
Abstract
Background:
Dietary and herbal supplements are widely utilized around the world. These products can cause adverse effects, including nephrotoxicity, through pharmacologically active ingredients, contaminants, or drug–herb interactions, even though they may be perceived as safe. While nephrotoxicity is well documented for certain pharmaceuticals, there are limited studies regarding safety concerns of nephrotoxicity associated with natural products.
Objective:
To identify signals for possible nephrotoxicity involving natural products using the Food and Drug Administration Adverse Event Reporting System (FAERS) database.
Methods:
A retrospective analysis of FAERS data (2004–2021) was conducted using the medical dictionary for regulatory activities (MedDRA) terminology to identify possible signals of nephrotoxicity with natural products. Disproportionality analysis was completed by calculating the reporting odds ratio (ROR) for signal detection. Significant signals (ROR ≥ 2.0 with 95% CI lower bound ≥ 1.0) with a case count greater than one were then supplemented by a literature review for clinical and preclinical evidence.
Results:
The analysis identified 231 nephrotoxic event–natural product pairs, representing disproportionate reporting signals for 63 natural products. Three significant signals were detected from a total of 15 cases, including ginger (n = 11) with an ROR (95% CI) of 6.21 (3.85–10), butcher’s broom (n = 2) with an ROR (95% CI) of 7.99 (2.56–24.94), and valerian (n = 2) with an ROR (95% CI) of 2.03 (1.09–3.78).
Conclusion:
While definitive associations between natural products and nephrotoxicity could not be established using a disproportionality analysis, the presence of significant signals for ginger, butcher’s broom, and valerian with respect to kidney-related adverse events highlights the need for further investigations and monitoring by clinicians.
Keywords
Introduction
The United States Food and Drug Administration (FDA) defines a dietary supplement as something that is “intended to add or supplement the diet and is different from conventional food.” 1 About one-third of adults in developed countries and more than 80% of the population in low- and middle-income countries use herbal and traditional medicines. 2 According to the National Center for Health Statistics, 57.6% of adults over 20 years of age have used a dietary supplement in the United States within the past 30 days. 3 From 2007–2008 through 2017–2018, the overall supplement usage increased in all age groups and is expected to keep increasing. 3
Despite a perception of being safe by consumers, dietary and herbal supplements may cause adverse events secondary to their own pharmacologically active ingredients, contaminants, or pharmacokinetic and pharmacodynamic drug–herb interactions.4,5 As utilization of dietary supplements increases, the likelihood of adverse events with these products can also be predicted to increase. In addition, adverse events from herbal products are unpredictable and potentially dose-independent, presenting further risk of harm. There is a need for increased pharmacovigilance among health care professionals and greater awareness among consumers regarding potential harm with dietary and herbal products.
In the context of kidney-related safety concerns, certain chemical drugs/drug classes such as NSAIDs, immunosuppressants (e.g., calcineurin inhibitors), antibiotics (e.g., aminoglycosides), and chemotherapeutics (e.g., cisplatin) have been identified as nephrotoxic with relatively well-known mechanism(s).6–8 In contrast, the data are sparse regarding the potential nephrotoxicity of dietary and herbal supplements.9–13 Speculation about kidney-related adverse effects from using dietary and herbal supplements is anticipated due to their unique properties, including high blood flow rates, large endothelial surface areas, high metabolic activity, and active uptake by tubular cells. 2 It is noted that up to 16% of drug-related, hospital, and community-acquired acute kidney injury (AKI) events are attributed to herbal medicines for adult patients admitted to nine hospitals in China. 14
The aim of the present pharmacovigilance study was to investigate possible nephrotoxicity of various natural products using real-world data from the FDA Adverse Event Reporting System (FAERS). 15 FAERS is one of the largest and most well-known publicly accessible post-marketing safety surveillance databases worldwide. To the best of our knowledge, this is the first study that utilized signal detection analysis of the FAERS database to identify signals of nephrotoxicity with natural products.
