
Abstract
Introduction:
Chronic pain is a major public health problem. Due to the persistent, costly, and complex nature of chronic pain, there is a need for new safe and effective treatments. Integrative breathwork interventions, or therapeutic styles of conscious breathing, have promise as novel treatments for chronic pain. The primary objective of this proof-of-concept study was to examine the feasibility, acceptability, and clinical significance of an integrative breathwork intervention for adults with chronic pain.
Methods:
Participants with chronic pain and without prior breathwork experience were eligible for this study. Participants completed online surveys at baseline, 2-week, and 6-week follow-ups as well as a brief survey immediately before and after the single group breathwork session. Guided Respiration Mindfulness Therapy (GRMT) was the integrative breathwork intervention that involved 1 hour of conscious connected breathing while engaging in somatically focused mindfulness and relaxation.
Results:
A total of 11 participants were enrolled into this study, and 10 completed the breathwork session. The intervention was rated as highly acceptable (M = 9.3, standard deviation [SD] = 1.9) and satisfying (M = 9.7, SD = 0.5). All participants recommended the intervention to someone else suffering from chronic pain. There were large, clinically meaningful improvements in pain intensity and pain interference from baseline to the 2-week (mean difference [MD] = −2.9) and 6-week (MD = −3.5) follow-ups.
Conclusion:
A single group session of GRMT was shown to be highly acceptable, satisfying, and potentially helpful to individuals with chronic pain. The findings demonstrated proof of concept, with most participants reporting a clinically meaningful improvement in pain outcomes through the follow-ups. Additional research on integrative breathwork interventions for chronic pain is warranted.
Introduction
Chronic pain is a major public health problem. It impacts >100 million people worldwide and continues to rise in prevalence and disease burden. 1 Chronic pain is a complex condition that is influenced by multiple interacting biological, psychological, and social factors. 2 This biopsychosocial model of chronic pain emphasizes the importance of integrative treatments to help restore function and improve quality of life for the whole person, rather than solely targeting pain relief. 3 While many treatment options are available for chronic pain, they tend to have modest efficacy along with high costs and risks. 4 Nonpharmacological interventions are recommended as first-line treatments for chronic pain and are growing in interest as standalone or complementary options to manage pain-related symptoms.5,6 Developing and testing nonpharmacological interventions rooted in the biopsychosocial model comprise a critical step to addressing the need for safe, effective, and accessible chronic pain treatments.
Breathwork is a promising mind–body approach for chronic pain and whole-person health. Breathwork is an umbrella term to describe the conscious control of breathing that is often used for therapeutic benefits. 7 There are a variety of styles, ranging from breathing self-management practices that individuals can engage in on their own to more intensive, facilitator-guided integrative breathwork interventions. Importantly, there is a bidirectional relationship between respiration and pain,8–10 stress,10,11 and emotions,12,13 which suggests that individuals can modify their breathing to influence biopsychosocial factors. Much of the research examining breathwork and chronic pain focuses on breathing self-management practices. 14 These include breathing techniques (e.g., slow deep breathing) or respiratory devices that are typically used daily for approximately 4–12 weeks. Preliminary evidence from various chronic pain populations shows small improvements in pain outcomes and small-to-large improvements in pain-related factors, including sleep, stress, and anxiety.15,16 A major advantage of these breathing practices is that they are accessible, scalable, and can empower individuals to self-manage their symptoms in daily life, such as during particularly stressful or painful situations.17,18 However, the lack of large, clinically meaningful improvements in chronic pain provides rationale to examine more potent forms of breathwork.
Integrative breathwork interventions incorporate conscious breathing along with other components or modalities. This style of breathwork is engaged in a 1-on-1 or group setting with a trained facilitator, who guides and supports the therapeutic process. There are many different names for approaches based on this style of breathwork (e.g., Transformational Breathwork, Therapeutic Breathwork, Holotropic Breathwork, Vivation) that are mainly differentiated by their theoretical framework and the combination of intervention components (e.g., bodywork, music). The defining commonality across integrative breathwork interventions is a conscious connected breathing pattern where there is no pause between inhale and exhale that is sustained for 45 min to 3 h. This conscious connected breathing technique can alter consciousness and elicit a wide variety of physical, emotional, cognitive, and spiritual experiences.7,19–23 These types of breathwork experiences are thought to be therapeutic or transformative for both clinical and healthy populations21,24–27 but have never been studied specifically for chronic pain. Case studies and retrospective reports have suggested that intensive styles of breathwork are safe for most people and potentially helpful for alcohol and drug addictions.28,29 A more recent study of individuals with mental health disorders found that a single integrative breathwork session can improve mindfulness, stress, and satisfaction with life for up to 4 weeks. 22 Of 58 participants in that study, 97% reported somatic effects, such as strong physical tension with eventual muscle release and relaxation. Although there is increasing public and scientific interest in integrative breathwork interventions,7,30 there is a need for more high-quality studies in this new area of investigation.
