve the treatment target and optimize drug consumption.
The prediction interval reflects the dispersion in true effects. Since tau-squared is estimated as zero, we assume that all studies share a common effect size, and there is no dispersion of true effects. This analysis includes five studies. As a general rule, estimates of heterogeneity based on less than 10 studies are not likely to be reliable. In this context, Bayesian random-effects meta-analysis could offer a more robust alternative, stabilizing heterogeneity estimation and providing more realistic uncertainty intervals in small-sample situations. Although not applied here, such methods may improve precision in future syntheses. We also acknowledge that including multiple subgroup comparisons from the same studies may violate the assumption of independence, potentially biasing effect estimates. Moreover, the interpretation of Tau2 = 0 as evidence of homogeneity should be approached with caution in the context of a small number of studies, as this limits the power to detect true heterogeneity. The wide prediction intervals observed suggest that effect sizes may vary across different populations and clinical settings.
In conclusion, our systematic review and meta-analysis showed that WBC significantly improved pain, function, and disease activity in AS patients. As a nonpharmacological adjunct therapy, it showed promising results in the management of AS patients who are often young and productive. Further research is essential to validate these findings and investigate additional aspects of WBC, including its tolerance and the establishment of standardized treatment protocols. We strongly encourage future research to establish standardized WBC protocols regarding temperature, session duration, and frequency to enhance comparability and optimize clinical outcomes. Long-term follow-up studies are also needed to assess the durability of clinical benefits observed after short-term interventions.
Authors’ Contributions
O.S.: Conceptualization, data curation, writing—review and editing. S.B.: Conceptualization, data curation, writing— original draft. S.B.D.: Writing—original draft, writing—review and editing. L.R.: Investigation, data curation. I.M.: Supervision. R.T.: Supervision. A.B.T.: Visualization. C.D.: Methodology, software, formal analysis. L.A.: Validation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Compliance with Ethical Standards
This research involves human participants but as it is a retrospective analysis of published cases, it does not require informed consent. Ethics approval and consent to participate were not applicable in this review.
Data Availability
All data generated or analyzed during this study are included in this published article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.