
Abstract
Purpose:
Veteran’s Affairs Whole Health system of care emphasizes a person-centered and proactive approach to self-care and well-being. Since personal values and locally available resources may affect these motivations among rural-dwelling female Veterans, we examined perceptions of self-care practices, views about what ideal health care entails, and recommendations for support among rural-dwelling female Veterans.
Method:
This study is part of a larger quality improvement project that evaluated a clinician-delivered telehealth outreach program. Twenty-one female Veterans (age range 22–85 years) participated in qualitative interviews.
Results:
Veterans reported engaging in a variety of self-care practices. Notably, being physically active outdoors was important, and many choose to live in rural communities to access outdoor activities. Veterans also found importance in community-based connection (e.g., participating in faith communities). Some Veterans noted challenges with accessing activities and having smaller social networks due to their rurality; thus, Veterans also saw a need for groups or events focused on community building to help foster community among women Veterans. When asked about ideal health care, multiple Veterans wished for less emphasis and reliance on medications, instead desiring more emphasis on holistic care and increased access to complementary and integrative health (CIH) approaches.
Conclusions:
These findings indicate that rural-dwelling female Veterans engage in myriad self-care practices and see their ideal health care as including more CIH approaches. These data support continued investment in CIH as part of the broader VA Whole Health initiative and the importance of health care teams helping facilitate nonpharmacologic interventions.
Introduction
In recent decades, Veterans Affairs (VA) health care systems have moved toward patient-centered approaches to improve Veteran engagement, self-activation, and well-being in the management of their health. This is notably anchored in the development of the Whole Health System model of health care aimed at empowering and equipping Veterans to “take charge of their health and well-being and to live their lives to the fullest.” 1 Whole Health programming emphasizes proactive, whole-person care and may include the use of trained Whole Health coaches and complementary and integrative health (CIH) strategies, such as yoga, tai chi, and acupuncture. 1 Importantly, Veterans do not need to endorse disease or disorder to access Whole Health services. Focusing on understanding what matters most to the Veteran and supporting associated goals potentially provides a means to better manage multiple chronic conditions and complex health needs.2,3
Female Veterans experience higher rates of chronic illness and have a higher burden of medical complexity compared with male Veterans.4,5 Rurality poses an additional challenge, as those living rurally encounter significant difficulties in accessing health care, often resulting in lower utilization. 6 In rural settings, access to health care is impacted by structural barriers, such as driving distance to a clinic, clinics with limited resources, frequently overburdened providers, and a limited number of specialists, especially those with expertise in female-specific care needs. 6 Studies have shown that rural residence is associated with lower odds of using CIH approaches compared with their urban counterparts. 7 Considering the strain of managing chronic conditions and overtaxed health care systems, there is increased interest in how best to support individuals in self-care practices that promote positive health outcomes.
“Self-care” can function as a patient-driven strategy to complement health system efforts and can employ the individual, families, and communities to support individuals’ well-being, prevent disease, and manage illness, which can be accomplished with or without the support of formalized clinical treatment. 8 The meaning of self-care is often unprecise due to the challenges of integrating definitions across medical and research contexts and the proliferation in the social milieu. The World Health Organization defines self-care as “activities that individuals, families, and communities undertake with the intention of enhancing health, preventing disease, limiting illness, and restoring health. These activities are derived from knowledge and skills from the pool of both professional and lay experience. They are undertaken by laypeople on their own behalf, either separately or in participative collaboration with professionals” (p. 2). 9 Self-care may encompass physical, psychological, emotional, spiritual, and professional domains 10 and include things like healthy diet, regular exercise, engaging in fun and/or intellectually stimulating activities (e.g., singing, reading, movies), social connection, and prioritizing health care. 11 Social connection, inclusive of social support, is a well-documented protective factor for mental health conditions. 12 As such, self-care practices can play an important role in successful management of well-being, mitigating downstream health conditions.