Guided Respiration Mindfulness Therapy (GRMT) is a manualized integrative breathwork intervention that is designed for clinical practice and rigorous research. 31 GRMT includes three core components: respiratory regulation (i.e., conscious connected breathing), somatically focused mindfulness, and relaxation of physical tension. These components are the focus of every 60-min breathwork session. Initial controlled and uncontrolled trials have shown that multiple sessions of GRMT may improve anxiety, depression, stress, and mindfulness.31–33 While its potential as a treatment for chronic pain remains untested, there is theoretical rationale to expect the additive or synergistic effects of the intervention components for pain. For example, increasing research suggests that mindful body awareness and interoceptive exposure with acceptance—techniques embedded in GRMT—may help with pain reappraisal and emotion regulation.34–36 Moreover, the conscious connected breathing pattern has been suggested to promote the extinction of avoidance behaviors, 25 which could include resistance to feeling sensations in the body (e.g., pain) or fear of movement—avoidance tendencies that contribute to the maintenance of chronic pain.37,38 Other potential mechanisms of GRMT that could plausibly reduce chronic pain include improved autonomic balance, 39 normalized brain activity,19,40–43 reduced allostatic load,44,45 increased interoceptive awareness,46,47 and deep states of rest and relaxation.48,49
The primary aim of this proof-of-concept trial was to examine the acceptability of GRMT among adults with chronic pain and evaluate whether a single GRMT session leads to clinically meaningful changes in pain intensity and interference. These aims align with the early phases of behavioral intervention development frameworks, where the goal is to test whether a new intervention can produce clinically significant, rather than statistically significant, improvements in outcomes.50–52 Single-session interventions can be beneficial for pain and pain-related outcomes53–60 and have some advantages over longer interventions. 61 Because group breathwork sessions are widely offered in real-world settings (e.g., workshops), this design also represents a scalable, ecologically valid treatment format to test. To demonstrate the plausibility of clinically meaningful improvement, we hypothesized that participants would report a minimal clinically important difference in pain intensity and interference from baseline to the 2-week follow-up.62,63 We also hypothesized high treatment acceptability with ≥80% mean ratings on overall acceptability and satisfaction. Evaluating whether the study is feasible and the intervention achieves these benchmarks of acceptability and clinical meaningfulness will inform a go/no-go decision to progress to additional pilot feasibility testing in anticipation of scaling up to a larger, fully-powered trial.52,64
Methods
Trial design
This single-site, single-arm, proof-of-concept trial was designed to evaluate the feasibility, acceptability, and clinical utility of a group breathwork session for adults with chronic pain. Participants completed online surveys at baseline, 2-week, and 6-week follow-ups as well as a paper-and-pencil survey before and after the breathwork session. This study was approved by the Florida State University Institutional Review Board and registered on ClinicalTrials.gov (Identifier = NCT06455839). All participants provided written and signed informed consent prior to engaging in the study procedures.
Participants
Participants were recruited from Tallahassee, FL, USA, through a combination of local outreach and online advertising. Adults were eligible to participate if they were 18 years of age or older, had received a formal chronic pain diagnosis, and agreed not to begin any new treatment during the study. Individuals were excluded if they had any prior training in breathwork. Participants were compensated for completing the study procedures.
Intervention
The integrative breathwork intervention, GRMT, includes three core components. The first component is respiratory regulation. This involves a conscious connected breathing pattern into the upper chest, with no pause between inhalation and exhalation. Breathing is in and out through the nose or mouth, with a deep, active inhale followed by a passive, relaxed exhale. The second component is somatically focused mindfulness, where the instruction is to focus on the most dominant sensation from moment-to-moment with an orientation of acceptance. Another aspect of mindfulness involves staying present with the breathing pattern while letting go of any thoughts that arise. The last component is relaxation, with suggestions to relax and release any areas of tension in the body. All participants engaged in a 60-min GRMT breathwork session.
