
Abstract
Introduction:
Patients with breast cancer commonly experience anxiety and sleep disturbance during and after treatment, and these symptoms are closely interrelated, negatively affecting the quality of life. Mindfulness-based interventions (MBIs) have been increasingly used as a nonpharmacological supportive approach. This systematic review and meta-analysis aimed to evaluate the effects of MBIs on anxiety and sleep quality in patients with breast cancer.
Methods:
A systematic search of PubMed, Web of Science, Cochrane Library, CINAHL, and Embase was conducted up to May 15, 2025. Random-effects meta-analysis was used to estimate standardized mean differences (SMDs) with 95% confidence intervals (CIs). Risk of bias was assessed using the Cochrane RoB 2.0, and the certainty of evidence was evaluated with Grading of Recommendations, Assessment, Development, and Evaluation.
Results:
Twenty-four randomized controlled trials (RCTs) including 3,212 participants were analyzed. MBIs significantly reduced anxiety compared with control groups receiving usual care, no intervention, or wait-list conditions (SMD: −0.47, 95% CI: −0.62 to −0.32), whereas no significant effect was observed for sleep quality. Subgroup analysis indicated that intervention duration accounted for 55.5% of the heterogeneity in anxiety outcomes. All studies were rated as having some concerns regarding risk of bias, primarily due to self-reported outcomes and lack of blinding. Certainty of evidence was moderate for anxiety and low for sleep quality.
Discussion:
MBIs appear to be effective in reducing anxiety among patients with breast cancer; however, no significant effect was observed for sleep quality. All included studies were rated as having some concerns regarding risk of bias, and the limited reporting of adverse events represents a limitation of the evidence. In addition, substantial heterogeneity in sleep quality outcomes and the limited number of included RCTs restrict exploration of heterogeneity sources and limit generalizability. Further high-quality well-designed RCTs are needed to strengthen and confirm the evidence.
Introduction
Breast cancer is the most commonly diagnosed cancer in women, and continues to be the primary cause of cancer-related deaths worldwide.1,2 Despite a 1% annual increase in incidence rates, patient survival rates have significantly improved, and the clinical outcomes for patients with breast cancer have markedly increased in recent years.2,3 Furthermore, advances in diagnostic techniques and therapeutic interventions have played a significant role in reducing breast cancer–related mortality. 4 However, breast cancer remains a significant concern in public health, in part because patients frequently experience debilitating side effects from common therapeutic interventions, including surgery, chemotherapy, biological therapy and radiation therapy. 5 Throughout the prolonged treatment period, patients experience both physical and psychological burdens, which are commonly associated with emotional disturbances, such as anxiety, depressive symptoms, and other mental health problems.6,7 Anxiety is a frequent psychological reaction to a cancer diagnosis and represents a normal response to perceived threats such as loss of body function, changes in physical appearance, and fear of death. Anxiety often increases, particularly as the disease advances or treatment becomes more intensive. 8
Among these psychological symptoms, sleep disturbances are particularly prevalent, affecting approximately 50% of patients with breast cancer, 9 and are significantly more prevalent compared with the general population. 10 Insomnia in breast cancer survivors has been linked to various factors, including anxiety, depression, and fear of recurrence. 11 However, insomnia is often overlooked and inadequately managed, as it is perceived as a normal and transient reaction to cancer or its treatment, and is not adequately reported by patients. 12 Previous studies have shown that sleep problems are common in anxiety disorders and that there is a bidirectional relationship between insomnia and anxiety. 13 Moreover, many patients experience both anxiety and sleep disturbances, which can interfere with their overall adjustment to the disease. 8
These challenges have led to an increasing number of patients with breast cancer seeking complementary therapies, such as supportive care during cancer treatment. 3 Among the various nonpharmacological complementary and alternative medicine therapies, mindfulness-based interventions (MBIs) have emerged as one of the most widely used approaches. Based on Buddhist traditions and incorporating formal meditation as a main component, MBIs aim to help patients manage pain, illness, and stress, while serving as an adjunct to conventional medical treatments. 14 This intervention has shown promise as a clinical treatment for reducing multiple co-occurring symptoms in breast cancer survivors by alleviating stress and enhancing cognition through mindfulness training. 15 In addition, MBIs help patients modify maladaptive thought patterns and manage negative emotions. 16 Evidence supports MBIs as an effective intervention for reducing individual symptoms of mood disturbances, depression, and anxiety in breast cancer survivors. 15 However, individual studies have limitations in establishing scientific evidence.
Systematic reviews and meta-analyses synthesize and analyze existing research findings, providing strong empirical support for the use of MBIs in patients with breast cancer. Previous meta-analyses have examined the impact of MBIs on psychological problems in patients with breast cancer. However, some studies have included both randomized controlled trials (RCTs) and non-RCTs,17,18 whereas others have analyzed a limited number of studies, making it difficult to obtain reliable evidence.16,19 Furthermore, regarding sleep quality, previous meta-analyses have suggested the need for further research incorporating more high-quality studies, as no significant effect of MBIs has been found in patients with breast cancer.16,17
Given these limitations, the present study focuses on anxiety and sleep quality, two of the most prevalent and interrelated symptoms in breast cancer survivors. Specifically, a meta-analysis of RCTs was conducted to evaluate the overall effects of MBIs on these outcomes and to identify moderating factors that may account for variations in the effects of MBIs. The findings of this review provide scientific evidence supporting the application of MBIs to reduce anxiety and improve sleep quality among patients with breast cancer.
Methods
This study was conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions (version 6.5) 20 and followed the PRISMA guidelines for systematic reviews and meta-analyses. 21 This meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO) database under registration number CRD42025639696.
Eligibility criteria
The PICOS-SD framework (Population, Intervention, Comparison, Outcomes, and Study Design) was used to establish the inclusion and exclusion criteria. According to this framework, the selected studies needed to meet the following requirements: (1) Population (P): patients aged ≥18 years diagnosed with breast cancer; (2) Intervention (I): MBIs, defined as programs that included formal mindfulness practices (e.g., mindfulness meditation, body scan, mindful breathing, mindful movement), incorporated mindfulness as a core therapeutic component, and involved regular mindfulness training sessions delivered over multiple weeks. (3) Comparison (C): standard care, usual care (considered synonymous with routine care), no intervention, wait-list control; (4) Outcomes (O): anxiety and sleep quality; (5) Study design: RCTs, to ensure a high level of evidence and minimize the risk of bias.
