
Abstract
Background:
Anxiety, depression, and sleep difficulties are mental health conditions (MHCs) that occur in up to 40% of young adults. Lifestyle practices, such as physical activity and quality diet, have been associated with better mental well-being; however, the use of lifestyle practices and the associations with MHCs among young adults are underexplored. Understanding these aspects may guide strategies to reduce the risk of MHCs via lifestyle choices.
Methods:
Data from the U.S. National Health Interview Survey, restricted to 3992 adults aged 18–30 years, were analyzed. Anxiety, depression, and sleep difficulties were assessed. Sixteen queried lifestyle practices were consolidated into the following: mind–body, body-based, physical activity, diet, substance use, and other. Prevalence estimates for MHCs and lifestyle practices were calculated. Logistic regression was used to assess the characteristics of young adults with each MHC, and the associations between lifestyle practices with each MHC.
Results:
Common characteristics of participants with anxiety, depression, or sleep difficulties were less likely to be male and more likely to be obese, using medications and health services, and reporting multiple chronic conditions. Across three groups of MHCs, mind–body practices were more frequently used than among their respective control populations. Across the MHC group, mind–body practices were significantly associated (adjusted odds ratio [aOR]A = 1.53; aORD = 1.78; aORS = 1.53). Unhealthy diet was positively associated with anxiety and sleep difficulties (aORA = 1.48, aORS = 1.34), and substance use was positively associated with anxiety (aORA = 1.81).
Conclusion:
Young adults with MHCs may face certain socioeconomic and health-related disadvantages. Strategies targeting these disadvantaged populations to reduce unhealthy diet consumption and substance use may improve MHCs.
Background
Anxiety, depression, and sleep difficulties are mental health conditions (MHCs) that are associated with increased frequencies of comorbidities, suicide, and reduced quality of life. 1 Studies reporting the prevalence of these three MHCs show increasing and higher rates among young-middle-aged adults. For example, a study of n = 155,026 U.S. residing adults aged 18–22 years reported that MHCs have risen from 22% in 2007 to 36% in 2017, 2 while a near 50% increase was reported from 2013 to 2021 among 350,000 college students. 3 During the COVID-19 pandemic, the global prevalence of anxiety, depression, and insomnia in young adults was reported as 28%, 35%, and 38%, respectively, 4 3%–10% higher than the global rates reported before the pandemic.5,6 Comparing age groups, data from the 2019 U.S. National Health Interview Survey (NHIS) showed that 18- to 30-year-old adults had a 3%–8% higher prevalence of depression (21%) and anxiety (20%) than adults aged 30 and older. 7 From the 2020 NHIS, prevalence of sleep difficulties (16%) was reported as higher (1%–3%) among 18- to 44-year-olds compared with older adults. 8 Prevalence of MHCs from the 2022 NHIS has not been reported; the 2022 NHIS dataset additionally provides an opportunity to assess a comprehensive list of potential determinants, many captured for the first time in the survey, of MHCs.
Sociodemographic and clinical determinants of MHCs among young adults are reported in several studies. A 2024 literature review reported that females, people who have experienced trauma, and ethnically minoritized groups had higher rates of MHCs. 9 Conversely, lowest MHCs and mental health service use were found among Asians compared with Caucasians in the U.S. population, 10 possibly due to systemic and cultural barriers, including stigma, misconception, language barriers, and lack of culturally appropriate services. 11 A second global review reported female, financial concerns, lack of social support, chronic health problems, and current mental illness as risk factors for anxiety and depression. 12 While these determinants inform potential structural and resource needs, a comprehensive assessment of lifestyle practices as determinants for MHCs may offer insights for self-modifiable care.
Lifestyle practices, including complementary and integrative health (CIH) approaches, physical activity, quality diet, and substance avoidance, have reported benefits for MHCs. For example, regular physical activity is associated with reduced anxiety, depression, and sleep difficulties.13,14 Benefits of quality diet on depression 15 and of CIH practices, such as meditation, yoga, and acupuncture, on risk reduction of MHCs have also been widely reported.16–20 Conversely, frequent consumption of processed food and sugar drinks is associated with increased risk of anxiety and depression, and reduced sleep quality,21–23 and heavy and long-term alcohol consumption and smoking are associated with higher sleep difficulties but not depression.12,24,25
These aforementioned studies have focused on the general population of young adults. There is relative paucity of work assessing the sociodemographic, clinical, and lifestyle characteristics of young adults with anxiety, depression, or sleep difficulties, and less so on the role and frequency of use of lifestyle practices in this population. This knowledge may provide insight into potential interventions for mental health management in target populations.
Methods
Data source
Free and publicly available (https://www.cdc.gov/nchs/nhis/documentation/2022-nhis.html) secondary data from the 2022 NHIS 26 were extracted for analysis. The NHIS is an annual cross-sectional study of the noninstitutionalized U.S. population, using multistage probability sampling to achieve a national representative sample, approved by the Research Ethics Review Board of the National Center for Health Statistics. Data on sociodemographics, health care access and use, health status, health-related behaviors, lifestyle practices, and MHCs were queried. Data from sample adult interviews and imputed income files were used, restricted to adults aged 18–30 years, n = 3992 (unweighted), representing an estimated 55,342,855 (22%) of the U.S. population in this age group. Recommended by the NHIS handbook, all analyses include sampling weights, strata, and primary sampling units; applied in this study.