This single-session intervention lasted for 2 h in group sizes of 2–4 individuals. Participants completed a preintervention survey and introduced themselves to the group with their name and a brief description of their chronic pain. The facilitator (L.L.) introduced GRMT and described the experiences that participants might have during the session, including possible transient discomfort. This included the potential challenge of maintaining the breathing pattern, as well as the possibility of feeling intense emotions or physical sensations (e.g., tetany). Participants remained supine for the 60-min GRMT breathwork session with their eyes closed. If a participant repeatedly drifted from the breathing technique, they were asked to sit up for a few minutes to maintain the breathing pattern. During the last 5 min, participants were instructed to let go of the conscious connected breathing technique and allow their breath to return to its natural rhythm while they relaxed. After the breathwork session, participants shared their experience with the group. The facilitator responded by normalizing participants’ experiences without providing additional intervention or therapeutic strategies. Participants were not assigned any homework or continued practice after the session.
Measures
Sample characteristics
The baseline survey assessed participants’ sociodemographics, including, age, sex, gender, race, ethnicity, marital status, education level, employment, and household income.
Feasibility
The recruitment rates included the number of eligible participants enrolled during the 1-week recruitment period. Intervention adherence was determined by calculating the number of enrolled participants who completed the 2-h intervention session.
Treatment acceptability
Treatment acceptability was assessed immediately after the breathwork intervention using a subset of items adapted from the Theoretical Framework of Acceptability Questionnaire.65,66 This scale is used to measure the acceptability of health care or behavioral interventions. Items were rated on a 5-point scale with anchors that matched each question. Negatively worded items were reverse-scored prior to averaging the items together; higher scores represented greater intervention acceptability. Items to measure general treatment acceptability and treatment satisfaction were rated on a 10-point scale. Additional face-valid questions were used to assess other domains of treatment acceptability.
Outcome measures
The Pain, Enjoyment, and General Activity Scale (PEG-3 67 ) is a measure of pain intensity and pain interference that was used to determine clinically meaningful effects. As the PEG-3 is recommended as a primary outcome measure in pain research, it is the planned future primary outcome measure that will be used to determine intervention efficacy if a larger trial is indicated. 68 It asks participants to rate their pain, on average, over the past week as well as how much their pain interfered with their enjoyment of life and general activity on a 0- to 10-point scale. Scores were averaged; higher scores represented greater levels of pain intensity and pain interference. Research defines a 2-point improvement in the PEG-3 score as clinically meaningful. 62 The Patient Global Impression of Change (PGIC) was assessed at the follow-ups only and asked participants how much their pain improved since the breathwork session, which is another indicator of clinical importance.
The following measures were administered at baseline, 2-week, and 6-week follow-ups. The Pain Catastrophizing Scale measured catastrophic thinking related to pain. 69 The PROMIS Sleep Disturbance Short-Form 6a assessed participants’ perceived sleep over the previous week. 70 The Patient Health Questionnaire-2 and Generalized Anxiety Disorder-2 assessed the frequency of depressive and anxiety symptoms over the past 2 weeks, respectively.71,72 The PROMIS Prescription Pain Medication Misuse Short-Form assessed the frequency of behaviors related to the inappropriate use of prescription pain medication in the past week. 73 The Mindful Reappraisal of Pain Scale measured the extent to which individuals reinterpret pain in a nonthreatening, mindful way. 74 The trait version of the Nondual Awareness Dimensional Assessment evaluated the frequency with which participants reported having self-transcendent experiences in daily life. 75 Before and after the breathwork session, participants completed the state version of the Nondual Awareness Dimensional Assessment, 75 the Emotional Breakthrough Inventory, 76 and reported their current level of pain intensity and pain unpleasantness. The PEG-3 was administered daily for 6 weeks as an exploratory measure but was not included in the current analyses to maintain focus on the primary aims of this study.
Statistical analysis
Descriptive statistics were used to describe baseline characteristics and study feasibility, evaluate intervention acceptability, and examine changes in the outcomes. Consistent with the models of intervention development, 51 the primary focus was on feasibility, treatment acceptability, and proof-of-concept that the intervention could produce clinically meaningful effects for the planned future primary outcome measure. To demonstrate proof-of-concept, we calculated the proportion of individuals who reported a clinically meaningful improvement in pain intensity and pain interference, which was defined as a ≥ 2-point change in the PEG-3 score. 62 We also examined the number of individuals who met the criteria for the treatment response in pain intensity according to the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) recommendations, with 30–50% improvement representing a clinically important effect and > 50% improvement representing a substantially clinically important effect. 77 As this study was primarily designed to examine intervention acceptability and feasibility, all outcome analyses were considered exploratory. Analyses were conducted using SPSS version 30.0.