We excluded the following studies: (1) studies involving male patients with breast cancer, patients with severe cognitive impairment or mental disorders, or those diagnosed with anxiety or insomnia who were undergoing treatment, because the effects of pharmacological treatment could confound the effects of MBIs; (2) studies in which MBIs were combined with other interventions in the experimental group, or studies that mentioned mindfulness without providing structured mindfulness training (e.g., single-session mindfulness breathing); (3) studies in which interventions were applied to the control group or studies that lacked a control group; (4) studies that did not evaluate anxiety or sleep quality; (5) studies that failed to provide the data necessary for meta-analysis; and (6) non-RCTs.
Data sources and search strategies
We searched five databases: PubMed, Web of Science, Cochrane Central Registry of Controlled Trials, CINAHL (Cumulative Index of Nursing and Allied Health Literature), and Embase. The search terms used were “breast cancer,” “cancer,” “mindfulness-based interventions,” “anxiety,” and “sleep quality.” The primary search terms included “breast cancer,” “mindfulness-based interventions,” “anxiety,” “sleep quality,” and “RCTs.” These terms were combined using Boolean operators (“AND” and “OR”) to create a comprehensive search strategy. In addition, Medical Subject Headings, entry terms, Embase Subject Headings (Emtree), and synonymous and free terms associated with these key terms were employed to optimize the search. Relevant studies were also identified through manual searching of websites and citation lists. The search was conducted from the inception of the databases until May 15, 2025, with no language restrictions applied. Detailed search strategies are provided in Supplementary Tables S1, S2, S3, S4, and S5. To ensure methodological rigor and minimize the risk of bias, only published peer-reviewed RCTs were included, and gray literature as well as clinical trial registries were not searched.
Study selection
EndNote 20 reference software (Clarivate Analytics, Philadelphia, PA) was used to import and manage the retrieved articles. Researchers (M.K., H.K., and Y.L.) independently screened the titles and abstracts of articles to identify potentially relevant studies. Subsequently, the full texts of the selected articles were reviewed separately by the same researchers to assess their eligibility based on the inclusion and exclusion criteria. Discrepancies that arose during this process were resolved through discussion and consensus building.
Data extraction
Data were extracted by a team of three reviewers (M.K., H.K., and Y.L.). In cases of disagreements, a discussion was held until a consensus was reached. The data extracted from the included studies comprised the following details: first author, publication year, country, stage of cancer, sample size, mean age, type of program, delivery method of the intervention, duration of the intervention, instruments, comparison groups, and adverse events. This comprehensive extraction ensured a detailed comparison of study characteristics and intervention features.
Risk of bias assessment
The three reviewers (M.K., H.K., and Y.L.) independently assessed the risk of bias in each study. Any discrepancies that arose during the evaluation process were addressed through discussions to reach a consensus. The risk of bias was assessed using the Cochrane Risk of Bias Tool 2.0 (RoB 2) for RCTs. 22 The evaluation covered five key domains: the randomization process, deviations from the intended interventions, missing outcome data, measurement of outcomes, and selection of reported results. Each of these domains was classified as “low risk,” “some concerns,” or “high risk.” The overall risk of bias for each study was determined based on the assessments across all five domains. In addition, the potential impact of high-risk domains on the study results was discussed, providing crucial information for evaluating the reliability of the study outcomes.
Certainty of evidence assessment
The certainty of evidence for each outcome was evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach. Two independent reviewers (MK and HK) assessed the evidence based on five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Any disagreements were resolved through discussion, and a third reviewer (YL) was consulted if necessary. Certainty was categorized as high, moderate, low, or very low using GRADEpro software.
Synthesis and statistical analysis
The meta-analysis was conducted using the meta package in R software (version 4.0.3; R Foundation for Statistical Computing, Vienna, Austria). For studies in which the same variable was measured at multiple time points, data closest to the end of the intervention were included in the analysis. To account for heterogeneity across studies in terms of measurement tools, intervention duration, and delivery methods, a random-effects model was applied. 23 Effect sizes were measured using different metrics across studies; therefore, standardized mean differences (SMDs) were calculated to compare effect sizes across studies. A random-effects model was used to estimate the mean effect, considering both within- and between-study variances in the analysis. Studies with smaller variances and higher precision were assigned greater weights than those with lower precision.
We assessed heterogeneity across studies using the I2 statistic, which quantifies the proportion of total variance in effect sizes attributable to true heterogeneity. I2 values of 0%–40% suggest that heterogeneity may not be important, 30%–60% indicate potentially moderate heterogeneity, 50%–90% suggest substantial heterogeneity, and 75%–100% reflect considerable heterogeneity. 20 Moderator analyses were conducted to investigate the sources in the presence of heterogeneity. For categorical moderators, a subgroup analysis was performed, and analysis of variance was applied when significant differences were found between the groups. Meta-regression analysis was used for continuous moderators.
Publication bias was first assessed using a funnel plot and then confirmed through Egger’s regression analysis, with a p-value less than 0.05 indicating the presence of publication bias. In addition, we assessed the robustness of the overall results through a leave-one-out sensitivity analysis, in which each study was excluded in turn, and the pooled effect size was reestimated.
Ethical approval
As the data used in this meta-analysis were extracted from primary studies that had already obtained ethical approval, and no raw participant data were involved, neither ethical approval nor patient consent was required.
Results
Study selection
Initially, 1280 articles were identified. After removing 363 duplicates, 971 articles were screened based on the titles and abstracts, resulting in the exclusion of 924 articles. Thus, 47 articles underwent full-text review, of which 25 were excluded for the following reasons: inappropriate participants (n = 4), inappropriate comparisons (n = 5), inappropriate outcomes (n = 5), inappropriate interventions (n = 1), protocol-only studies (n = 2), non-RCT studies (n = 4), and missing mean/standard deviation (SD) (n = 4). A total of 22 articles from five databases were included in the final analysis.
In addition, seven articles were identified through a manual search, but five articles were excluded for the following reasons: inappropriate intervention (n = 2), combined intervention (n = 2), and missing mean/SD (n = 1). Consequently, two articles from the manual search were included in the final analysis.