Among rural female Veterans, individual values and access to resources in rural communities may underlie different types of self-care management. In addition, attitudes around what is popular and accepted as conventional are likely to affect the perceptions of self-care as self-care practices are based upon cultural scripts and moral beliefs. 13 Self-care practices are often promoted toward women, 14 which is likely reflected in that being a female is a factor that increases CIH use among Veterans.7,15
Although studies have examined rural male Veteran perspectives on self-care as it relates to mental health, showing a range of activities (e.g., hiking, working with one’s hands through gardening or on cars, attending church), 16 research has not yet studied self-care practices in rural female Veterans. Thus, it is necessary to better understand how rural-dwelling female Veterans are perceiving self-care practices (e.g., exercise, activities, social connection) and what ideal health care may entail, with recommendations for improvements, to ultimately support rural-dwelling female Veterans in maintaining well-being.
In this article, we examine perceptions of self-care practices, views about what ideal health care entails, and recommendations for support among rural-dwelling female Veterans.
Materials and Methods
Study overview
This analysis is part of a larger quality improvement project that evaluated a clinician-delivered telehealth outreach program, called the Boost Program, aimed at improving access to and engagement with Veterans Health Administration (VHA) services among rural-dwelling female Veterans. Clinician-driven outreach calls were piloted across five VHA primary care catchment areas within one VHA health care system in Northern California from September 2022 through December 2024. We direct readers to Cohen et al. 17 for additional information on the Boost Program. The research team was comprised of five researchers, including two physicians (J.C. and M.J.), one medical anthropologist (K.A.Z.-R.), one clinical psychologist (C.L.M.), and one nurse practitioner (T.S.), employed by the VHA in urban locations. The two qualitative researchers (K.A.Z.-R. and C.L.M.) did not have any other relationships with the Veterans. We adhered to the policies and procedures delineated by the VHA for the review and conduct of ethical research. According to the VA Electronic Determination Aid, this project was determined to meet the regulatory definition of research in accordance with 38 CFR 16.102 18 but did not meet the definition of human subjects research; therefore, Institutional Review Board review was exempted. The local research office reviewed and approved the final project.
Participants
Female Veterans who completed a Boost outreach call (n = 543) and completed a brief assessment (n = 100) were invited to participate in a 30-minute semistructured interview. Given that the patient population at VA is predominantly older (median age of 60+ years old), 19 we oversampled for younger Veterans (under 50 years of age). Verbal informed consent was obtained from all participants prior to participating in an interview.
Data collection
Participant age, race, and ethnicity data were collected through chart review of individuals’ VA electronic health records. Data on race and ethnicity are obtained by the VA in accordance with mandates from the Office of Management and Budget, which outlines the use of standards including self-identification of race and ethnicity using the following categories: American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or Pacific Islander, White. For this project, Veterans who self-reported multiple races were coded as “multiracial.”
We developed original semistructured interview guides, which focused on participants’ feedback on the Boost telehealth outreach program, prior and current experiences seeking female health care services in rural communities, self-care practices, views on social connection, and perspectives on notions of “ideal care.” 18 The current article focuses on participant views on what their current self-care and social connection entails and what their ideal health care would look like. Interview guides did not change during data collection. Two qualitative researchers conducted each 30-minute telephone interview from June 1, 2023, through June 1, 2024, and interviews were audio-recorded for analysis. All recruitment tracking spreadsheets and data were stored and retained in accordance to local VA policy. Data were deidentified with study IDs not linked to identifiable information. Audio files will be destroyed after the completion of the project.
Data analysis
We used a Rapid Qualitative Analysis approach, within an interpretivist paradigm, developed for health services research settings, which allows for qualitative results to be analyzed concurrently with data collection.20–22 Guided by our semistructured interview guides, we created summary templates using Microsoft Excel organized by topical area. A qualitative team member listened to each audio-recorded interview and populated a summary template with key points and quotations. To ensure reliability and mitigate researcher bias, a second qualitative researcher listened to the audio-recorded interview and reviewed the summary for accuracy. To synthesize data, we used a matrix analysis, an approach to displaying data to highlight commonalities and differences and to identify patterns and relationships.20,21,23 We created a Veteran findings matrix using Microsoft Word organized by domains in the interview guide to compare feedback across participants. The two qualitative team members met weekly throughout the concurrent data collection and data analysis phases to ensure consensus of emergent themes. Consensus was reached between the two analysts through discussion of any discrepancies. Finally, the two qualitative team members met with the larger study team bimonthly to discuss preliminary findings, with the interdisciplinary viewpoints of team members encouraging collaborative reflexivity. 24
Results
Twenty-one female Veterans, between the ages of 22 and 85 years (M = 56.8; SD = 16.9), participated in the interviews. Veterans identified as White (67%; n = 14), American Indian or Alaska Native (5%), and multiracial (19%) and none as Hispanic/Latino. Several themes emerged across 21 Veteran interviews.