Sociodemographic and clinical variables
Age, sex, ethnicity (White, Black/African American, Asian, American Indian and Alaska Native, other single, and multiple races), highest level of education (never attended, grades 1–11, 12th grade, General Educational Development or equivalent, high school graduate, some college, associate degree, bachelor’s degree, master’s degree, doctoral degree), marital status (married, living with a partner together as an unmarried couple, neither), employment (last week, did you work for pay at a job of business?), and socioeconomic status (derived from ratio of family income to federal poverty level) 27 were recoded and recategorized (Table 2).
Body mass index (BMI) was calculated by weight (kg) divided by height (m) squared and was categorized based on the World Health Organization definitions 28 ; comorbidities were reported as a total number: 0, 1, and >1 from a list of 12 chronic conditions. 29 Other clinical variables analyzed in this study (dichotomized as No/Yes) were health insurance; counseling/therapy (received in the past 12 months); prescription medications used for anxiety/worry/nervousness, depression, and/or sleep difficulties (helping fall asleep or stay asleep)—consolidated as No/Yes for any of three MHCs; and prescription medications used in the past 12 months for other mental health reasons (emotions/concentration/behavior/mental health).
Mental health conditions
MHC criteria were defined as per guidelines, where available, and each was coded as binary (No/Yes) for analyses.
Lifestyle practices
Sixteen lifestyle practices were queried within the NHIS. CIH practices (nine practices, including meditation, yoga, and acupuncture) were queried as “having used” in the past 12 months. Physical activity was queried by “How often do you do physical activities” with further questions regarding type, frequency, and duration; for analysis, defined as minimum physical activity based on the 2018 guidelines 32 and consolidated with walking (for fun, relaxation, exercise, or to walk the dog). Diet was queried as a selection of five beverages and nine food items by frequency of consumption (never to daily) in the past month; daily consumption of all listed processed foods and sugar drinks was consolidated as “unhealthy diet.” Coffee or tea, green leafy, other kinds of potatoes, vegetables, and salsa were excluded from analysis given their low representation of a quality diet. Smoking status was queried as current, former, or never; current was used for analysis. Alcohol drinking status was queried by 10 options ranging from lifetime abstainer to current heavier, and moderate/heavy was used for analysis. Lifestyle practices were further consolidated into six categories (Table 1) based on having similar features and then dichotomized for analysis.
Categorization of National Health Interview Survey Lifestyle Practices
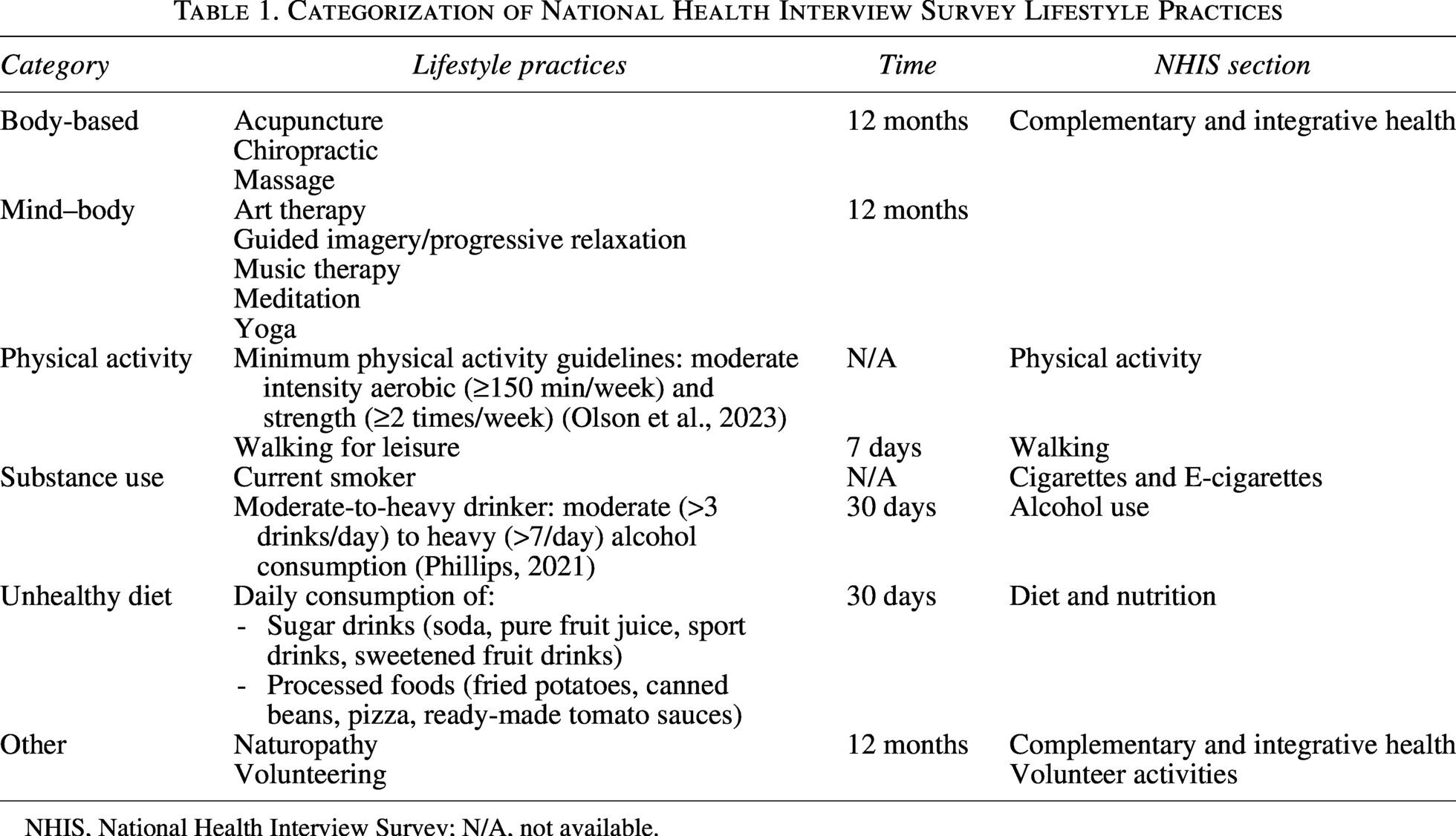
NHIS, National Health Interview Survey; N/A, not available.
