
Abstract
Background:
Caregivers of patients receiving palliative care frequently experience high levels of stress and anxiety, which may negatively affect their quality of life.
Objectives:
This study aimed to investigate the effects of mandala coloring on perceived stress, anxiety, and quality of life (primary outcomes) among caregivers of patients receiving palliative care.
Methods:
This cluster randomized controlled trial included 80 caregivers, allocated to an intervention group (n = 40) or a control group (n = 40). The intervention group participated in mandala coloring sessions 4 days per week for 4 weeks (16 sessions total), while the control group received no intervention. Data were collected using the Perceived Stress Scale (PSS), State Anxiety Scale, and Short Form-36 (SF-36) Health Survey. Postintervention outcomes were analyzed using analysis of covariance, controlling for baseline scores. The study was conducted and reported according to CONSORT cluster extension guidelines.
Results:
After adjustment for baseline scores, the intervention group showed significantly lower PSS (F = 133.29, p < 0.001, ηp2 = 0.634) and state anxiety scores (F = 38.57, p < 0.001, ηp2 = 0.334) compared with the control group. Postintervention SF-36 physical (F = 86.31, p < 0.001, ηp2 = 0.529) and mental health scores (F = 112.05, p < 0.001, ηp2 = 0.593) were significantly higher in the intervention group. In the control group, perceived stress and anxiety increased significantly, and quality of life scores decreased over the study period (p < 0.05). No adverse events, discomfort, or intervention-related withdrawals occurred, indicating that the intervention was safe and well-tolerated.
Conclusion:
Mandala coloring effectively reduced perceived stress and anxiety and improved the quality of life in caregivers of palliative care patients. Given its noninvasive, low-cost, and safe nature, it may be recommended as a supportive nurse-led intervention in palliative care settings.
Relevance to Clinical Practice:
Mandala coloring can be integrated into routine palliative care as a nurse-led nonpharmacological intervention to support caregiver well-being.
Introduction
Palliative care is defined by the World Health Organization (WHO) as a holistic approach that aims to improve the quality of life of patients with terminal illnesses and their families through the prevention and relief of suffering by early identification, assessment, and management of physical, psychosocial, and spiritual problems. 1 Caregivers play a crucial role in this process. They are responsible for monitoring symptoms, ensuring comfort, providing emotional support, coordinating care, maintaining patient safety, and arranging the care environment.2,3 However, fulfilling these responsibilities can be challenging and emotionally exhausting. Studies have shown that caregivers often experience stress, anxiety, and psychological burden due to the intensity of care and the emotional pain associated with witnessing their loved ones’ decline or anticipating their loss.4,5 The caregiving process, which is typically long and demanding, can lead to fatigue, helplessness, and social isolation, negatively affecting caregivers’ quality of life.6,7 Therefore, reducing stress and anxiety is essential to protect the physical and psychosocial well-being of caregivers and to improve the quality of care provided. 8
Nursing is described as the art of caring, which approaches patients and caregivers from a holistic perspective. This definition highlights that nursing is not limited to medical interventions but also involves empathy, human connection, and creative approaches that promote healing and enhance quality of life. 9 Caring as an art includes expressive and therapeutic activities that enable individuals to externalize emotions and achieve psychological balance. Within this context, art therapy is considered an artistic and therapeutic form of caring that allows individuals to express complex and painful emotions symbolically, providing relaxation and emotional relief.10–12
Among art therapy techniques, mandala coloring has attracted growing attention for its meditative and relaxing qualities. Unlike free drawing, which is spontaneous and unstructured, mandala coloring involves working within circular and symmetrical patterns that symbolize balance and wholeness. 13 The repetitive, structured activity promotes focus, mindfulness, and emotional regulation by transforming internal tension into creative expression. Through these mechanisms, mandala coloring helps individuals transfer emotions and thoughts into visual form, reduce anxiety, and restore inner calm. Research supports that art therapy, and particularly mandala coloring, effectively alleviates stress and anxiety and enhances well-being across different populations.13–16
Although several studies have examined the use of mandala coloring in various patient and caregiver populations,16–18 evidence regarding its effects among caregivers of palliative care patients remains limited. Given the limited evidence regarding the effects of mandala coloring among caregivers of palliative care patients, the main goal of this study was to examine the effect of mandala coloring on perceived stress, anxiety levels, and quality of life in caregivers of patients receiving palliative care.