Theme 1: Veterans engage in a wealth of activities they define as “self-care,” including indoor and outdoor activities
Participants reported that staying active and/or physically fit (e.g., exercising at the gym or attending a Pilates class, moving one’s body) is especially important. Veteran 008 noted that her morning workouts are an activity during which she can take time for herself in contrast to more community- or family-focused activities (Table 1).
Qualitative Findings and Quotes
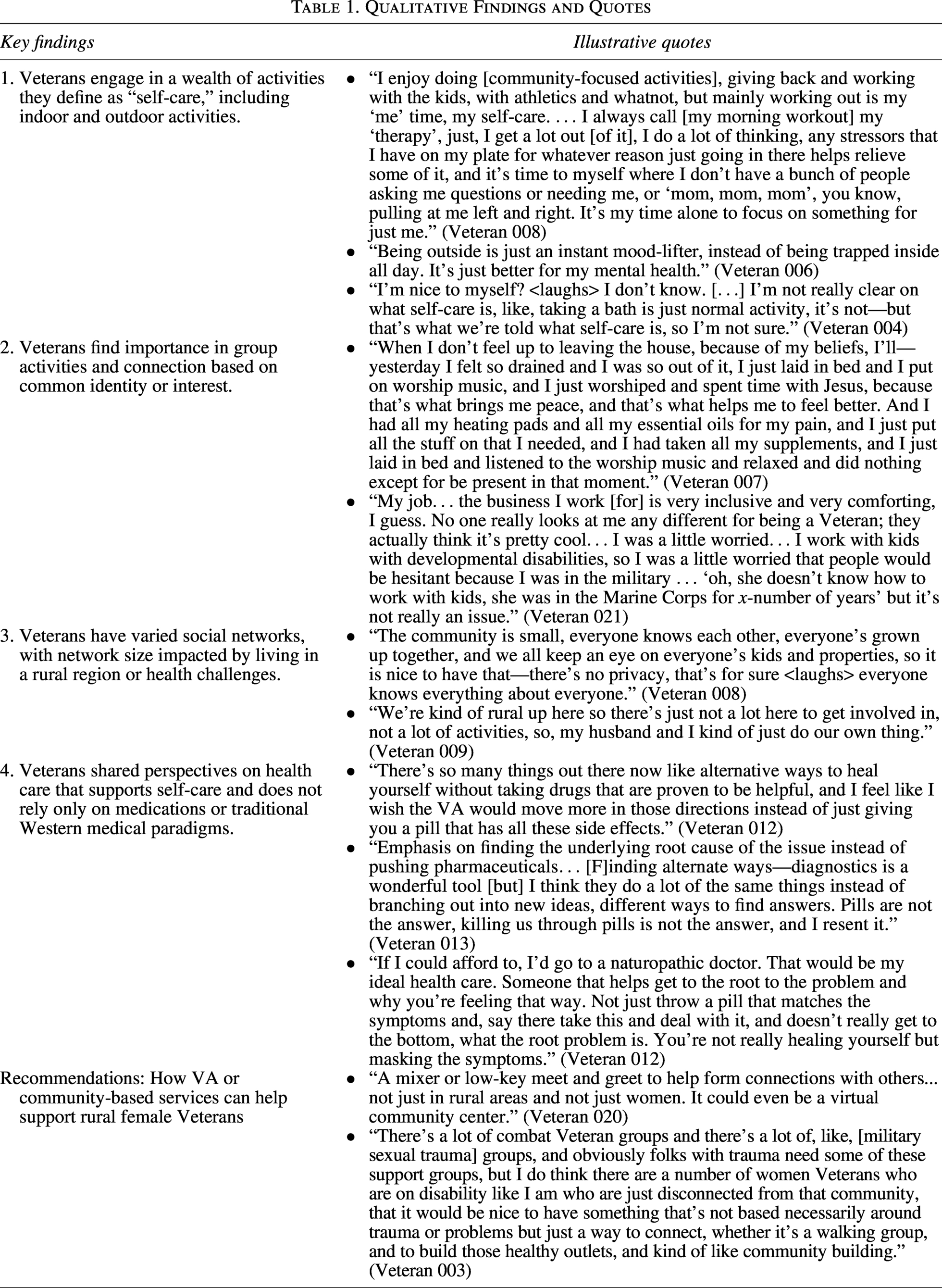
Many Veterans endorsed the importance of outdoor activities, whether related to exercise, such as hiking, water sports (e.g., boating, kayaking, rafting), or walking dogs, or other outdoor activities, such as camping, fishing, gardening, and attending live music events. Veteran 006 noted the importance of spending time outdoors on her mental well-being (Table 1). Similarly, Veteran 011 reflected on the lack of social events in her rural town, making having a dog to help her get outside and take walks valuable for improving her overall health. Veteran 011 added that she notices a difference in her health; she does not go on walks.
Veterans also prioritize indoor activities, especially when the weather or their physical health limits outdoor or physical activities (e.g., crocheting, writing cards and letters, reading, watching movies and TV shows, cooking, building kits). Veteran 017 noted that it is challenging to be outside during the winter season due to rain and weather; thus, she focuses on self-care activities such as healthy eating and stretching during these seasons.
Veterans also reported enjoying activities like hunting, target shooting, and making knives. Veteran 001 shared that although she did not have an interest in firearms after first separating from the military, she decided to start target shooting for self-defense and now practices at a shooting range 1–2 times per week. She likes “being in competition with myself, to be more accurate, figuring out what I’m doing wrong so that the next time I go I can be even a better shot.” Veteran 001 added that she has also gotten to know some of the regulars at the shooting range, and thus, this new hobby has expanded her social network.