Statistical analysis
All analyses were conducted on complete cases using Stata/SE 17.0 version. 33 Responses of “refused,” “not ascertained,” and “don’t know” were coded as missing.
Prevalence estimates of lifestyle practices among participants with and without MHCs (Fig. 1) were derived using svy in Stata and included sampling weights, strata, and primary sampling provided by the NHIS. Peason chi-squared test was then applied to assess statistical differences between groups.
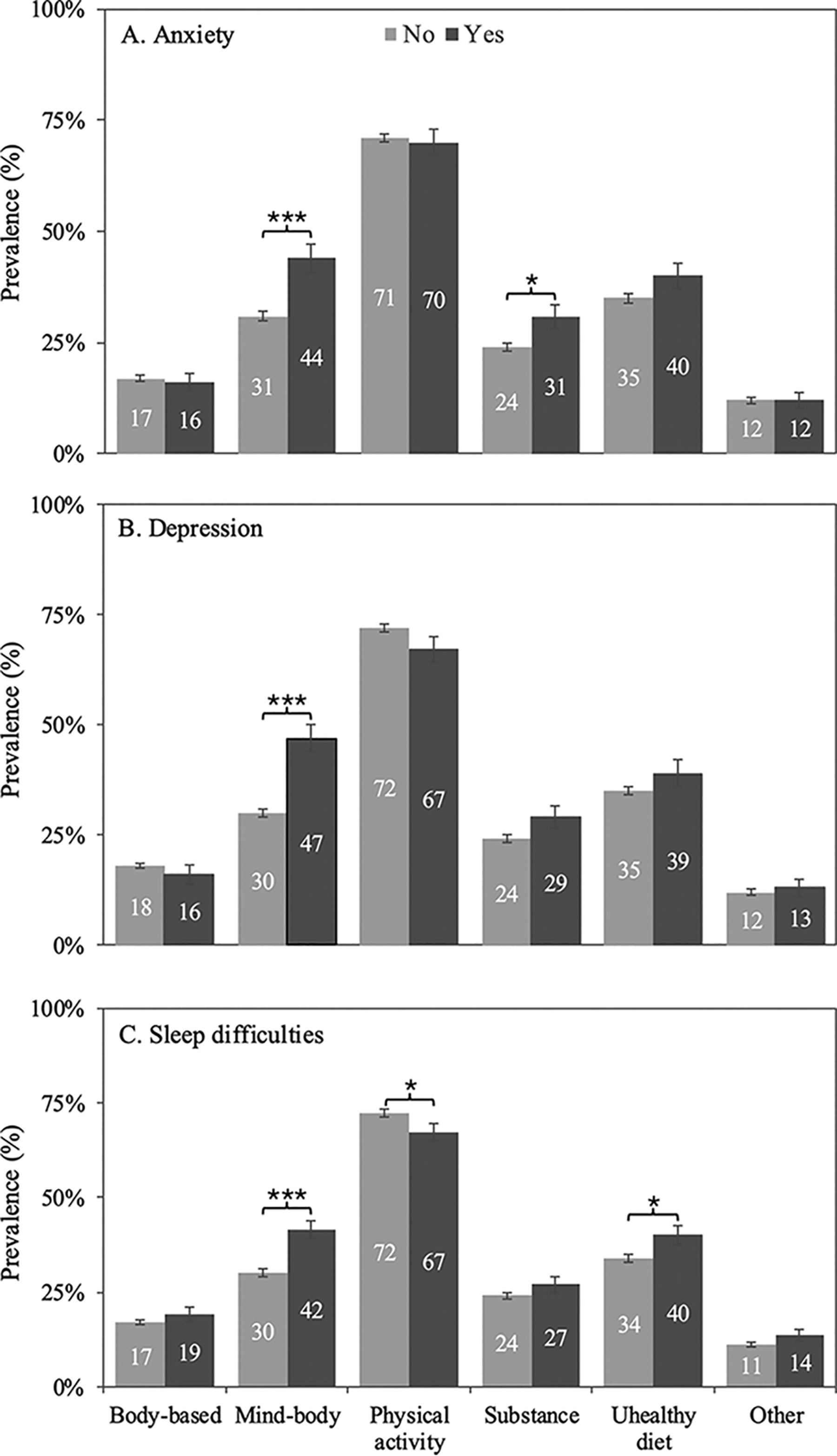
Weighted population estimated prevalence ± standard error of the mean of lifestyle practices (x-axis) used among young adults without (No) and with (Yes):
Logistic regression, adapted to the NHIS complex sample design, was used to assess associations of sociodemographic and clinical characteristics with each MHC (Table 2), adjusted for age, sex, and education to minimize overadjustment. The comparator group was specific to each MHC: young adults with anxiety were compared with young adults without anxiety, those with depression compared with those without depression; those with sleep difficulties with those without sleep difficulties.