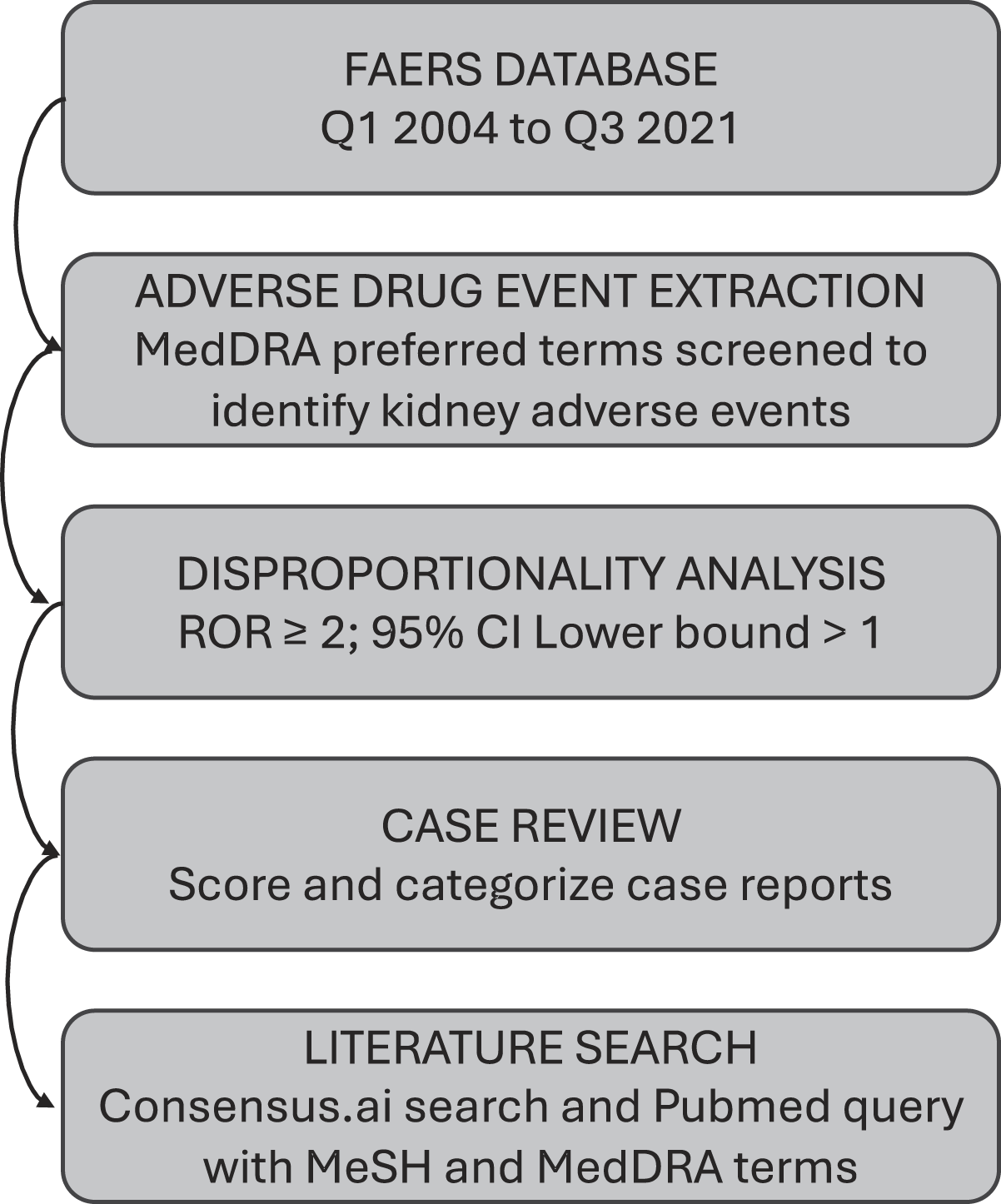
The flowchart of study.
Materials and Methods
A retrospective analysis was performed using the FAERS database from its public release (quarter 1, 2004, through quarter 3, 2021) to identify natural products with disproportionate reporting signals for nephrotoxicity. The FAERS database is a result of the MedWatch system, which contains records of spontaneous reports recorded by manufacturers, consumers, and health care professionals. Reporters list known medication histories and provide an assessment of primary or secondary culprit drugs. Curation strategies to overcome de-duplication, product misspellings, and mapping of ingredients and adverse events to harmonized codes were applied to the FAERS database prior to its use.16,17 The aggregate list of natural products was compiled using methods from a similar study by Li et al. 17 Queries were completed by using the Medical Dictionary for Regulatory Activities (MedDRA) terminology to identify reported kidney-related adverse events (Supplementary Table S1).