Results
During the 1-week recruitment period (June 3–7, 2024), 15 participants were screened and deemed eligible for this study. Four were unable to attend any breathwork session and did not contribute the study data, resulting in a recruitment rate of 73.3%. One participant withdrew prior to the start of the intervention due to unrelated personal reasons and only completed the baseline survey. The remaining 10 participants (90.9%) adhered to the single breathwork session. However, it was determined that after the session, one participant lacked sufficient English proficiency to complete the postsession surveys and did not provide additional study data.
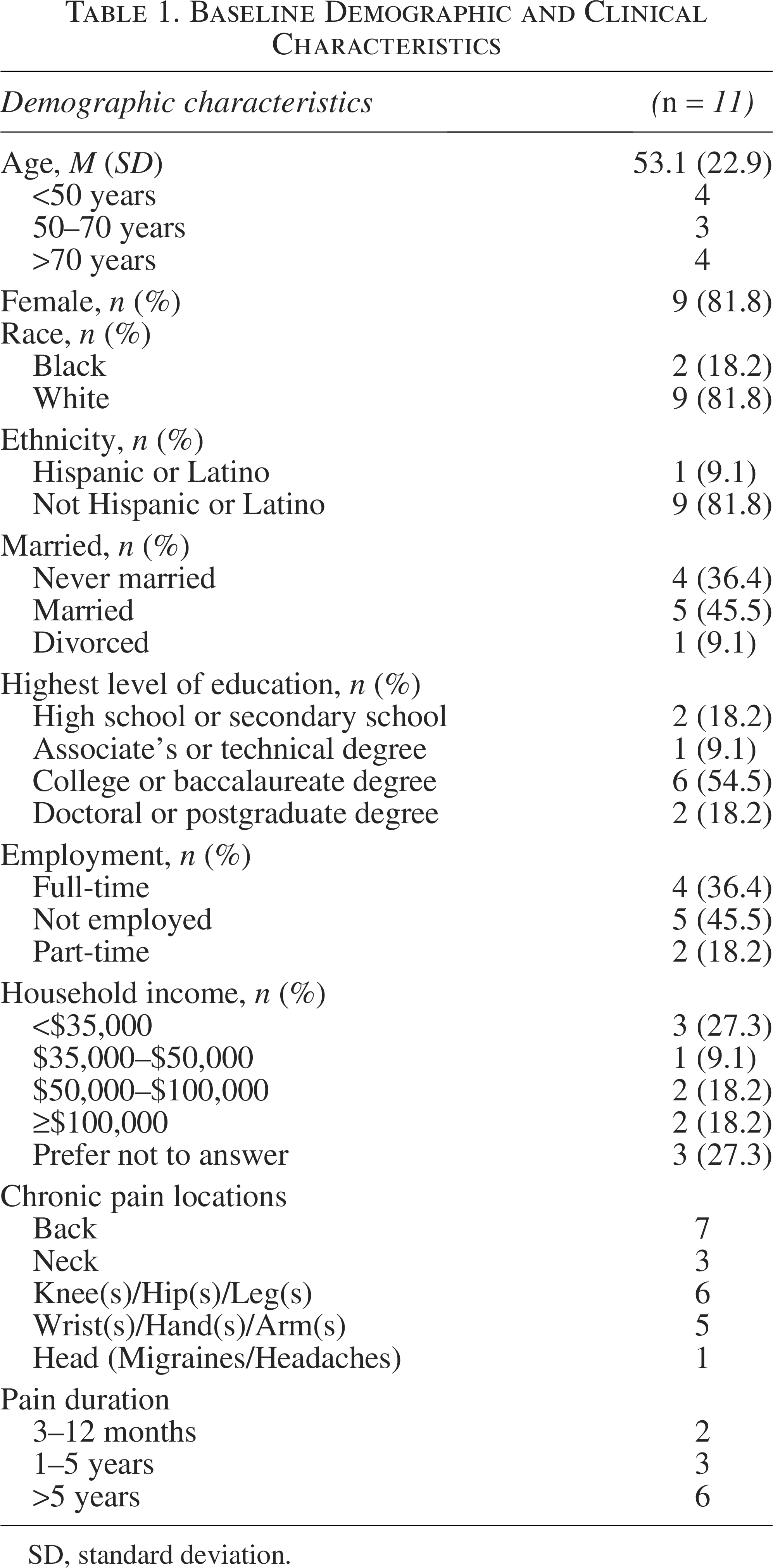
Table 1 shows the baseline demographics and clinical characteristics of participants. The sample was predominantly female (81.8%), with an average age of 53.1 years (SD = 22.9, range = 19–82). Participants reported chronic pain at multiple sites, with musculoskeletal pain being the most common type, including persistent pain in the low back, neck, and knees. Most participants had chronic pain for > 5 years.