Sociodemographic and Clinical Characteristics of Young Adults with Mental Health Conditions
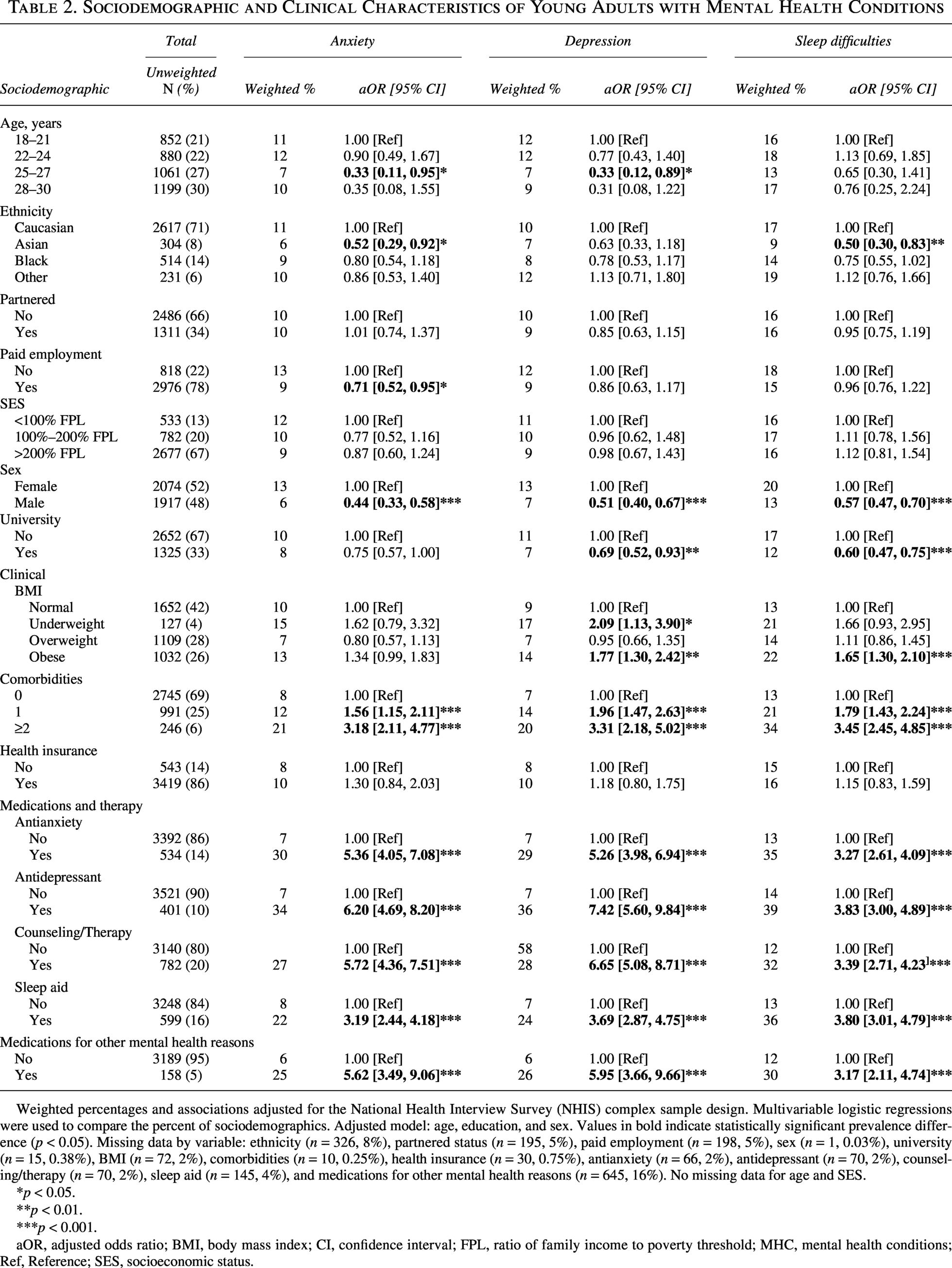
Weighted percentages and associations adjusted for the National Health Interview Survey (NHIS) complex sample design. Multivariable logistic regressions were used to compare the percent of sociodemographics. Adjusted model: age, education, and sex. Values in bold indicate statistically significant prevalence difference (p < 0.05). Missing data by variable: ethnicity (n = 326, 8%), partnered status (n = 195, 5%), paid employment (n = 198, 5%), sex (n = 1, 0.03%), university (n = 15, 0.38%), BMI (n = 72, 2%), comorbidities (n = 10, 0.25%), health insurance (n = 30, 0.75%), antianxiety (n = 66, 2%), antidepressant (n = 70, 2%), counseling/therapy (n = 70, 2%), sleep aid (n = 145, 4%), and medications for other mental health reasons (n = 645, 16%). No missing data for age and SES.
p < 0.05.
p < 0.01.
p < 0.001.
aOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; FPL, ratio of family income to poverty threshold; MHC, mental health conditions; Ref, Reference; SES, socioeconomic status.