MedDRA preferred terms (PT) were used to screen and identify possible adverse events reported for natural products related to the kidney. These PTs used were AKI, fetal renal impairment, nephropathy toxic, prerenal failure, renal failure neonatal, blood creatinine increased, creatinine clearance decreased, creatinine urine decreased, glomerular filtration rate decreased, hypercreatininemia, kidney injury molecule-1, renal tubular injury, renal tubular necrosis, and protein urine present.18,19
According to the FDA definition, a signal is “information that arises from one or multiple sources (including observations and experiments) that suggests a new potentially causal association, or a new aspect of a known association, between an intervention and an event or set of related events, either adverse or beneficial.” 20 In the present study, a post-marketing surveillance, nephrotoxicity with events described with MedRA PT, was considered the signal of interest. The disproportionality analysis was employed to identify natural products with disproportionate reporting signals for events related to the kidney considered possibly nephrotoxic. 21 To achieve this goal, a reporting odds ratio (ROR) was calculated (Table 1). The ROR is a disproportionality measure used for signal detection in spontaneous reporting databases and compares the odds of reporting a specific adverse event for a given exposure to the odds of reporting the same event for all other exposures in the FAERS database. Signals with ROR ≥ 2 were determined to have an adequate intensity and were eligible for further analysis and reporting. 22 Signals with a ROR ≥ 2, a lower bound 95% confidence interval (95% CI) ROR ≥ 1, and at least two case reports were considered significant.23,24 Statistical analyses were performed using R (version R 4.3.2) and Microsoft Excel software (version 16, 2021).
Reporting Odds Ratio (ROR) Estimation

After completing the disproportionality process, the individual case reports identified in FAERS were reviewed for additional duplicate signals not initially captured with the automated process.16,17 Reports were manually reviewed and assessed by two pharmacists in a standardized fashion to determine if the natural product could be attributed to the adverse event. A straightforward scoring system based on the Naranjo criteria and embedded within a Qualtrics survey was utilized to evaluate the strength of individual reports. 25 Each case report was assigned a distinct score, which was then recorded in a spreadsheet and categorized as weak, moderate, or strong. The survey included questions regarding report completeness, the source of the interaction report, potential alternative causes, the adverse event, and the availability of supporting literature.
A literature search using “Does natural product ‘X’ lead to adverse event ‘Y’” was performed using Consensus.AI. Consensus includes a meter that indicates whether each abstract supports or does not support the proposed association, helping to quickly assess the relevance of each AE-NP pair. Articles returned from Consensus.AI were evaluated to determine if there was a supporting mechanism for the adverse event. In addition, we performed a targeted literature search in PubMed to identify and evaluate AE-NP pairs based on mechanism of action and history of case reports (Supplementary Table S2).
Results
There were a total of 290 distinct Latin binomial names of natural products, resulting in 924-character strings representing common names of natural products in the FAERS database. From this, a total of 231 signals (AE-NP pairs) associated with 63 natural products were identified. By considering an ROR equal to or more than two and at least two case-reports, there were three natural products identified from a total of 15 cases (Table 2).