Therefore, the final sample used in the meta-analysis comprised 24 studies, 22 identified through the database search, and 2 identified through manual searching (Fig. 1).
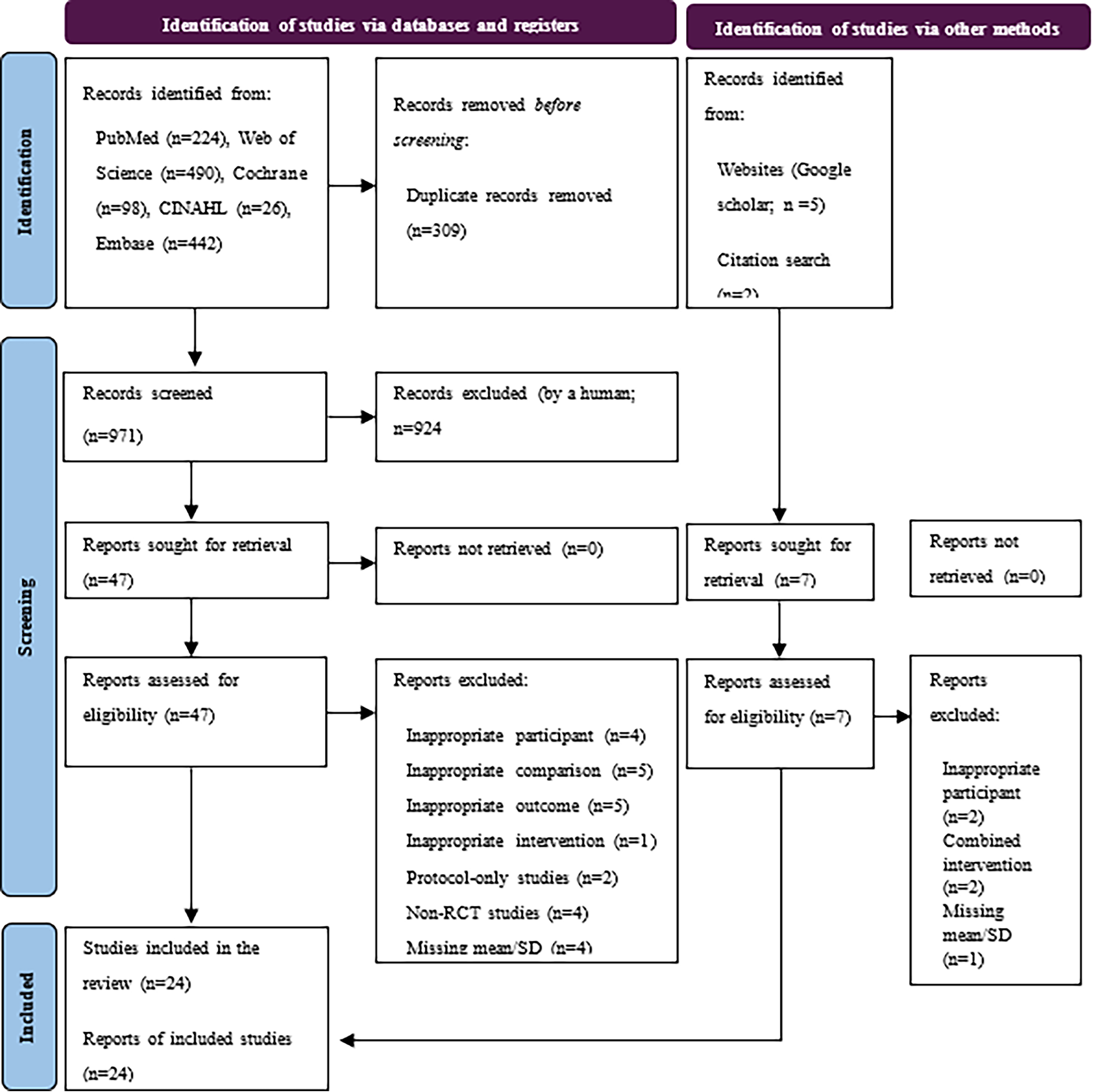
Flowchart summarizing the process of study selection.
Characteristics of the included studies
This systematic review and meta-analysis included 24 RCTs with a total of 3212 participants that met our inclusion criteria. All the studies were published between 2013 and 2024, of which 11 (45.8%) were published after 2020. Eight studies were conducted in the United States15,24–30 and eight in China7,31–37; two studies were conducted in Denmark38,39; three in Iran40,41; and one each in South Korea, 42 Japan, 43 and Sweden. 44
Most studies were conducted in hospital settings (n = 13). The most common cancer stages among participants were 0–III (n = 9). The sample sizes ranged from 12 to 165 participants in the experimental groups and 12 to 155 in the control groups. The mean age of participants varied from 42.35 to 57.2 years, with three studies not reporting the average age.
Regarding the type of intervention program, mindfulness-based stress reduction (MBSR) was the most common and was applied in 16 studies. The delivery method was predominantly in person (n = 20). The intervention duration ranged from 4 to 12 weeks, with 8-week programs being the most frequent (n = 10), followed by 6-week programs (n = 10).
In terms of measurement tools, the State–Trait Anxiety Inventory was the most commonly used tool to assess anxiety (n = 5), whereas the Pittsburgh Sleep Quality Index was widely used to measure sleep quality (n = 7). The most frequent comparators were usual care (n = 10), wait-list (n = 7), routine care (n = 5), no intervention (n = 1), and standard care (n = 1) (Table 1).