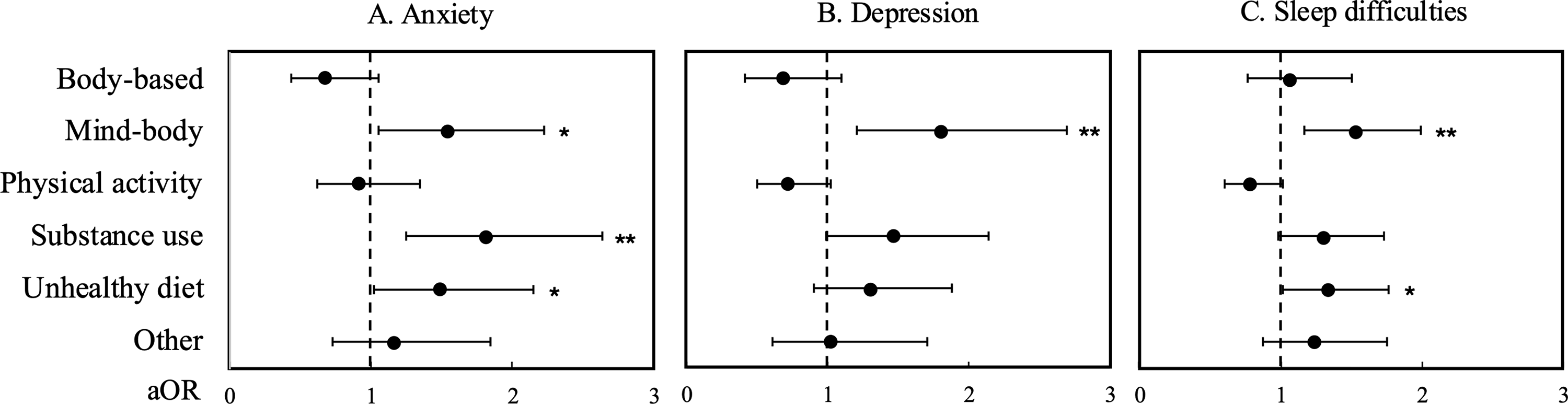
Associations between lifestyle practices and each of three MHCs (Table 3 and Fig. 2) were assessed by multivariable logistic regression, adapted to the NHIS complex sample design, adjusted for prescribed medications for anxiety, depression, or sleep difficulties (as appropriate to the outcome measure), as well as prescription medications for other mental health reasons, number of comorbidities, employment status, education, and sex. Covariate adjustments were based on previous literature 12 and reached significance with stepwise analysis. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) are presented, with significance set at p < 0.05.
Associations Between Lifestyle Practices and Mental Health Conditions
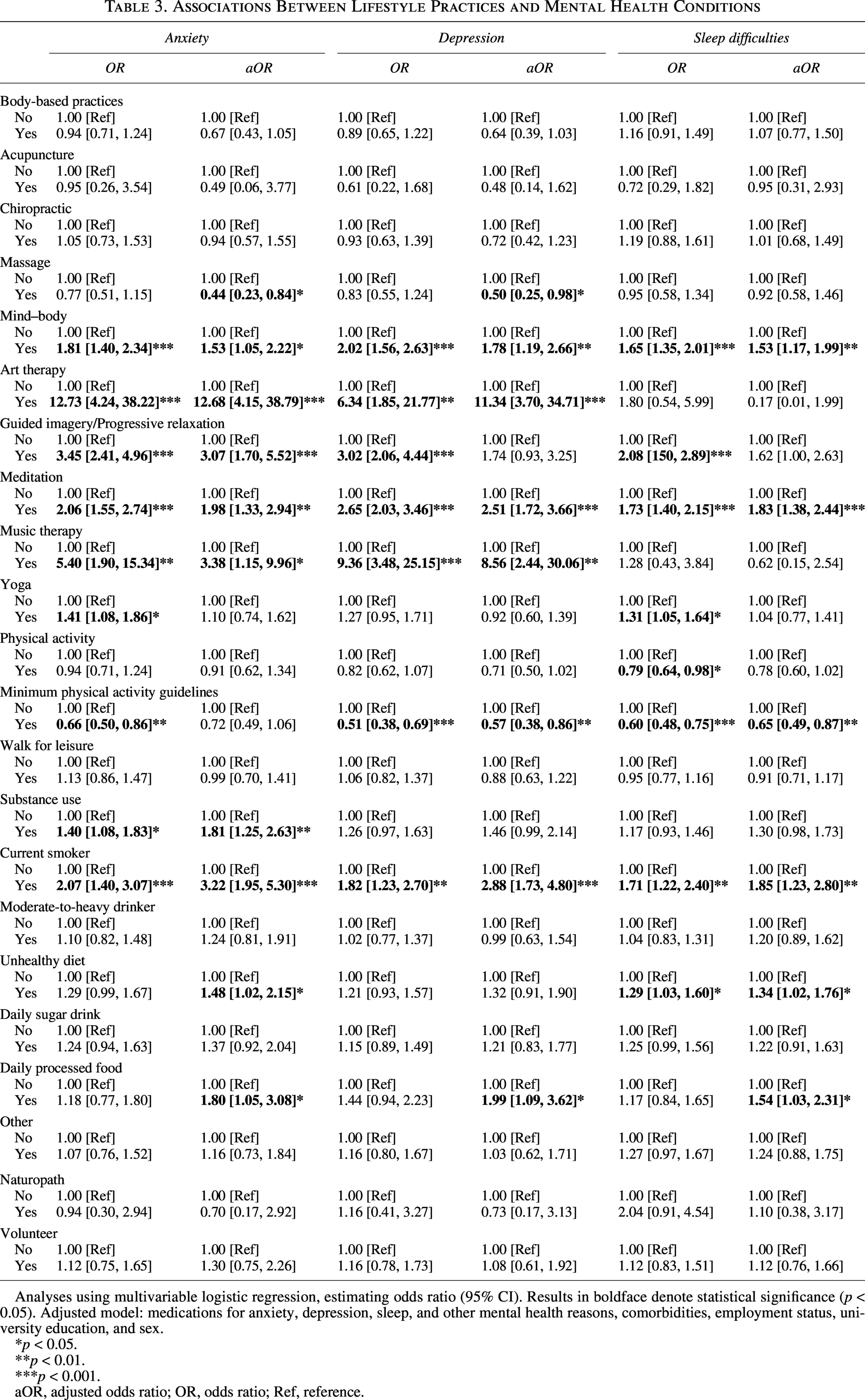
Analyses using multivariable logistic regression, estimating odds ratio (95% CI). Results in boldface denote statistical significance (p < 0.05). Adjusted model: medications for anxiety, depression, sleep, and other mental health reasons, comorbidities, employment status, university education, and sex.