General Characteristics of Kidney Safety Reports Related to Natural Products Identified from 15 Cases
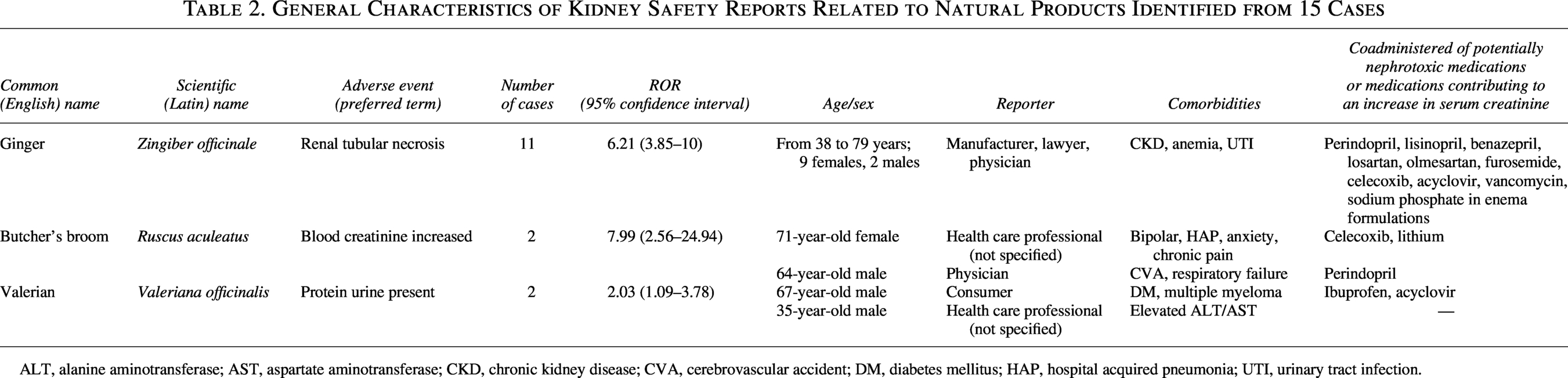
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CKD, chronic kidney disease; CVA, cerebrovascular accident; DM, diabetes mellitus; HAP, hospital acquired pneumonia; UTI, urinary tract infection.
Valerian (Valeriana officinalis)
Two cases of protein urine present in valerian recipients were found. Both were reported in 2005. The first case, reported by a consumer, was a 66-year-old male with plasma cell (multiple) myeloma and type 2 diabetes. A total of 67 medications were listed in his medication history. The primary suspects of protein urine present were zoledronic acid and pamindronate. The second case, reported by a physician, was a 35-year-old male with liver injury. There were five medications listed in his medication history. The primary and secondary culprit drugs were oxymetholone and methasterone, respectively. No data were reported about the purpose and duration of valerian treatment in these two cases.
Butcher’s broom (Ruscus aculeatus)
Two cases of blood creatinine increased in recipients of butcher’s broom were identified. The first one was reported by a health care professional in an unspecified country in 2004; it was about a 71-year-old female, a known case with psychiatric and rheumatologic diseases, hospitalized because of hypotension, loss of consciousness, prolonged QT, and sinus arrest. The patient received 13 concomitant medications, such as celecoxib and lithium. Nevertheless, propranolol was labeled as the primary culprit drug, while ciprofloxacin and tizanidine were considered as secondary suspects of the blood creatinine increased. The second case was reported by a physician in France in 2019 and described a 64-year-old male who died due to acute respiratory failure and a cerebrovascular accident. The medical history of the patient comprised 20 medications, with amiodarone was as the primary suspect cause of the blood creatinine increase.
Ginger (Zingiber officinale)
A total of 11 cases of renal tubular necrosis were found for individuals receiving ginger. Most cases (10 out of 11) described patients who underwent colonoscopies and received ginger-flavored bowel-stimulating agents, like sodium phosphate. The mean age of reported cases was 65.9 years. Common concomitant diseases in the cases included chronic kidney disease (CKD), anemia, and urinary tract infection. All subjects were also given at least one potentially nephrotoxic agent simultaneously.
Discussion
The KDIGO 2024 clinical practice guideline for the evaluation and management of CKD has made a clear recommendation to have health care providers review and limit the use of over-the-counter medicines, dietary supplements, and herbal remedies that may be harmful for people with CKD. 26 The rationale behind this recommendation is that these agents may either induce or accelerate kidney diseases. However, adherence to this recommendation is challenging given the ubiquitous lack of knowledge about the safety profiles for natural products, stressing the importance of pharmacovigilance for these supplements to ensure patient safety. In addition to the KDIGO 2024 guideline, the WHO also published guidelines on pharmacovigilance of herbal medicines, including nephrotoxicity. 27 Table 3 lists several herbal medicines associated with different types of nephrotoxicity reported in the literature. 1 In our evaluation, we identified 15 cases and 3 new safety signals that have not been discussed previously related to the kidney using the FAERS database.