Baseline Demographic and Clinical Characteristics
SD
Treatment acceptability
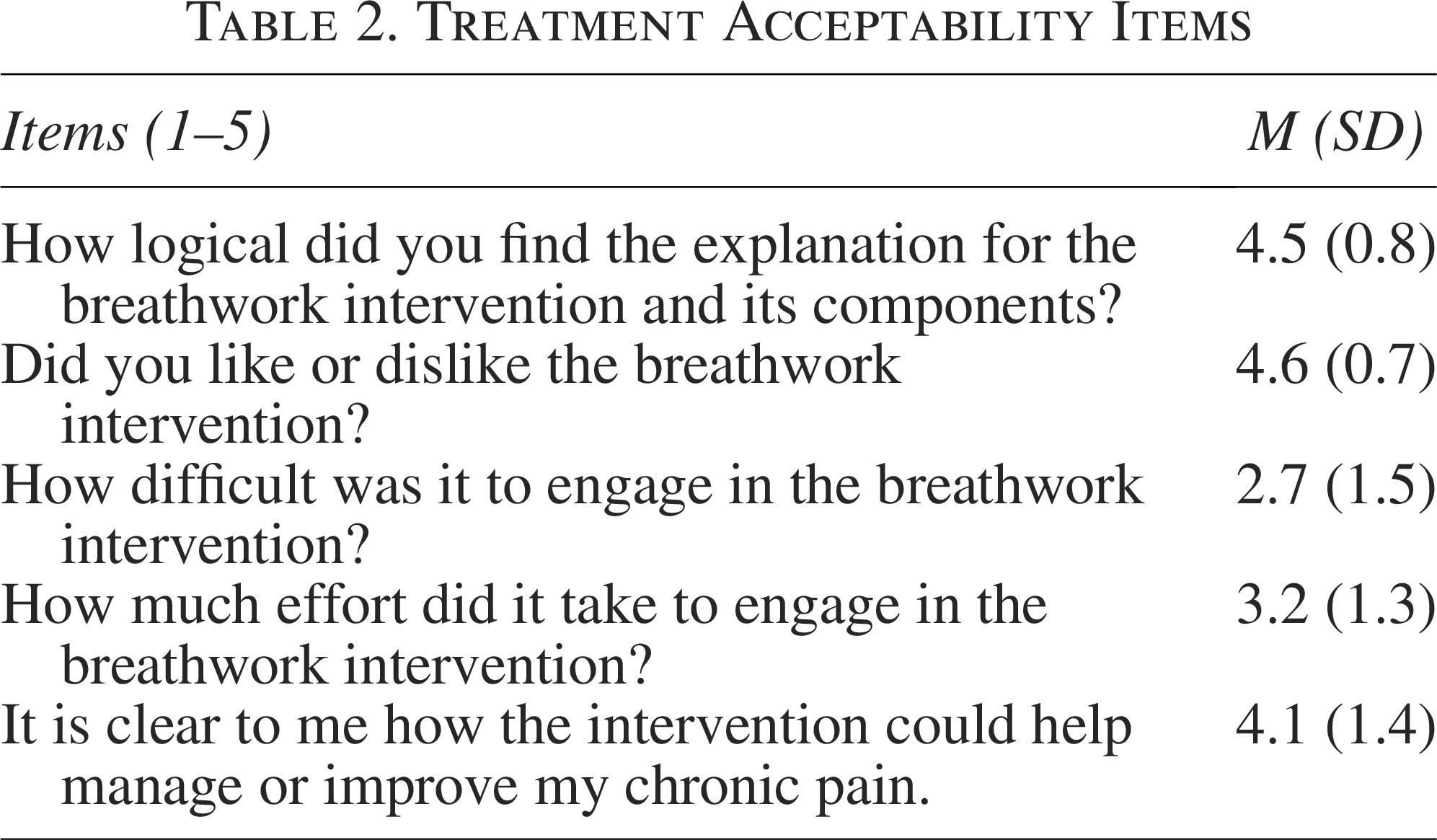
The intervention was rated as highly acceptable (M = 9.3, SD = 1.9) and satisfying (M = 9.7, SD = 0.5), with 90% of participant ratings being >8 out of 10. All participants indicated that they would recommend the intervention to someone else suffering from chronic pain. Table 2 shows the participant responses for additional acceptability items. Participants found that the intervention was logical and thought that it could potentially help manage or improve their chronic pain. They reported moderate difficulty and effort to engage in the intervention but liked it overall. Most participants (60%) indicated that they were willing to attend at least eight more breathwork sessions. Half of the participants (50%) indicated that it would be reasonable to ask others with chronic pain to attend two to four sessions; 40% indicated that it would be reasonable to ask others with chronic pain to attend at least five to eight or more sessions. There were no adverse events or concerns with the safety of the intervention.