However, several Veterans were unsure what to consider self-care when asked. Veteran 013 described doing what she calls “the basics,” such as healthy eating (e.g., organic grass-fed meat), prioritizing sleep, and limiting daily alcohol consumption, stating “I’ve changed my coping skills.” She added that she is “kind to myself and give myself grace” as forms of self-care. This attitude of kindness to self and to others was echoed by other Veterans as an important self-care approach. Veteran 020 practices gratitude and a positive outlook about life, including simple things like smiling at or complimenting someone. Although at times she feels down, “I allow myself 5-minute pity parties and then move on with living,” applying her positive outlook. Another respondent, Veteran 004, reflected that she is not sure of what is meant by “self-care” as she reflected that some self-care practices seem like activities of daily living according to popular culture (Table 1).
Theme 2: Veterans find importance in group activities and connection based on common identity or interest
Veterans described their faith and faith-based activities, such as attending church or Bible study, as important aspects of their self-care. Veteran 007 stated that her family attends church and Bible study together, and even when she is unable to leave her home due to chronic pain, she finds ways to connect to her faith and faith community through worship [practices at home] (Table 1). Similarly, Veteran 015 named her church, including a women’s Bible study group, as her primary source of social connection and community.
Other respondents reported finding connection through Veteran-centric organizations, including the American Legion, and community events, such as a Veterans’ ceramics group. Veteran 011 attended a ceramics class for Veterans, which was the first time she met other women Veterans in her locality, making the group function as an informal support group. Veteran-centric support may be especially salient for self-care, as Veteran 021 noted hesitancy in how people might view her as a military Veteran in her workplace (Table 1). Some respondents also engaged in events with neighbors at a community center where people get together, volunteering (e.g., working in a community garden, food bank), being in a community band, and through sports. Veteran 011 believes that people are healthier when in community, stating how “Especially as we get older, people are healthier if they are in community in some way.”
Theme 3: Veterans have varied social networks, with network size impacted by living in a rural region or health challenges
Many people discussed relying on a variety of people for social connection, notably spouses, family, and new and old friends. Veteran 008 noted that she lives in the house she grew up in, and her neighbors across the street are the same family as from when she was younger (Table 1).