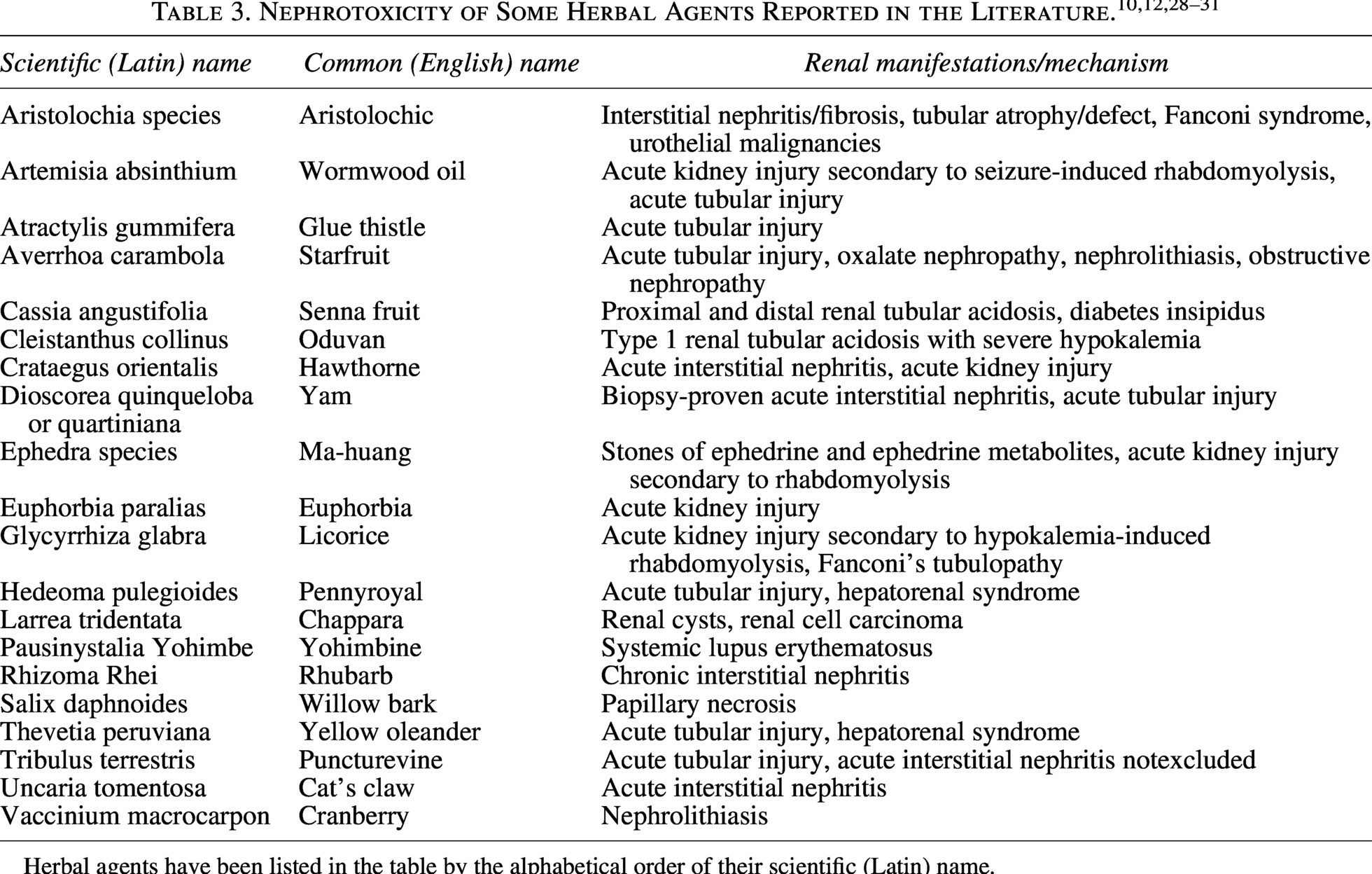
Herbal agents have been listed in the table by the alphabetical order of their scientific (Latin) name.