Research Hypotheses
Mandala coloring has no effect on perceived stress, anxiety levels, or quality of life among caregivers of palliative care patients.
Mandala coloring significantly reduces perceived stress among caregivers of palliative care patients.
Mandala coloring significantly reduces anxiety levels among caregivers of palliative care patients.
Mandala coloring significantly improves the quality of life among caregivers of palliative care patients.
Methods
Study design
The present study was conducted using a cluster randomized experimental design with a pretest-posttest control group.
Participants and setting
The study population consisted of caregivers of patients hospitalized in the palliative care units of Fethi Sekin City Hospital between May and November 2023. Caregivers who met the inclusion criteria and agreed to participate were randomly selected from this population.
Inclusion and exclusion criteria
Inclusion criteria.
Being 18 years of age or older, Having adequate vision, hearing, and communication abilities, Providing care to a palliative patient for at least three months, Voluntarily agreeing to participate.
Exclusion criteria:
Paid or professional caregivers, Individuals with vision or hearing impairments, Those allergic to colored pencils or felt-tip pens.
Sample size calculation
The sample size was determined using G*Power version 3.1.9.4. Based on the independent samples t-test results reported by Koo et al. (2020), the effect size was 0.674, considering the comparison of State Anxiety Scale (SAS) mean scores (34.8 ± 11.8 vs. 28.3 ± 6.8). 19 Using this effect size, with a significance level of 0.05, 20 and a statistical power of 0.80, 21 the required minimum sample size was calculated as 72 participants (36 per group). To account for multiple testing across six primary outcomes, a Bonferroni-adjusted significance level (p < 0.0083) was considered. This more stringent significance threshold would require a larger sample size to maintain adequate statistical power. However, due to recruitment limitations during the study period, including difficulty in reaching eligible caregivers and time constraints, the study was completed with a total of 80 participants (40 per group).
A post-hoc power analysis was conducted to evaluate the achieved statistical power given the final sample size.
Randomization
The study was conducted in four palliative care wards (wards 1–4) in the hospital. Prior to participant recruitment, an independent researcher randomly assigned the wards to intervention or control groups using a lottery method: wards 2 and 3 were assigned to the intervention group, and wards 1 and 4 to the control group. All caregivers meeting the inclusion criteria in each ward during the study period were invited to participate. Allocation of wards was concealed from participants and clinical staff to prevent selection bias. Ward-level cluster randomization was chosen for pragmatic reasons, to prevent contamination between participants within the same ward and to facilitate implementation of the intervention. The randomization process and study conduct adhered to CONSORT 2025 guidelines and the CONSORT extension for cluster randomized trials (Fig. 1).