Characteristics of the Randomized Controlled Trial Studies (n = 24) in This Meta-Analysis
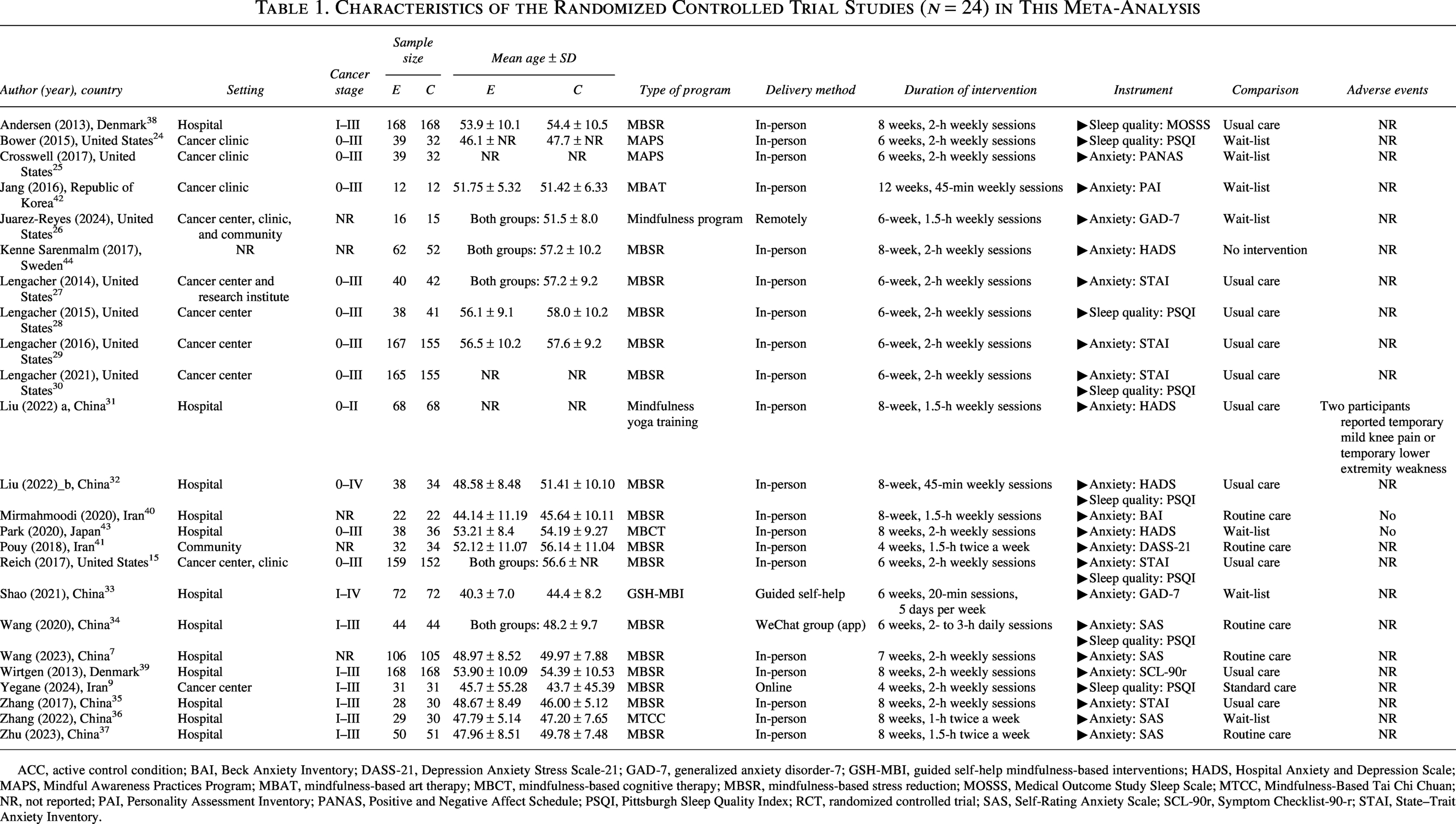
ACC, active control condition; BAI, Beck Anxiety Inventory; DASS-21, Depression Anxiety Stress Scale-21; GAD-7, generalized anxiety disorder-7; GSH-MBI, guided self-help mindfulness-based interventions; HADS, Hospital Anxiety and Depression Scale; MAPS, Mindful Awareness Practices Program; MBAT, mindfulness-based art therapy; MBCT, mindfulness-based cognitive therapy; MBSR, mindfulness-based stress reduction; MOSSS, Medical Outcome Study Sleep Scale; MTCC, Mindfulness-Based Tai Chi Chuan; NR, not reported; PAI, Personality Assessment Inventory; PANAS, Positive and Negative Affect Schedule; PSQI, Pittsburgh Sleep Quality Index; RCT, randomized controlled trial; SAS, Self-Rating Anxiety Scale; SCL-90r, Symptom Checklist-90-r; STAI, State–Trait Anxiety Inventory.
The majority of the studies (n = 21) did not report any adverse events. Two studies explicitly stated that no adverse events occurred, and one study reported mild, transient, practice-related adverse events in two participants (1.4% each), including temporary knee pain and temporary lower extremity weakness, both of which were resolved with simple measures.
Risk of bias
While all 24 studies were rated as having an overall risk of bias of “some concerns,” none were judged to be at “high risk.” In the domain of the randomization process, three studies were rated as “some concerns” due to insufficient information regarding the item “Was the allocation sequence concealed until participants were enrolled and assigned to interventions?” whereas the remaining 21 studies were rated as “low risk.” In the domain of deviations from intended interventions and missing outcome data, all studies were rated as “low risk.” In the outcome measurement domain, all 24 studies were rated as having “some concerns.” This was because, in all studies, the outcome assessors were aware of the interventions received by the participants, and outcomes were measured using self-reported questionnaires. Although these characteristics could potentially introduce measurement bias, the extent was not considered sufficiently severe to warrant classification as “high risk,” and therefore all studies were categorized as having “some concerns.” In the domain of selection of the reported result, all studies were rated as “low risk,” as the reported outcomes were consistent with those prespecified in the “Methods” section, and no evidence of selective outcome reporting was identified (Fig. 2).