Patients and providers often assume that natural products are relatively safe and possibly effective. Pharmacodynamics and pharmacokinetics profiles of these agents may be unknown, and their potential toxicity, including nephrotoxicity, is unstudied. Rigorous testing and reporting adverse events through the FDA-approved process are required for all drugs that are approved in the United States, but not for natural products. In addition, information on the safety of natural products is poorly organized and not easily accessible or understandable to the public. Due to the importance of this issue, the KDIGO 2024 guideline for CKD has listed and grouped by continent common herbal remedies and dietary supplements with evidence of potential nephrotoxicity. 26 Still, this list is based on sparsely available data and needs continuous updates as new data becomes available. Notably, there were no overlapping natural products between our results and those currently included in the CKD guidelines.
Valeriana officinalis, as a member of the Caprifoliaceae family, is native to North America, Asia, and Europe. Its roots and rhizomes are typically used as a sedative/hypnotic in complementary and traditional medicine. 32 Valerian side effects are scarce and primarily limited to dizziness, drowsiness, and vivid dreams. Rarely, valerian recipients experience mild-to-moderate hepatotoxicity, usually in combination with other herbal agents. 33 In the context of kidney impairment, a crossover, double-blind, clinical trial indicated that valerian may significantly improve patients’ cognitive status with no significant changes in electroencephalography findings in patients receiving hemodialysis. 34 Moreover, an experimental study failed to show any protective effects of Valeriana wallichii against gentamicin nephrotoxicity in rabbits, despite its high flavonoid content. 35 Protein urine present identified in two cases in the present study may be at least partially attributed to coadministered medications, including bisphosphonates and anabolic-androgenic steroids. Both medication classes have been associated with different types of glomerular diseases like focal segmental glomerulosclerosis, manifested by proteinuria.6,36 Still, V. officinalis was identified as a signal in our study and requires awareness by clinicians until further investigation to understand its impact on the kidney.
Ruscus aculeatus, also known as butcher’s broom, is a member of the Asparagaceae family that is native to Europe. It is traditionally used to relieve the symptoms of discomfort and heaviness of legs related to minor venous circulatory disturbances. Besides varicose veins, hemorrhoids have been another indication of butcher’s broom in clinical practice. These therapeutic effects are attributed to the anti-inflammatory and antioxidant activities of the medicinal herb. 37 Common side effects of this natural product include nausea, vomiting, diarrhea, and gastritis. In the context of the kidney, Ruscogenin, an active compound in R. aculeatus, significantly reduced surrogate biomarkers involved in folic acid-induced AKI, suggesting nephroprotective activity.38,39 Blood creatinine increased in two cases presented here and may be partially attributed to this herbal agent since primary and secondary suspects, including propranolol, tizanidine, and amiodarone, are not prominent nephrotoxins. 21 One report indicated concomitant use of ciprofloxacin, which can be associated with acute interstitial nephritis and crystal nephropathy. 40 In the other report, the person was also taking celecoxib and lithium, both of which have known nephrotoxic potential compared with the primary and secondary suspected medications. 6
Ginger (Zingiber officinale) belongs to the Zingiberaceae family and is native to Southeast Asia. Ginger is a widely used natural product with a well-established efficacy and side effect profile. In addition to being consumed as a common dietary condiment (spice), its rhizomes have been mainly used to treat dysmenorrhea, osteoarthritis, motion sickness, and pregnancy-induced nausea/vomiting. 41 Ginger side effects are uncommon and include abdominal discomfort, heartburn, and irritation of the mouth and throat. 42 Z. officinale has protective effects against drug-induced nephrotoxicity like cisplatin, gentamicin, and doxorubicin via its antioxidant/anti-inflammatory activities in experimental studies.43–45 Ginger has also demonstrated protective effects on the kidney when given before renal ischemia. 46 There have been no published case reports suggesting Z. officinale is a nephrotoxic agent. Interestingly, in most reported cases with renal tubular necrosis in the present study, ginger was given as a flavoring agent in combination with bowel-stimulating agents like sodium phosphate. Acute phosphate nephropathy, following the administration of sodium phosphate enemas, has been rarely reported in patients with underlying renal insufficiency. Most of the reported cases belonged to individuals over 65 years of age. In addition, most of our cases also had CKD as an underlying disease. 47 Finally, all patients were given at least one potentially nephrotoxic medication (e.g., losartan, benazepril, celecoxib) simultaneously. Therefore, it seems unlikely that ginger per se is nephrotoxic, at least in cases reported here. Still, 11 reported cases do give reason for pause and suggest clinicians should monitor serum creatinine in older patients with CKD receiving sodium phosphate enemas.