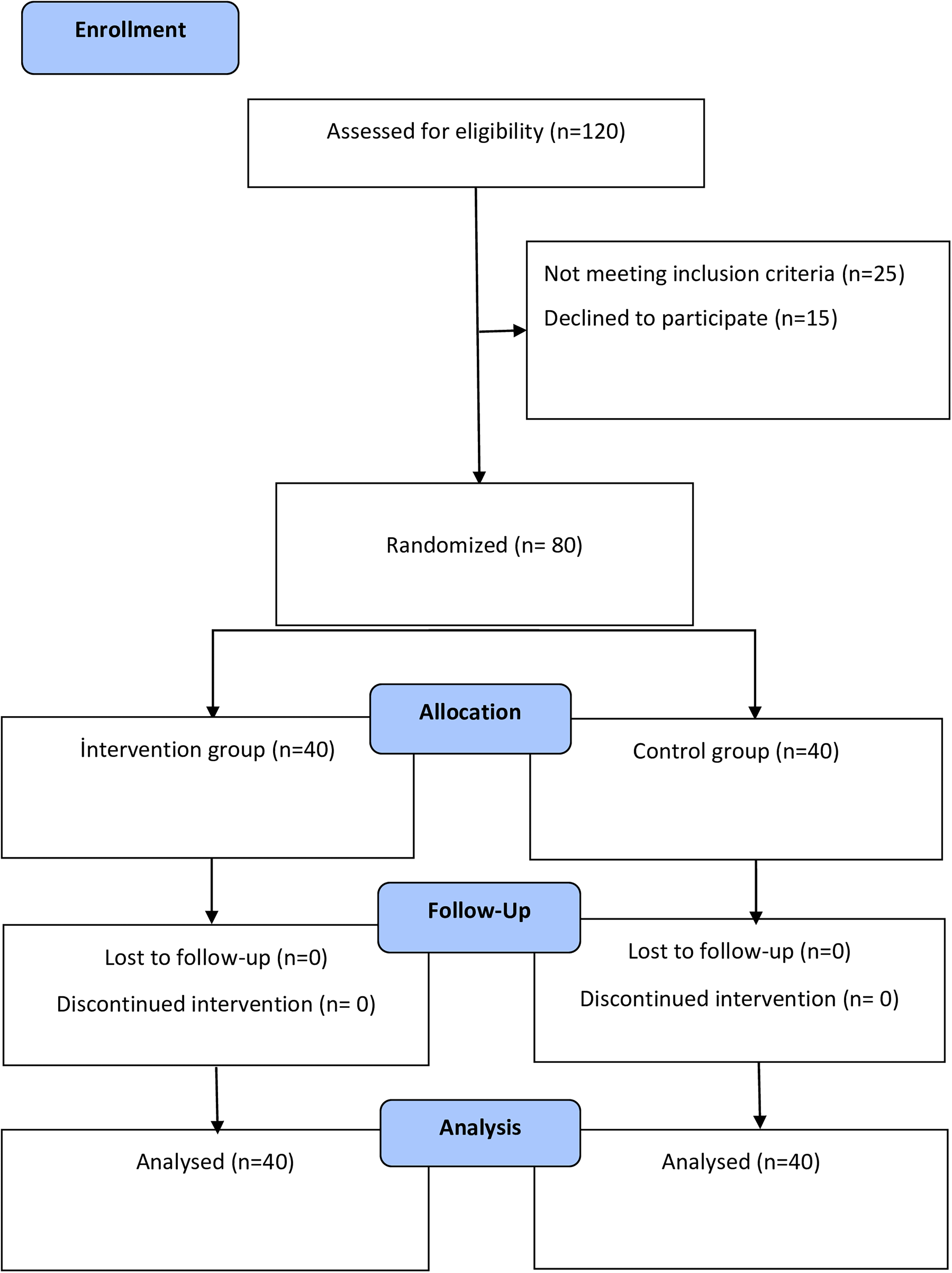
CONSORT Flow Diagram.

Examples of Mandala Coloring. Figure 2 presents examples of the mandala templates used during the intervention. These images are illustrative and were not obtained as study results.
Blinding
Due to the nature of the intervention, caregivers and clinical staff could not be blinded to group allocation. However, statistical analyses were conducted by an independent statistician who was blinded to the group assignments, ensuring unbiased outcome assessment.
Measurements
Data were collected using an Introductory Information Form and validated, self-reported instruments: the Perceived Stress Scale (PSS) for perceived stress, the State Anxiety Scale (SAS) for anxiety, and the Short Form-36 (SF-36) Health Survey for quality of life.
Introductory information form
There are a total of 16 questions in this form, including 12 questions about the identifying characteristics of the caregiver (gender, educational status, marital status, income status and how long they have been caring for the patient) and 4 questions about the identifying characteristics of the patient (age, gender, diagnosis and duration of diagnosis).
Perceived stress scale
The PSS was designed by Cohen, Kamarck and Mermelste to measure the degree individuals perceived certain situations in their lives as stressful, and Cronbach’s alpha coefficient was 0.86. 22 Bilge, Öğce, Genç and Oran adapted the scale into Turkish and found Cronbach’s alpha value to be 0.81 in the reliability study. 23 The scale has been designed to measure the extent to which individuals perceive their experiences as stressful, including their feelings and thoughts that they may have experienced during the last month. The items in the PSS are scored between “0: Never and 4: Very Often” and it is a five-point Likert-type 8-item scale. Maximum possible score from the scale is 32. High scores from the scales indicate that the perceived stress level is high and the individual has coping problems. Cronbach Alpha value of the present study was 0.91.
State anxiety scale (SAS)
Spielberger et al. developed The State Anxiety Scale. 24 Öner and Le Compte conducted the validity and reliability study in Turkey and found Cronbach’s alpha value to be between 0.94 and 0.96. 25 In this study, the 20-item “State Anxiety Scale” (SAS) was used to evaluate state-related anxiety. State Anxiety Scale was developed to express how individuals feel when they are under a certain situation and condition. The 4-point Likert-type 20 item scale is scored between “1: Not at all and 4: Completely”. Possible score from the scale is between 20 and 80. Higher scores indicate higher levels of anxiety. 25 In this study, Cronbach alpha value was 0.95.