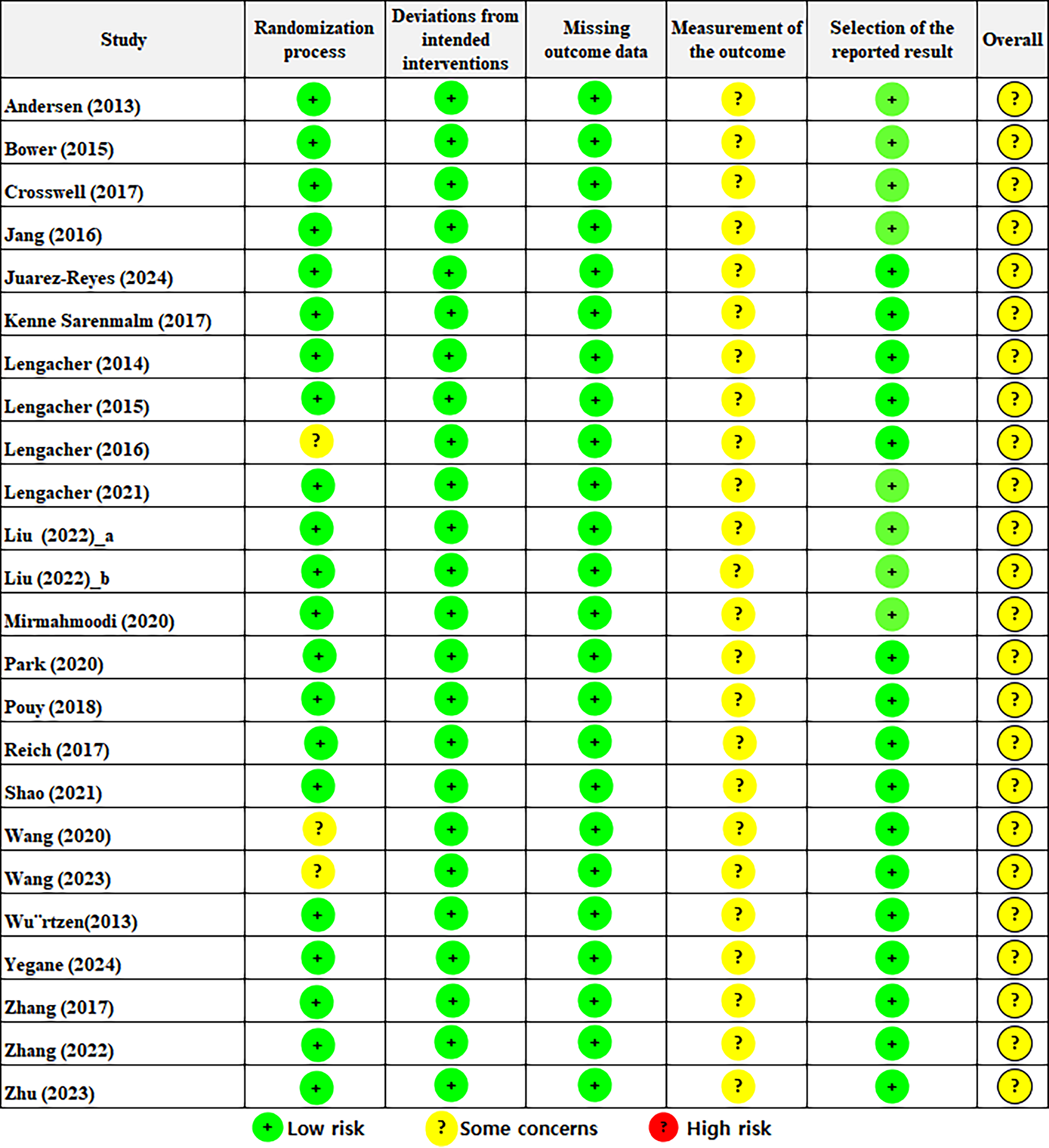
Risk-of-bias summary according to the revised Cochrane Risk-of-Bias 2.0 tool for randomized trials.
Effects of mindfulness-based interventions on anxiety among patients with breast cancer
The meta-analysis revealed that MBIs significantly improved anxiety (SMD: −0.47, 95% confidence interval [CI]: −0.62 to −0.32, p < 0.01) (Fig. 3). A negative value indicated a reduction in anxiety levels. This result was derived from 20 studies involving a total of 2,664 participants. In Figure 3, the width of the diamond represents the CI of the mean effect size, and the narrow CI observed in this study (95% CI: −0.62 to −0.32) suggests high accuracy and reliability of the results. The I2 value was 69%, indicating substantial heterogeneity.
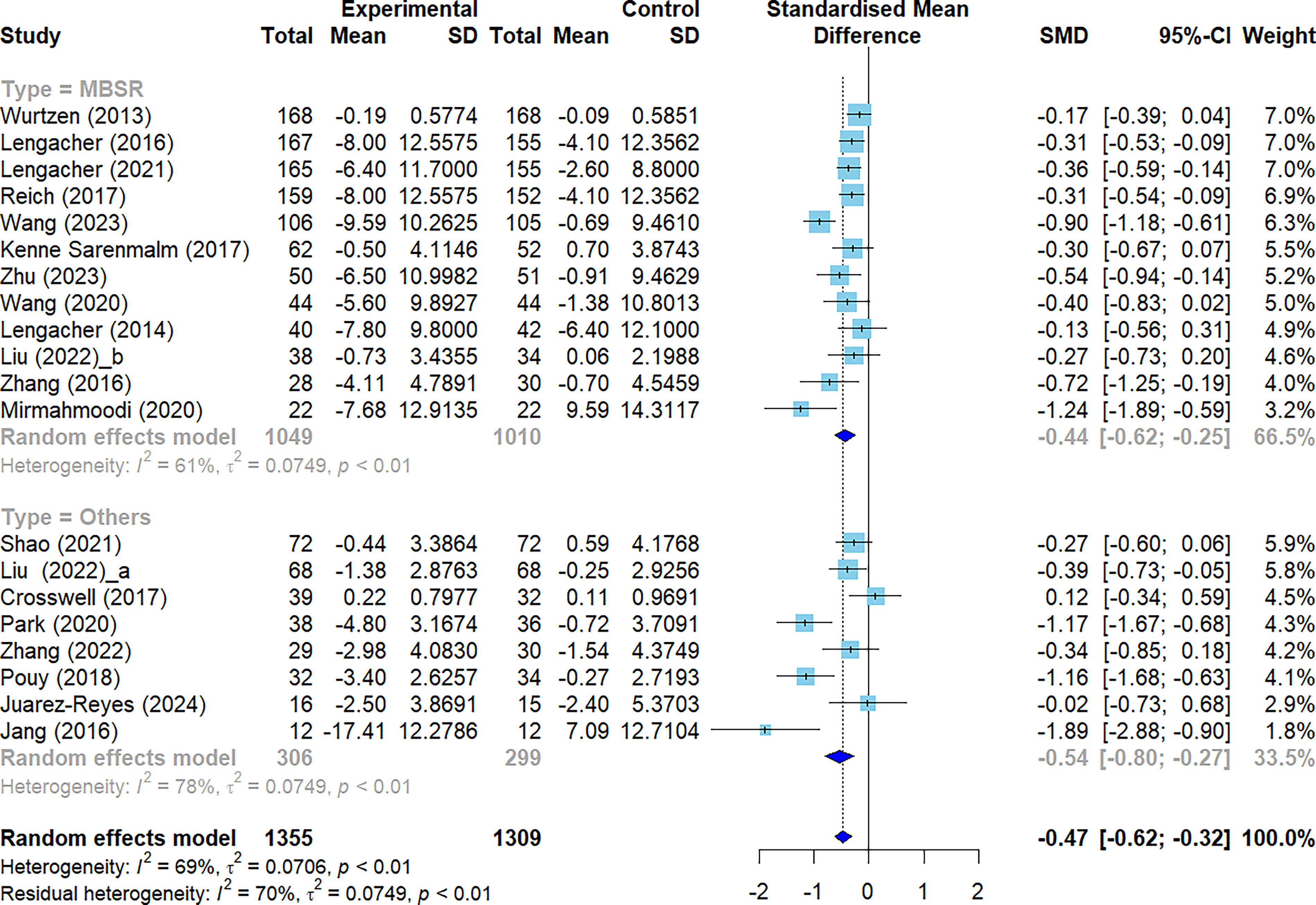
Forest plots: Effect of mindfulness-based interventions on anxiety in patients with breast cancer. CI, confidence interval; SD, standard deviation; SMD, standardized mean difference.