Although the study explores a novel topic and utilizes the FAERS database, one of the largest pharmacovigilance repositories, it has several limitations. First, FAERS contains a large amount of valuable information about adverse drug events and signal detection; however, database is not representative of the entire population of events and is reliant on voluntary reporting. Since the database relies on voluntary reports from both health care providers and consumers, several biases and gaps in reporting may arise. Health care professionals may not be motivated or may not have enough time to report adverse drug events, especially if the events are not serious. Concerns about possible legal issues may be another cause of underreporting adverse events by health care professionals. In addition, patients may not recognize their signs/symptoms of kidney disease linked to a specific medication or supplement, leading to underreporting. Finally, a lack of reporting by patients about herbal product use is another potential source of underreporting and hinders the ability to identify signals in the FAERS database.
Second, our limited case reports cannot necessarily prove causal relationships between natural products and nephrotoxicity. The FDA form is simple, only requiring the patient identifier, event or problem, reporter information, and product information sections to be filled out. Consequently, the amount of provided information can vary significantly and be inadequate. A report being submitted may have several medications that have the potential to cause kidney injury with different possibility levels, making it harder to identify the true causative substance.7,48 Lack of temporal information makes this task especially difficult, as the adverse event could have occurred independent of administration of the causative agent.
Third, the PT used in this study based on the FAERS database seem to be mostly vague, inconclusive, and imprecise from the nephrology viewpoint. For example, “blood creatinine increased” identified in two cases of butcher’s broom, the amount and duration (chronicity) of serum creatinine increase are unknown. In cases reported here, we cannot definitively determine whether blood creatinine increases and even kidney failure is AKI, acute kidney disease, or CKD. This is also true for “protein urine present” reported in two cases of V. officinalis. It is unclear whether reported proteinuria cases are normal (less than 30 mg/day albumin in urine), microalbuminuria (30–300 mg/day albumin in urine), macroalbuminuria (300–3,000 mg/day albumin in urine), or nephrotic range (more than 3,000 mg/day albumin in urine). 43 In other words, MedDRA terms do not necessarily allow for differentiating laboratory abnormalities from clinically confirmed AKI and determining AKI severity. In addition, similar clinical events may be coded under multiple PT, which may lead to misclassification or underestimation of kidney events. Finally, the need for dialysis or long-term kidney outcomes in affected cases is unknown.
Conclusions
This pharmacovigilance disproportionality analysis based on the FAERS database identified three natural products, including ginger, butcher’s broom, and valerian, that had a significant signal for possible nephrotoxicity. It is interesting that there is some conflicting evidence in the literature suggesting ginger may be nephroprotective. This may be partially explained by the lack of causality assessments in FAERS including the presence of cofounders and alternative causes of nephrotoxicity like the coadministration of nephrotoxic agents. Regarding ginger cases, nephrotoxicity signals could be attributed to phosphate nephropathy caused by sodium phosphate present in enema formulations. Therefore, these reported cases of nephrotoxicity in FAERS require confirmatory evaluations and biological plausibility assessments. Nevertheless, these signals cannot be overlooked until more conclusive data are available given the limited data on the safety of natural products. Clinicians should be vigilant about monitoring kidney function in individuals taking butcher’s broom, valerian and older patients with CKD receiving ginger-flavored phosphate enemas.
Data Availability
The data that support the findings of this study are openly available in Food and Drug Administration Adverse Events Reporting System at https://www.fda.gov/drugs/fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-latest-quarterly-data-files.
AI Use Statement
Artificial intelligence (AI) was used solely to improve grammar, spelling, and clarity during article preparation. No AI tools were used to generate, analyze, or interpret data, nor to draw scientific conclusions.
Footnotes
Author Disclosure Statement
S.K.G.—Federal Grant Funding: National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK); Member, American Board of Internal Medicine Critical Care Specialty Board; Member, Board of Regents, American College of Clinical Pharmacy.
Funding Information
This work was supported by the
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.