p < 0.05.
p < 0.01.
p < 0.001.
aOR, adjusted odds ratio; OR, odds ratio; Ref, reference.
Associations between lifestyle practices and
Results
Population characteristics
Characteristics of young adults with one of the three MHCs, compared with their respective comparison group without the MHCs, were assessed to determine commonalities and differences in potential sociodemographic, clinical, and lifestyle predictors of having MHCs. Results showed that common characteristics across young adults with one of the three MHCs were less likelihood of being male and more likely to be obese, reporting ≥1 comorbidities, taking medications for MHCs, and utilizing counseling/therapy (Table 2). Determinants of specific MHCs included the following: young adults with anxiety were less likely to be in paid employment or to be of Asian ethnicity; young adults with depression were less likely to be university educated; and young adults with sleep difficulties were less likely to be of Asian ethnicity or university educated.
Prevalence estimates identified the frequency of MHCs and lifestyle practices among young adults. Results (data not shown) revealed that 10% of young adults reported depression, 10% reported anxiety, and 16% reported sleep difficulties in the study population. Regarding lifestyle practices, 71% of young adults engaged in regular physical activity, 32% in mind–body practices, 35% had an unhealthy diet, and 25% reported substance use. Body-based practices (17%) and other (12%) lifestyle practices were least frequently used. Missing data for MHCs and lifestyle practices were <5%.
Chi-squared analyses revealed differences in engagement with lifestyle practices between young adults with and without MHCs. Compared with the respective MHC control group, mind–body practices were significantly higher in young adults with anxiety (44% vs. 31%; Fig. 1A), depression (47% vs. 30%; Fig. 1B), and sleep difficulties (42% vs. 30%; Fig. 1C). Unhealthy diet was higher in young adults with anxiety (40% vs. 35%) and sleep difficulties (40% vs. 34%), and substance use was higher in young adults with anxiety (31% vs. 24%). Physical activity was lower in young adults with sleep difficulties (67% vs. 72%), and body-based practices were lower in those with anxiety (16% vs. 17%) and depression (16% vs. 18%).
Associations between lifestyle practice use and MHCs
Regression analyses identified associations between lifestyle practices (Table 3 and Fig. 2) with each of the three MHCs. For an overall perspective of lifestyle practices, six broad lifestyle categories were analyzed. This followed an analysis of individual practices within these categories for detail. All results are reported in Table 3, and for clarity, only associations reaching significance upon adjustment are reported in the text.
Results revealed that compared with young adults without anxiety, those with anxiety were more likely to engage with three of six lifestyle categories defined in Table 1: mind–body practices (aOR = 1.53), unhealthy diet (aOR = 1.48), and substance use (aOR = 1.81). To identify whether specific practices were associated, further analysis of practices within broad lifestyle categories was undertaken. This revealed that young adults with anxiety, compared with those without anxiety, were more likely to practice meditation (aOR = 1.98), guided imagery/progressive relaxation (aOR = 3.07), art therapy (aOR = 12.68), and music therapy (aOR = 3.38). They were also more likely to consume processed food daily (aOR = 1.80) and be a current smoker (aOR = 3.22). Another association was less likelihood of use of massage (aOR = 0.44) within the category of body-based practices.
Compared with young adults without depression, those with depression were more likely to use mind–body practices (aOR = 1.78), specifically meditation (aOR = 2.51), art (aOR = 11.34), and music therapy (aOR = 8.56). They were also more likely to consume processed food (aOR = 1.99) and be a current smoker (aOR = 2.88), and less likely to meet the physical activity guideline (aOR = 0.57) or use massage (aOR = 0.50).