Effects of MBIs on sleep quality among patients with breast cancer
The meta-analysis revealed that MBIs had no significant effect on sleep quality in patients with breast cancer (SMD = −1.69, 95% CI = −3.48 to 0.10, p < 0.001). This result was derived from data from eight studies involving a total of 1339 participants with considerable heterogeneity (I2 = 98.9%) (Fig. 4).
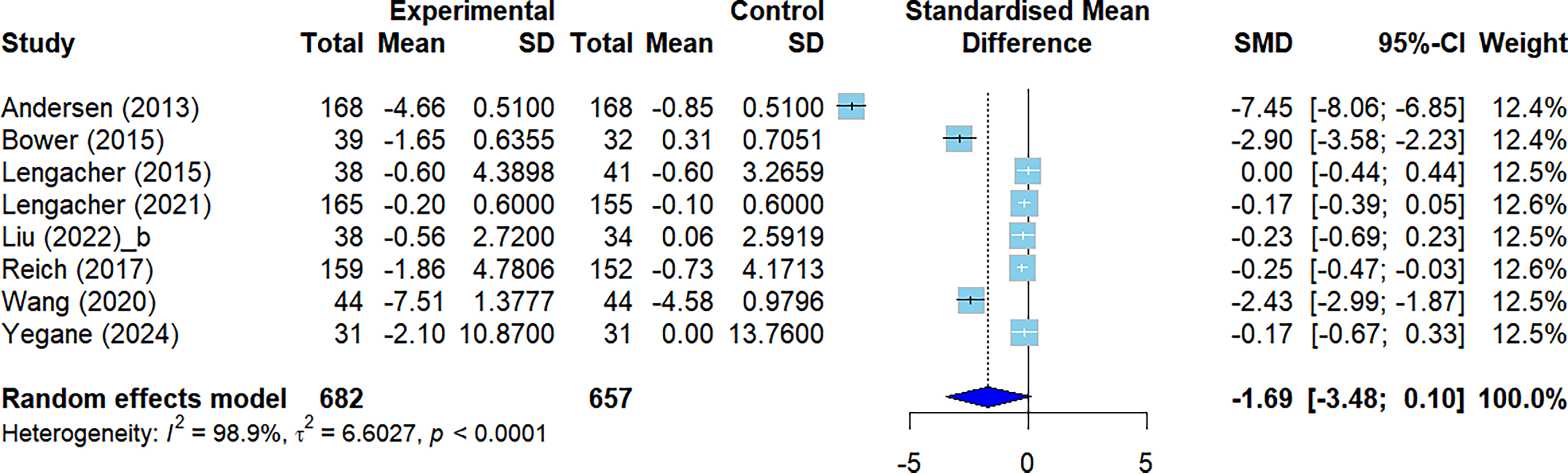
Forest plots: Effect of mindfulness-based interventions on sleep quality in patients with breast cancer.
Subgroup and moderator analyses
We observed substantial heterogeneity in anxiety (I2 = 69%) and explored the sources of this heterogeneity. In the analysis of categorical moderators, the type of program and delivery method did not influence the effect size; however, the duration of the intervention did have an effect. Specifically, the results from the 4-, 7-, and 12-week interventions were derived from a single study each, and thus were considered statistically unreliable. Both the 6-week and 8-week interventions showed significant effects, with the 8-week intervention (SMD = −0.47, 95% CI = −0.66 to −0.28) demonstrating a larger effect size compared with the 6-week intervention (SMD = −0.25, 95% CI = −0.43 to −0.07). Intervention duration accounted for 55.5% of the heterogeneity (Q moderator [QM] = 20.08, p < 0.001). The continuous moderators (age and sample size) did not significantly influence the overall effect size (Table 2).