Treatment Acceptability Items
Proof-of-concept
The means, SDs, and Cohen’s d effect sizes are displayed in Table 3 for the outcome measures. There were large within-person effect sizes for improvements in pain intensity and pain interference from baseline to the 2-week follow-up (d = 1.3) and 6-week follow-up (d = 1.1). A clinically meaningful improvement in average pain intensity and interference over the past week was observed in five of nine participants at the 2-week follow-up (mean difference [MD] = −2.9, SD = 2.2) and six of nine participants at the 6-week follow-up (MD = −3.5, SD = 3.2). When examining only the pain intensity item from the PEG-3, two participants reported >50% reductions and three reported 30%–50% reductions at the 2-week follow-up; four participants reported >50% reductions and two reported 30%–50% reductions at the 6-week follow-up. These findings are consistent with PGIC scores, in which six of nine participants reported that their pain was much improved or very much improved at the 2-week follow-up and five of nine at the 6-week follow-up.
Clinical Outcome Measures at Baseline and Follow-Ups
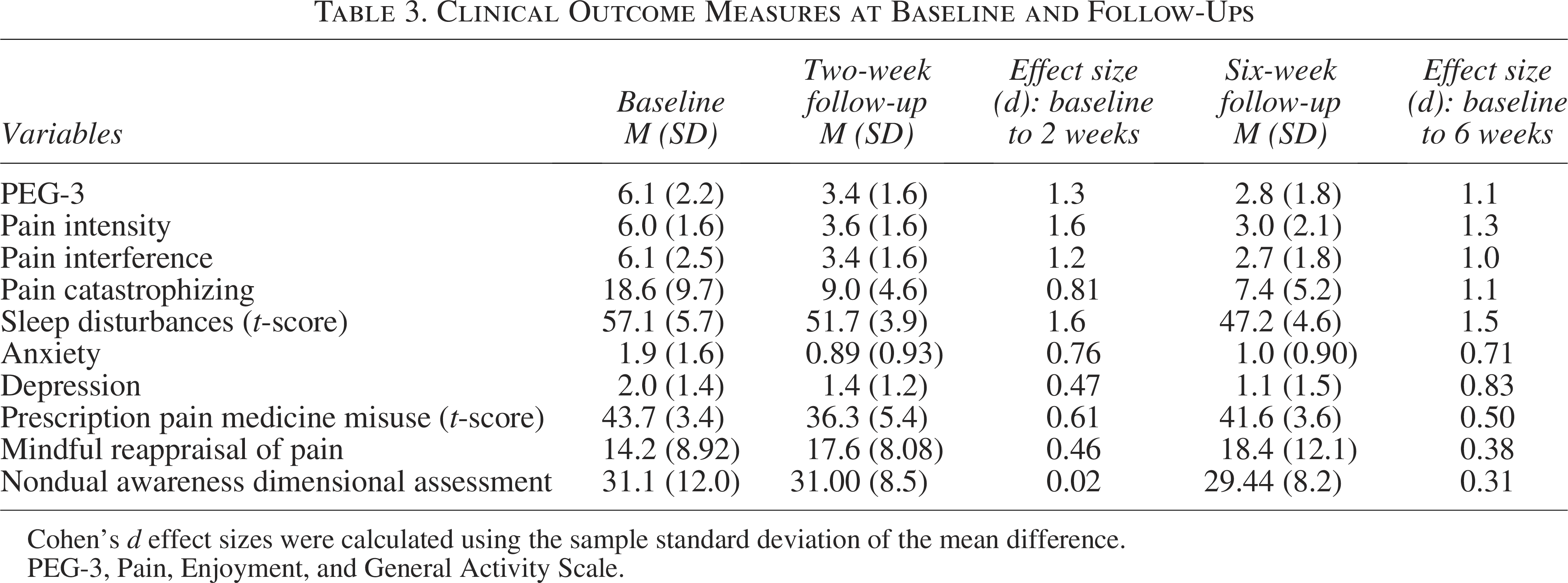
Cohen’s d effect sizes were calculated using the sample standard deviation of the mean difference.