Compared with young adults without sleep difficulties, those with sleep difficulties were more likely to use mind–body practices (aOR = 1.53), specifically meditation (aOR = 1.83), and consume an unhealthy diet (aOR = 1.34), specifically processed food daily (aOR = 1.54). They were also more likely to be a current smoker (aOR = 1.85) and less likely to meet the physical activity guideline (aOR = 0.65).
Discussion
The prevalence of anxiety, depression, and sleep difficulties in young adults is reportedly up to 40%. 4 Assessing the young adult fraction (18–30 years old) of participants in the 2022 NHIS using patient-reported screening measures, the authors show that 10% of participants had anxiety, 10% had depression risk, and 16% had sleep difficulties. Little is known of the use of lifestyle practices, predictors of these MHCs, or the association between lifestyle and MHCs in this population. The authors found that for each of the three MHCs, gender, BMI, comorbidities, medication, and service use were consistently associated. Of the lifestyle practice categories assessed, mind–body practices were consistently positively associated with MHCs, of which regular physical activity was most frequently used.
The cross-sectional study design here precludes causal inferences as to lifestyle–MHC causal directionality. However, it is important to highlight that the associations seen here between lifestyle practices, as well as other clinical and demographic characteristics, and MHCs are potentially impactful in either counterfactual scenario. If factors like unhealthy lifestyle practices or low socioeconomic status or other potentially negative/deleterious characteristics are more common among young adults with MHCs, then surveillance and increased outreach targeting these factors may be needed. On the contrary, if lifestyle practices or other clinical and demographic characteristics are associated with MHCs, these may represent valuable intervention targets. There is plausibility for either of these pathways to be in action, and more likely that bidirectional relationships exist, as well as potential feedback loops. Exploration of these dynamics in prospective cohort studies with comprehensive longitudinal measures of these potential risk factors and outcomes is needed.
The authors estimated a prevalence of 10%–16% for MHCs among 18- to 30-year-old adults in a national U.S. population in 2022; lower than global rates reported as 31%–38% in adults and university students during the COVID-19 pandemic. 4 Differences potentially attributed to the global study including multiple measures for MHCs as well as inclusion of mild MHCs in their criteria compared with the use of a single tool and moderate/severe criteria. Nevertheless, these results show a moderate increase in MHC frequencies compared with those reported from the 2019 NHIS: 6% versus 10% for anxiety, 7% versus 10% for depression, and 15% versus 16% for sleep difficulties.7,8
Sociodemographic and clinical predictors of MHCs
Consistent with previous studies,12,34 the authors found sex, employment, and education to be associated with MHCs. Females were more likely to have MHCs, which others have proposed to be attributed to biological and psychosocial factors, such as sex hormones and social roles. 35 Young adults in paid employment are less likely to have MHCs, in alignment with studies reporting that financial stress is associated with worsening mental health. 12 However, given the cross-sectional design of both the current and past studies, the directionality of effect is unclear; it may be that financial stress from unemployment may contribute to poor mental health and/or poor mental health impacts the ability to find and maintain employment. Young adults with a university degree were less likely to have depression or sleep difficulties, possibly due to higher educated persons having better employment opportunities, financial stability, awareness and capacity to seek support, and higher self-mastery, each of these factors being contributors to better mental health. 9 Asian young adults had lower frequencies of MHCs compared with Caucasians, in alignment with a 2023 study of n = 13,642 respondents in the U.S. reporting that Asian Americans were less likely to report MHCs and use mental health services compared with other ethnicities. 10 This may reflect sampling bias, or mental health awareness and mental health being culturally stigmatized in Asian communities, highlighting consideration of culturally tailored mental health services.
BMI has been associated with higher MHCs, with a bidirectional relationship.36,37 In corroboration, the authors showed that underweight and obese BMI was associated with increased frequencies of depression, and obesity with increased frequencies of sleep difficulties. They also found a pattern of increasing odds between multicomorbidities and MHCs. Chronic conditions and medications are commonly associated with adverse effects on mental well-being, including an increased sense of vulnerability to other adverse events. 38 Relatedly, in this study population, suggesting more frequent use, mental health services, prescribed MHC medications, and counseling/therapy were positively associated with MHCs. While it is necessary to substantiate these findings in prospective cohort studies, these results align with the literature and suggest the potential for these factors to be considered among people with MHCs.10,12,39
Broad category lifestyle practices among young adults with MHCs and associations with MHCs
Lifestyle practices of mind–body, unhealthy diet, and substance use were more frequently used, and physical activity were less frequently, among young adults with one of the MHCs compared with those without MHCs (Fig. 1). Prior studies have similarly reported that unhealthy diet, smoking and alcohol consumption, and physical inactivity are prevalent in people with MHCs, 40 especially for anxiety and depression, possibly serving as maladaptive coping mechanisms, while also acting as contributing factors that increase the risk of developing these conditions. 41
Few studies reported on mind–body practice use. A study of 3286 18–24-year-old adults with mental distress reported that 15% used mind–body practices, including meditation, guided imagery, or progressive relaxation. In this study population, use of these practices was in 32% of the population. The use of both adaptive (mind–body practices) and maladaptive practices (unhealthy diet, substance use, and physical inactivity) in young adults with MHCs suggests that interventions for MHC management need to consider characteristic predictors of these practices in assessing which may be most effective.