However, several respondents acknowledged challenges with developing and maintaining friendships while residing in rural regions, noting the importance of travel to visit loved ones. For example, Veteran 009 prioritizes traveling to visit her grandchildren (Table 1). For Veteran 010, her largest social group is family and long-time friends who are in the mid-West, where she grew up. She described visiting 3–4 times per year and staying in touch via Facebook Messenger and telephone.
Some participants described how health and lifestyle challenges affect their engagement with social networks. Veteran 017 has family and friends in her town of 1500 people but reflected that “when you’re ill, when you’re hurt—you’re not doing that [social] stuff.” Similarly, Veteran 003 noted that due to disability for major depressive disorder, she spends most of her time by herself, and if she is not staying active and engaged in activities, her depression can become severe, especially in the winter. Physical and mental health conditions can substantially impact social connection and may be exacerbated in rural regions with less available community activities.
Theme 4: Veterans shared perspectives on health care that supports self-care and does not rely only on medications or traditional Western medical paradigms
Veterans noted the importance of nonpharmacologic approaches to maintaining their well-being. A few Veterans detailed relying on natural remedies to help manage health concerns and with relaxation, including herbs, supplements, essential oils, massage, yoga, tai chi, and heating pads. Veteran 012 stated that she does research to find ways to address her health concerns in minimally invasive ways (Table 1). Some participants discussed relying on alternative practices to help manage pain specifically. For example, unable to exercise due to pain, Veteran 017 focuses on nutrition, stretching, using a heating pad, and rest and avoiding medication when in pain. Another respondent, Veteran 019 identified as a naturopath, not a medical doctor, and that she is currently studying dietary and nutritional needs. She has spinal injuries and thus has adjusted to her physical needs by instead focusing on taking supplements and doing yoga and tai chi.
Veterans generally reported wanting to see nonpharmacological and integrative health modalities emphasized in their clinician-directed health care and to de-emphasize reliance on pharmaceuticals. Veteran 011 stated, “If you can treat yourself without meds, that’s much better. I’m a big fan of the Whole Health thing,” a sentiment that was reflected by others (Table 1). Relatedly, Veteran 012 described her ideal care as entailing going to a naturopathic doctor (Table 1). Veteran 013 similarly described seeking more education around nutrition, stating that the food pyramid is outdated.
Recommendations: How VA or community-based services can help support rural female Veterans
Veterans suggested creating social groups offering different opportunities for female Veterans to get together, including events focused on community building whether virtual or in-person and outside of the clinic (Table 1). Veteran 002 suggested creating outdoor events that take advantage of what is available in the region (e.g., access to nature in northern California), such as walking groups or group boating events. Veteran 003 emphasized a need for groups that are not necessarily based on shared trauma or shared health condition but instead offer opportunities for community-building (Table 1). Generally, Veterans were open to meeting at their local VA outpatient clinic or in the community/region to participate in these activities.
For resources already available to Veterans within the VHA, Veterans noted wanting easier access to and increased number of wellness services offered (e.g., chiropractic care, acupuncture, massage therapy, reiki, yoga), as VA allows a set amount of time to use authorized wellness visits. To further increase access, one Veteran suggested having wellness services approved as part of routine care at VA, in the same way that an annual primary care doctor visit and lab work are given each year.
Discussion
In the present qualitative analysis, we sought to understand self-care practices, perspectives on what ideal health care might entail, and recommendations for support among rural female Veterans. Veterans described numerous practices that they defined as “self-care,” including many community-based activities and engaging with their varied social networks. In describing their ideal health care, Veterans desired less emphasis and reliance on medications, more emphasis on holistic care, and increased access to CIH approaches as part of “ideal care.” Recommendations for how VA or community-based services can help support rural female Veterans are centered around community building events and often with an outdoor focus. Our findings suggest that self-care and community engagement can take many forms; thus, support for Veteran’s well-being needs to be individualized.