Subgroup and Moderator Analysis
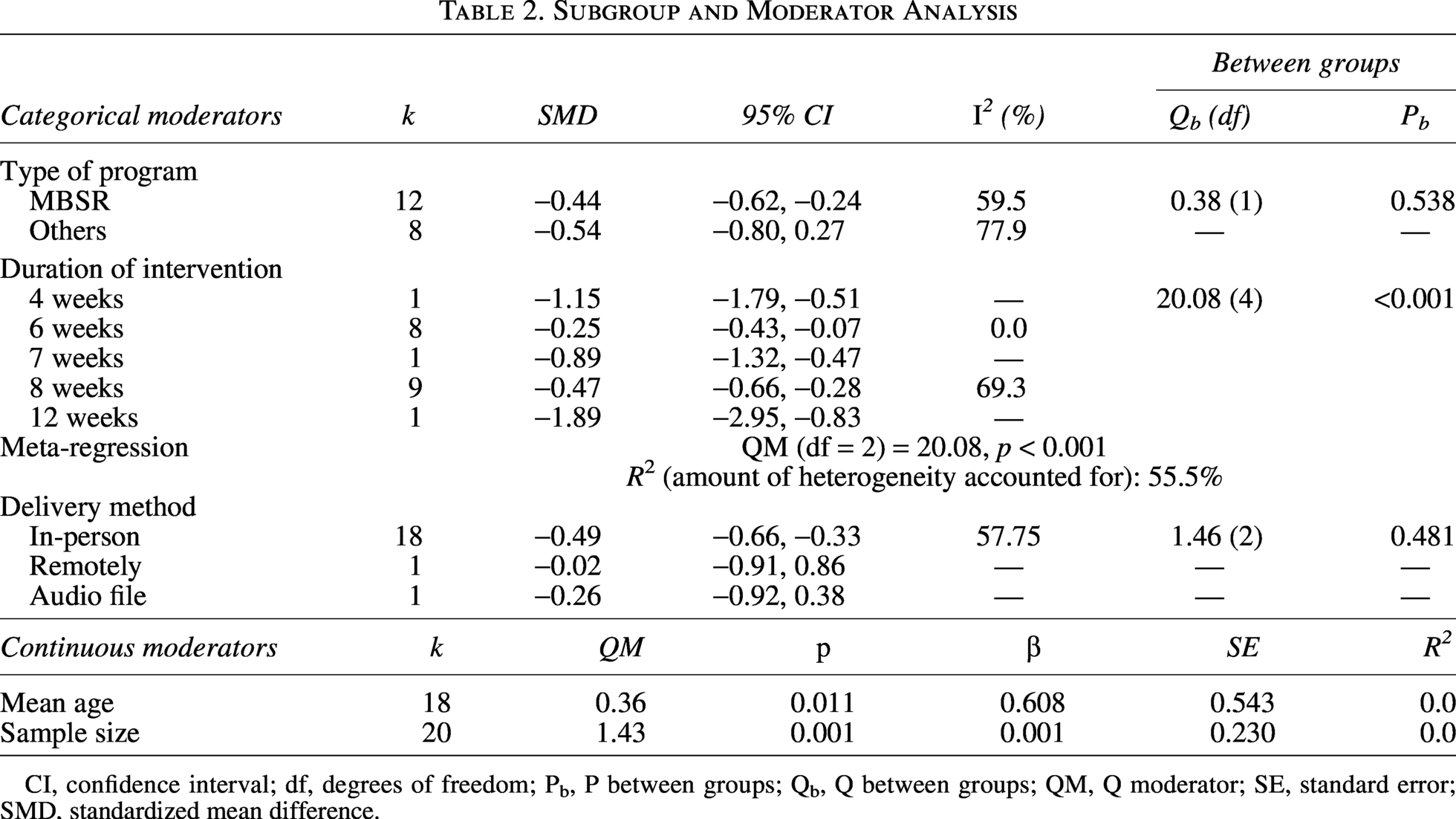
CI, confidence interval; df, degrees of freedom; Pb, P between groups; Qb, Q between groups; QM, Q moderator; SE, standard error; SMD, standardized mean difference.
Although there was considerable heterogeneity in sleep quality, a moderator analysis could not be conducted owing to the limited number of studies (n = 8), which resulted in insufficient statistical power.
Publication bias
Publication bias in the anxiety variable was assessed by analyzing the funnel plot, which displayed an empty space in the bottom-right corner, indicating possible asymmetry (Supplementary Fig. S1). Egger’s regression test was performed to statistically evaluate the presence of funnel plot asymmetry, and the results showed no strong evidence of publication bias (t = −1.91, df = 18, p = 0.072). Because of the limited number of studies on sleep quality, publication bias could not be assessed.
Sensitivity analysis
A sensitivity analysis was conducted by excluding each study individually and performing a meta-analysis of anxiety. The results showed that in all studies, the overall effect size was consistently within the 95% CI, thus demonstrating the reliability and robustness of the meta-analysis results (Supplementary Fig. S2). Sensitivity analysis for sleep quality could not be performed because of the insufficient number of included studies.
Certainty assessment using GRADE
The certainty of evidence for anxiety was evaluated using the GRADE approach. Regarding risk of bias, all included studies were rated as having some concerns, which contributed to downgrading the overall certainty of evidence. Other domains, including inconsistency, indirectness, and imprecision, were assessed as “not serious,” and no publication bias was detected. As a result, the overall certainty of the evidence for anxiety was rated as moderate.
In the assessment of the certainty of evidence for sleep quality, all studies were rated as having “some concerns” for risk of bias, which was therefore rated as serious. For inconsistency, heterogeneity was substantial, but because the number of included studies was small, the sources of heterogeneity could not be adequately explored, leading to a very serious rating. Indirectness and imprecision were not considered serious; however, due to the limited number of studies, publication bias was strongly suspected. Consequently, the overall certainty of the evidence for sleep quality was rated as low (Supplementary Table S6).
Discussion
Interpretation of results and comparison with previous studies
We conducted a meta-analysis of the effects of MBIs on anxiety and sleep quality in patients with breast cancer. Mindfulness involves self-regulation of attention and a state of consciousness characterized by nonjudgmental moment-to-moment awareness. 45 It emphasizes qualities such as patience, calmness, openness, trust, being nonstriving, letting go, and compassion.45,46 MBIs have been increasingly used to reduce psychological distress in patients during and after cancer treatment, 47 the most common being MBSR and mindfulness-based cognitive therapy (MBCT); various mindfulness-based programs have also been developed, and their effects have been increasingly explored. 46 Mindfulness encourages individuals to intentionally pay attention to present-moment experiences in an accepting and nonjudgmental manner. 17 These interventions have shown a positive impact on the common psychological difficulties in patients with breast cancer.