Regarding associations, mind–body, substance use, and unhealthy diet were positively associated with MHCs, compared with those without specific MHCs. Similarly, reviews including 42 and 49 studies (n = 2974 and n = 4506, respectively) have shown that mind–body practices improve anxiety, depression, and sleep quality in the general population,42,43 while other reviews of 15 studies and 29 studies, respectively, have shown that substance use (smoking and illicit drugs) and unhealthy diet (processed foods and sugar drinks) were negatively associated with all three MHCs in the general population.25,44,45 These subcategory analyses revealed further insights, however, due to low sample sizes, interpretation is limited.
Specific lifestyle practices among young adults with MHCs and associations of practices with MHCs
Of the three subcategories in the body-based practices, only massage was inversely associated with anxiety. Massage therapy has been positively associated with anxiety and depression, but due to low-quality studies and variations in massage intervention, recommendations remain inconclusive.18,46 Systematic reviews have reported acupuncture to be positively associated with reduced depression and sleep difficulties.20,47 The authors did not find such associations, possibly due to fewer than 2% (n = 54, data not shown) of this population using acupuncture, and limited capture of frequency and number of times used in the 12-month period queried.
Physical activity categories comprised aerobic/strength activity and waking for leisure; only the former was inversely associated with MHCs. The general consensus in the literature is that a combination of aerobic (≥150 min/week) and strength (≥2 times/week) training is required for observed benefits on MHCs. 32 Multiple studies have shown that regular physical activity improves sleep quality and high-intensity physical activity reduces anxiety and depression.13,14 While these data showed no association between walking and MHCs, others have reported benefits; for example, a review, including seven studies, showed that walking in nature reduced depression and anxiety. 48
Mind–body subcategories were positively associated with MHCs, with the highest effect observed with meditation. Meditation practice for reducing anxiety and depression, and for improving sleep is widely reported, with interventions ranging between 4 and 8 weeks.16,17 However, detrimental effects were reported in a review of 83 studies, of which 33% of studies with a total population size of n = 4023 reported higher anxiety, depression, and cognitive anomalies in adults who practice meditation. The authors suggest adverse effects possibly due to inappropriate form of meditation and/or practice not carried out properly. 49 These highlight that ongoing support and monitoring of health are required upon prescribing lifestyle modifications.
A few small studies have reported the benefits of 12-week yoga practice on sleep and distress, 10–20 minutes of guided imagery/progressive relaxation on anxiety and stress, and 3-week art/music therapy on anxiety and depression.19,50,51 In this study population, guided imagery and art/music therapy were positively associated with anxiety, and art/music therapy was positively associated with depression, but yoga was not associated with any of the MHCs. Duration, frequency, and modality of practices may contribute to differences in these and prior studies.
Of unhealthy and other lifestyle practices, only current smoker and daily consumption of processed food were positively associated with MHCs. Some prior cross-sectional studies have reported positive associations between both smoking and consumption of ultraprocessed food and sugar drinks with anxiety and depression,25,44 while others have reported no associations between smoking and depression. 12 Bidirectional associations between alcohol and MHCs have also been reported: excessive alcohol intake increases the risk of MHCs, and conversely, individuals with existing MHCs may consume alcohol as a coping strategy.24,52 Practices of naturopathy and volunteering reduce anxiety and depression.53,54 In this study population, duration and frequency of practice, as well as small sample size, may contribute to the lack of associations observed for these practices. Together, these findings highlight the importance of continued promotion of a high-quality diet as well as smoking cessation for mental health management, and the complexity in measuring lifestyle practices.
Strengths and limitations
This study strengths include the use of data from a large nationally representative sample, facilitating greater representation and generalizability. Second, to the best of our knowledge, this is one of the few studies investigating predictors of MHCs and frequency of use of a comprehensive list of lifestyle practices and their associations with MHCs.
The primary limitation of this study is its cross-sectional study design. As noted previously, the absence of follow-up measures within the NHIS precludes longitudinal assessments. Other limitations include use of self-reported measures, nonvalidated tools, absence of frequency and duration data on lifestyle practices, no clinical assessment or linkage to medical records for MHCs, and use of nonethnicity-specific BMI classification for this multiethnic study population. These represent areas to explore in future studies. Finally, the authors did not assess the co-occurrence of the three MHCs and interactions between MHCs; all three co-occur in 20%–60% of cases. 55
Conclusions
Young adults with MHCs had specific sociodemographic and clinical characteristics informing potential subpopulations at higher risk of MHCs. Frequency of use of lifestyle practices in this population and the associations between lifestyle practices and MHCs, especially for mind–body practices, unhealthy diet, and substance use, highlight potential targets for MHC management and health promotion.
Authors’ Contributions
X.Y.: Conceptualization, investigation, methodology, data curation, formal analysis, original draft preparation, writing—review and editing, and funding acquisition. S.S.-Y.: Methodology and writing—review and editing. N.N.: Conceptualization, investigation, methodology, visualization, original draft preparation, writing—review and editing, funding acquisition, supervision, and project administration.
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
China Scholarship Council–University of Melbourne PhD Scholarship awarded to X.Y. (under the supervision of N.N.). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the article; or in the decision to publish the results.
Institutional Review Board Statement
The NHIS is approved by the Research Ethics Review Board of the National Center for Health Statistics and the U.S. Office of Management and Budget.
Informed Consent Statement
Participants were provided with a participant information statement, and all provided informed consent.
Data Availability Statement
Data are publicly available from the National Center for Health Statistics of the Centers for Disease Control and Prevention. Consolidated data for the current study are available by request to N.N.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.