PEG-3, Pain, Enjoyment, and General Activity Scale.
As shown in Table 3, there were large effect sizes for improvements in pain catastrophizing and sleep disturbances from baseline to the 2- and 6-week follow-ups. A clinically meaningful improvement in pain catastrophizing (i.e., ≥6.8-point change) 78 was observed in four of nine participants at the 2-week follow-up (MD = −9.3, SD = 11.4) and six of nine participants at the 6-week follow-up (MD = −11.1, SD = 10.2). There were medium-to-large effect sizes for anxiety and depression at the 2- and 6-week follow-ups and small-to-medium effect sizes for mindful reappraisal at the follow-ups. Of the six participants who reported a pain medication prescription at baseline, there was a medium effect size for improvement among the five participants who completed the follow-up assessments. A small effect was observed for decreases in the trait measures of nondual awareness at the 6-week follow-up, with no change at the 2-week follow-up.
As measured immediately before and after the breathwork session, there were clinically meaningful changes in pain intensity (MD = −2.3, SD = 1.3) and pain unpleasantness (MD = −3.3, SD = 1.57). Participants reported a significant increase in the state measure of nondual awareness during the breathwork intervention (MD = 3.8, SD = 2.1, F = 29.8, p < 0.001), but not for the measure of emotional breakthrough (MD = 1.0, SD = 2.4, F = 1.4, p = 0.27).
Discussion
The goal of this trial was to evaluate the acceptability, feasibility, and potential clinical benefits of a single group session of GRMT in a sample of adults with chronic pain. The integrative breathwork intervention was safe and well-tolerated, with high levels of treatment acceptability and satisfaction. Moreover, all participants reported that they would recommend the intervention to someone else suffering from chronic pain, and most participants were willing to attend more than eight additional breathwork sessions. The study was feasible, with high rates of participant recruitment and intervention adherence. The findings demonstrated proof-of-concept by meeting our targets of success, with most participants reporting a clinically meaningful improvement in pain intensity and pain interference through the 2- and 6-week follow-ups. Although this study was small and uncontrolled, the sustained benefits are noteworthy. The large within-person effect sizes appear to result from a single GRMT breathwork session, without any homework or continued engagement with a self-management practice. As this study was the first test of an integrative breathwork intervention for patients with chronic pain, it provides a positive signal that additional research is warranted.
Notably, there were large improvements in pain catastrophizing following the session of GRMT. Pain catastrophizing is a key treatment target and robust mediator of psychosocial interventions for chronic pain.53,79–81 The clinically meaningful improvement in pain catastrophizing at the 2- and 6-week follow-ups was similar in magnitude to an efficacious single-session pain intervention at 1- and 3-month follow-ups. 55 While many psychosocial interventions teach coping skills and pain neuroscience education, the current study used a breathwork style that may best be considered an experiential intervention. Participants were guided to focus on the strongest sensation with mindful acceptance while maintaining a continuous breathing pattern. This practice may have led to implicit learning to reappraise sensations, including pain, as nonthreatening.36,74 For instance, multiple participants shared that they experienced a new way to be with uncomfortable sensations in their body, which could have led to a different relationship to their pain and less pain catastrophizing over time.
Following the breathwork session, there were medium-to-large within-person effects for other biopsychosocial outcomes, including sleep disturbances, anxiety, and depression. These pain-related symptoms can arise from chronic pain but can also contribute to worse chronic pain over time. 82 Of the limited clinical research on integrative breathwork interventions, preliminary studies have found reductions in stress, anxiety, and depression as well as increases in mindfulness and quality of life.22,32,33 The small within-person effects for mindful reappraisal and nondual awareness at the follow-ups were surprising, as the breathwork intervention included elements of mindful reappraisal. Moreover, other research has shown that a 45-min conscious connected breathing session can alter consciousness to a similar degree as that experienced under the effects of psychedelic substances.19,27,43 These types of experiences are worth exploring because they have been shown to mediate the effects of various therapies for pain, addiction, depression, and anxiety symptoms.83–86 In the current study, two participants reported a self-transcendent experience75,87 after the breathwork session, which may have been captured by the state, but not trait, changes in nondual awareness. Unexpectedly, GRMT did not lead to subjective reports of emotional breakthrough. Integrative breathwork interventions can elicit emotional release and catharsis, however, GRMT is considered a noncathartic style of breathwork. Additional research is necessary to understand whether the subjective experiences that are common during this style of breathwork, such as emotionality, psychological insight, or altered consciousness, are predictive of the treatment response.