Recent studies have shown how the attitudes about what is regarded as conventional in popular culture may further impact what is perceived as self-care, often with a focus on “pampering” and “luxury” through consumerist behaviors, including beauty products most often marketed toward women.14,15 Considering that some respondents were unsure of how to define self-care, or how these practices might differ from self-care products advertised toward women, education about self-care practices and their relationship to personally valued activities may be of particular relevance among Veterans. Diverse activities are important to highlight as some Veterans may not resonate with conventional outlets and use alternative ideas as a launching point (e.g., target shooting, blacksmithing). Prevalent participation in faith-based activities suggests that provider education around faith and spiritual needs may also be useful in supporting discussions about faith within the medical context.25,26 Many female Veterans practiced self-care, although some listed barriers, including physical and mental health limitations, along with weather or access-related barriers. These challenges are likely barriers to engaging in self-care practices and community support and those that are mutable, such as isolation, tailored interventions, including psychoeducation and behavioral activation, may be especially crucial for individuals identifying such challenges.
Rural female Veterans highlighted the importance of holistic care and an interest in CIH approaches when asked about what their ideal care would entail. This finding aligns with other data showing that Veterans demonstrate considerable interest in CIH modalities, yet there remains limited CIH availability.15,27 In 2017, over half of Veterans sampled had used a CIH modality in the prior year, 26 and further evaluation from 2016 to 2019 demonstrated a 70% increase in CIH use over that time frame. 15 Among recently returned Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn Veterans, females were more likely than males to use CIH modalities, especially meditation and spiritual healing, 28 suggesting the appeal of these types of interventions for female Veterans. A patient-centered Whole Health approach appears to be important in improving the long-term care for rural female Veterans, which is supported by preliminary research on well-being-related outcomes and reduction in invasive pain treatment procedures.29–31 However, while VA has made considerable gains in offering CIH services, structural access inequities in rural VA Whole Health delivery remain.7,15
Given these findings, we recommend supporting care team members through increased education on available services, including coaching and CIH, to aid in promoting patient-centered care and disseminating information to Veterans directly. As health care systems and providers are overburdened, leveraging nonprovider roles, such as peer-support specialists, may be particularly effective in supporting engaging Veterans in Whole Health.
Limitations
This study’s findings should be considered in relation to its strengths and limitations. This study sampled from rural VA outpatient clinics on the west coast; thus, findings may not be transferable to Veterans in other rural regions across the United States nor to those in urban regions or non-VA settings and civilian samples. Considering VA comprises patients that are predominantly male and older in age, the current sample may not transfer to the VA patient population broadly.
Conclusions
This work demonstrates the importance of recognizing a holistic approach in the provision of care and recognizing the individual strengths and challenges of rural female Veterans in supporting their self-care and social connections. The recent priority and implementation of VA’s Whole Health System of care maps onto rural female Veterans’ perceptions of “ideal care,” suggesting that these services may positively impact patient engagement and self-management of personal well-being and health care. Future studies should assess continued use of Whole Health services, including nutrition, biofeedback, and coaching, which can be delivered by VA staff through telehealth modalities, and long-term impacts on well-being and health. For rural Veterans, CIH care offerings that can be delivered via telehealth are especially advantageous to reduce the reliance on travel to VA and/or community care. Notably, Veteran’s express a desire for improved access to CIH, yet given real-world constraints (e.g., geographic, limited CIH availability, Whole Health budgets) and variation in implementation across VA health care systems, system capacity remains insufficient. As effective and relevant programming is crucially needed to support the self-management needs of Veterans, this qualitative study provides evidence to support continued investment in VA Whole Health services.
Authors’ Contributions
C.L.M., J.C., and K.A.Z.-R. contributed to the concept, design, analysis, and article. C.L.M. and K.A.Z.-R. conducted interviews and interview analysis. All authors reviewed and approved the final article. M.J. and T.S. contributed to project investigation and administration.
Footnotes
Acknowledgment
The content is solely the responsibility of the authors and does not represent the views of the Department of Veterans Affairs or the U.S. Government.
Author Disclosure Statement
The authors have declared that no competing interests exist.
Funding Information
This work was funded by the Department of Veterans Affairs, Veterans Health Administration, Office of Rural Health, NOMAD #PROJ-03878.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.