First, the results of the study showed that the overall effect size of MBIs on anxiety in patients with breast cancer was −0.47, indicating a significant improvement. Zhang et al. 17 in their meta-analysis on the effect of MBSR on anxiety in patients with breast cancer included both RCTs and non-RCTs, which may have increased the risk of selection bias and heterogeneity. In the study by Zainal et al., 48 the positive overall effect size of MBSR on anxiety in patients with breast cancer was 0.733. However, the effect size differed by study design, with 0.488 for only one RCT and 0.816 for non-RCTs, indicating a variation in the effect size depending on the research design. 48 A meta-analysis on the effects of MBSR 19 revealed the effect size of RCTs on anxiety as SMD = −0.5; however, only two studies were included in this meta-analysis. In a relatively recent meta-analysis, including both RCTs and non-RCTs, conducted by Chang et al., 49 the effect size of MBCT on patients’ anxiety was SMD = −0.70, showing a somewhat higher effect size. Notably, this study included and analyzed 20 RCTs encompassing both MBSR and MBCT, thereby enhancing the reliability of the effect size compared with previous studies that were based on only a small number of trials. Another previous study reported that the effect size of MBIs on anxiety varied depending on the intervention duration and type of control group. 50 Similarly, the subgroup analysis in this study showed a significant difference in effect size according to the duration of the intervention.
Our study also confirmed significant differences in the effect size of anxiety according to the intervention duration through a subgroup analysis. Both the 6- and 8-week interventions showed significant effects, with the 8-week intervention demonstrating a larger effect size compared with the 6-week intervention. In particular, the analysis of the 6- and 8-week interventions in this study included a larger number of studies, which may have reduced the likelihood of bias compared with previous studies.16,50 Regarding the differences in effect sizes according to the duration of interventions, it is important to consider the mechanisms of mindfulness. MBIs emphasize the enhancement of moment-to-moment, nonjudgmental, and nonreactive awareness of internal and external experiences. 51 This process helps individuals regulate their emotions in distressing situations, reduces rumination and overinterpretation of painful experiences, and ultimately alleviates negative emotions. However, it should be noted that this process also requires a certain amount of time to take effect. 51 Unlike the 6-week program, the 8-week mindfulness program includes a process that encourages patients to internalize the practices and develop associative patterns suited to their individual circumstances. Therefore, it can be emphasized that a certain amount of time is required for this process, from initial exposure to internalization for mindfulness to have a positive impact on individuals. 16 This calls for a more detailed investigation of the variation in effect sizes based on the duration of such interventions. Furthermore, the findings suggest the need for an analysis of how such interventions contribute not only to short-term improvements but also to the maintenance of long-term effects on negative psychological symptoms in patients with breast cancer.
Second, although individual studies have suggested that MBIs can reduce negative emotions, potentially leading to improved sleep quality,16,36,50 the effect of MBIs on the sleep quality of patients with breast cancer in this study was found to be nonsignificant. Similarly, in the meta-analysis by Zhang et al., 17 which included both RCT and non-RCT studies on the effect of MBSR on sleep quality in patients with breast cancer, the five studies analyzed showed considerable heterogeneity and did not demonstrate a significant effect compared to the control group. In contrast, a meta-analysis focusing exclusively on RCT studies found a significant effect size immediately after conducting MBSR in breast cancer patients, but this analysis included only three studies. 16 Thus, the limited number of studies included in meta-analyses restricts the ability to interpret the results fully. Sleep disturbance is one of the most common cancer-related symptoms experienced by cancer survivors, with approximately half of long-term cancer survivors reporting sleep problems. Sleep disturbances contribute to daytime functional impairment, fatigue, depression, and increased inflammation and negatively affect both quality of life and overall survival. 52 In particular, the prevalence of sleep disturbances in patients with breast cancer ranges from 0.14 to 0.93, indicating considerable variation. Since sleep disturbance has been identified as a significant risk factor for major depression, it requires appropriate management and intervention. 53 Therefore, future studies should conduct more rigorously designed large-scale experimental research to assess the effects of MBIs on sleep quality in patients with breast cancer. These studies should be integrated to reduce heterogeneity and produce more accurate and robust effect sizes.
Strengths and limitations
This study evaluated the overall effects of MBIs, including both MBSR and MBCT, on anxiety and sleep quality in patients with breast cancer, by including only RCTs conducted to date. The findings contribute to a higher level of scientific evidence. In addition, by including a larger number of studies and analyzing factors that may explain the variations in the effects of these interventions on anxiety, this study offers a more reliable foundation for understanding the effectiveness of MBIs, which can be considered a key strength of this review.
However, this study had some limitations that must be considered. First, although no specific language restrictions were applied, only studies published in English were included, which may have resulted in the exclusion of non-English-language studies. Future studies should include those published in various languages to provide a more comprehensive evaluation of the effects of MBIs on patients with breast cancer. Second, although subgroup analyses were conducted to identify the sources of heterogeneity, the small number of studies on certain variables limited a more detailed examination of these sources. Therefore, future research should include a greater number of high-quality studies with larger sample sizes to enable more comprehensive meta-analyses and better explore meaningful differences in effect sizes across various characteristics. Third, although no evidence of publication bias was found for anxiety, the possibility of publication bias due to gray literature cannot be completely ruled out. In addition, the inability to assess publication bias for sleep quality remains a limitation of this study. Fourth, the certainty of evidence was rated as moderate for anxiety and low for sleep quality, indicating that the results should be interpreted with caution. Last, the inclusion of studies with small sample sizes in this meta-analysis may have reduced the precision of effect size estimates and lowered the confidence in the conclusions drawn from the results. Future research should involve large-scale, long-term studies on this topic toward more robust results.
Conclusions
This systematic review and meta-analysis of 24 RCTs demonstrated that MBIs significantly reduced anxiety in patients with breast cancer, whereas no significant effect was observed for sleep quality. All included studies had some concerns regarding risk of bias, mainly due to self-reported outcomes and lack of blinding. The certainty of evidence was rated as moderate for anxiety and low for sleep quality. In addition, most studies did not assess safety; two studies reported no adverse events, and only one study reported minor and transient adverse events. Overall, due to limited or absent safety reporting, the safety of MBIs cannot be determined from the current evidence. Future research should focus on well-designed, large-scale trials with rigorous outcome assessment and systematic reporting of adverse events to provide more robust evidence, particularly regarding sleep outcomes.
Authors’ Contributions
Y.L. and H.K.: Data selection and extraction, methodology, quality assessment, writing—original draft, writing—review and editing, and supervision. M.K.: Conceptualization, data selection and extraction, statistical analysis, methodology, quality assessment, visualization, writing—original draft, and writing—review and editing. All the authors have read and approved the final version of this article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.