While many mindfulness-based interventions have been examined as a treatment for chronic pain,88,89 the integrative breathwork intervention tested in this study is novel. GRMT is better considered a respiratory-based intervention that includes mindfulness as a component to support the variety of experiences that can arise from altering one’s breathing, such as intense physical sensations or emotions. Most mindfulness-based interventions involve the sustained self-regulation of attention to present-moment experiences (e.g., observation of the breath), but the component that best defines breathwork and differentiates it is the sustained conscious connected breathing technique. As the respiratory system is deeply interconnected with the nervous system and other systems of the body, volitionally modifying one’s breathing may have cascading effects on physiological and psychological processes relevant to improving chronic pain and whole-person health that are not influenced by mindfulness alone. For example, conscious breathing may lead to changes in the brain,40,90,91 autonomic nervous system, 92 immune system,27,93 biochemistry,93,94 biomechanics, 95 and state of consciousness.19,23,43,96 GRMT and mindfulness-based interventions also likely share several mechanisms for chronic pain. One promising transdiagnostic factor to investigate is interoception, or the sensing of internal body signals.7,47 Research has shown that mind–body therapies increase interoceptive awareness, which may account for improvements in pain outcomes. 46 Given the small effect sizes for chronic pain typically found from mindfulness-based interventions,88,89,97 it is plausible that additional or alternative mechanisms are engaged with integrative breathwork interventions.
The single-session, group breathwork intervention was an innovative treatment format that represented a naturalistic setting (e.g., breathwork workshop). Single-session interventions reduce the participant burden and address common barriers to treatment adherence and treatment accessibility. 54 The group format also decreases the cost of delivering the intervention and increases the scalability to reach more individuals with fewer resources. Several studies have found that single-session psychosocial interventions can produce clinically meaningful improvements in chronic pain and pain-related outcomes.61,98 A single session of a skills-based intervention (“Empowered Relief”) was noninferior to 8-weeks of cognitive behavioral therapy for adults with chronic low back pain through 6-month follow-up.53,55 For integrative breathwork interventions, there may be a dose–response relationship, where treatment effects are stronger after additional sessions. Research is underway investigating whether an 8-week version of GRMT is feasible, acceptable, and clinically helpful for adults with chronic low back pain.
Limitations
There are several limitations for this study. First, without a control condition, we are unable to determine whether the changes in the outcomes were related to the treatment or other common factors, such as time, attention, or regression to the mean. As most participants reported chronic pain for >5 years, it is unlikely that the effects were a result of natural history. Nevertheless, randomized controlled trials with appropriate comparison conditions are necessary. Second, this study was limited by a small sample size that may be vulnerable to self-selection bias. As this was a proof-of-concept study, it was neither powered nor designed to test for statistically significant effects of treatment efficacy. Thus, the results are exploratory and focus on descriptive statistics and clinical significance to provide initial information about the intervention. Third, the sample comprised patients with various chronic pain conditions. Although there were benefits to this heterogeneity to learn about the safety, acceptability, and preliminary efficacy of the intervention for different types of chronic pain, future research will require homogenous samples to make conclusions on the efficacy for specific populations. Lastly, the results may have been influenced by therapist effects, as the developer of GRMT delivered the breathwork sessions. Additional research should examine whether the effect sizes and treatment acceptability ratings are maintained when the intervention is delivered by trained individuals with less expertise.
Conclusion
A single group session of an integrative breathwork intervention was shown to be highly acceptable, satisfying, and potentially helpful to individuals with chronic pain. The majority of participants reported clinically meaningful improvements in pain intensity and pain interference that were sustained at the 2- and 6-week follow-ups. As GRMT has never been tested before in chronic pain populations, this proof-of-concept study provides a positive signal that this novel breathwork intervention may improve pain and pain-related outcomes, including sleep disturbances, anxiety, and depressive symptoms. Given its promise as a nonpharmacological intervention for chronic pain, future research is needed to evaluate GRMT compared with an appropriate control condition in larger randomized controlled trials.
Authors’ Contributions
S.D.P.: Conceptualization, data curation, formal analysis, methodology, writing—original draft. L.L.: Investigation, writing—review and editing. A.D.: Investigation, data curation, writing—review and editing. A.W.H.: Conceptualization, data curation, formal analysis, methodology, writing—review and editing.
Footnotes
Author Disclosure Statement
L.L. reported receiving personal fees for consulting on the project and training providers in this intervention.
Funding Information
This study was supported by the grant K01AT012066 (S.D.P.) from the National Center for Complementary and Integrative Health.