SF-36 health survey
The scale was developed by Ware. 26 Koçyiğit et al. adapted the scale into Turkish to be used in clinical practice and research. 27 It was adapted to Turkish and Cronbach’s alpha value was calculated as 0.93. 27 The scale, which includes 36 items, consists of 2 main dimensions (physical dimension and mental dimension) and is in 2-point, 3-point, 5-point and 6-point Likert type.26,27 The subscales assess health on a 0–100 point scale, with 0 representing “poor health” and 100 representing “good health”.28,29 Cronbach’s alpha value was found to be between 0.88 and 0.90 in the present study.
Implementation
Before the intervention, both the intervention and control group caregivers were informed verbally and in writing about the study. The Introductory Information Form, PSS, State Anxiety Scale (SAS), and SF-36 Quality of Life Scale were administered as pretests to both groups. These instruments were selected because they are widely used, reliable, and valid tools for measuring stress, anxiety, and quality of life among caregivers.
Mandala coloring was chosen as the art therapy method because it is simple, non-invasive, and suitable for individuals without artistic skills. Its structured and symmetrical form promotes mindfulness and emotional regulation, helping to reduce stress and anxiety.13,30
Caregivers in the control group did not receive any intervention during the study period.
Caregivers in the intervention group participated in mandala coloring sessions using 16 pre-selected mandala templates (Fig. 2 here). Each session was carried out at the patient’s bedside in the palliative care room, allowing caregivers to stay close to their patients while completing the coloring activity. A new printed mandala drawing on A4 paper and a set of 12 colored felt-tip pens were provided before each session. Caregivers colored the mandalas on their own without supervision, and the researcher collected the drawings after each session.
The literature shows that the duration and frequency of mandala coloring interventions are not standardized and vary between 4 and 16 weeks.15–18,30–32 Based on this evidence, in the present study, mandala coloring was implemented four days per week (Monday, Wednesday, Friday, Sunday) for four consecutive weeks. Each session lasted 1 hour between 16:00 and 17:00, scheduled so as not to interfere with patient treatments or physician rounds.
The same questionnaires (PSS, SAS, and SF-36) were re-administered to both groups immediately after the four-week intervention as posttests.
Safety assessment
Safety was assessed through active monitoring during the intervention period. At each session, participants were asked whether they experienced any discomfort, emotional distress, fatigue, or any other adverse effects potentially related to the intervention. In addition, the researcher observed participants during sessions for any visible signs of distress, disengagement, or discomfort. Any reported or observed adverse events were to be recorded.
Evaluation of data
Data were analyzed using SPSS version 27.0. Normality of the scale scores was assessed using skewness and kurtosis values (±2), Kolmogorov–Smirnov and Shapiro–Wilk tests, and histogram inspections. The distributions were considered approximately normal. The internal consistency of the scales was evaluated using Cronbach’s alpha coefficients. Descriptive characteristics of the participants were summarized using frequencies and percentages, while means and standard deviations were calculated for continuous variables. Although statistical comparisons of baseline characteristics are reported, such tests are generally not required in randomized studies because randomization aims to balance groups. Baseline characteristics are presented for descriptive purposes, and in our study, with 40 participants per group, these tests were included to provide additional reassurance about group comparability. Chi-square tests were used to examine the homogeneity of the intervention and control groups with respect to descriptive characteristics. Given the experimental pretest–posttest design of the study, analyses of covariance (ANCOVA) were conducted to compare post-implementation outcomes between the intervention and control groups. Pre-implementation scores were entered as covariates to control for baseline differences between groups. ANCOVA assumptions were evaluated prior to analysis. Although the PSS includes multiple subscales, separate ANCOVA models were performed for each subscale (perceived stress, perceived coping, and total score), as each represents a distinct construct. Adjusted post-implementation mean scores, F values, p values, and partial eta squared (ηp2) were reported. A p value < .05 was considered statistically significant. To control for Type I error due to multiple testing of the six primary outcomes, a Bonferroni correction was applied, and the significance level was set at p < .0083 for these analyses.
Ethical considerations
Before starting the study, approval (23.03.2023 dated and 2023/05–08 numbered) was obtained from Ethics Committee of Fırat University Non-Interventional Research and an official permission letter was obtained from the hospital. Helsinki Declaration of Human Rights was adhered to during the study. Clinical trial registration was done (ClinicalTrials.gov ID: NCT05847231).
Results
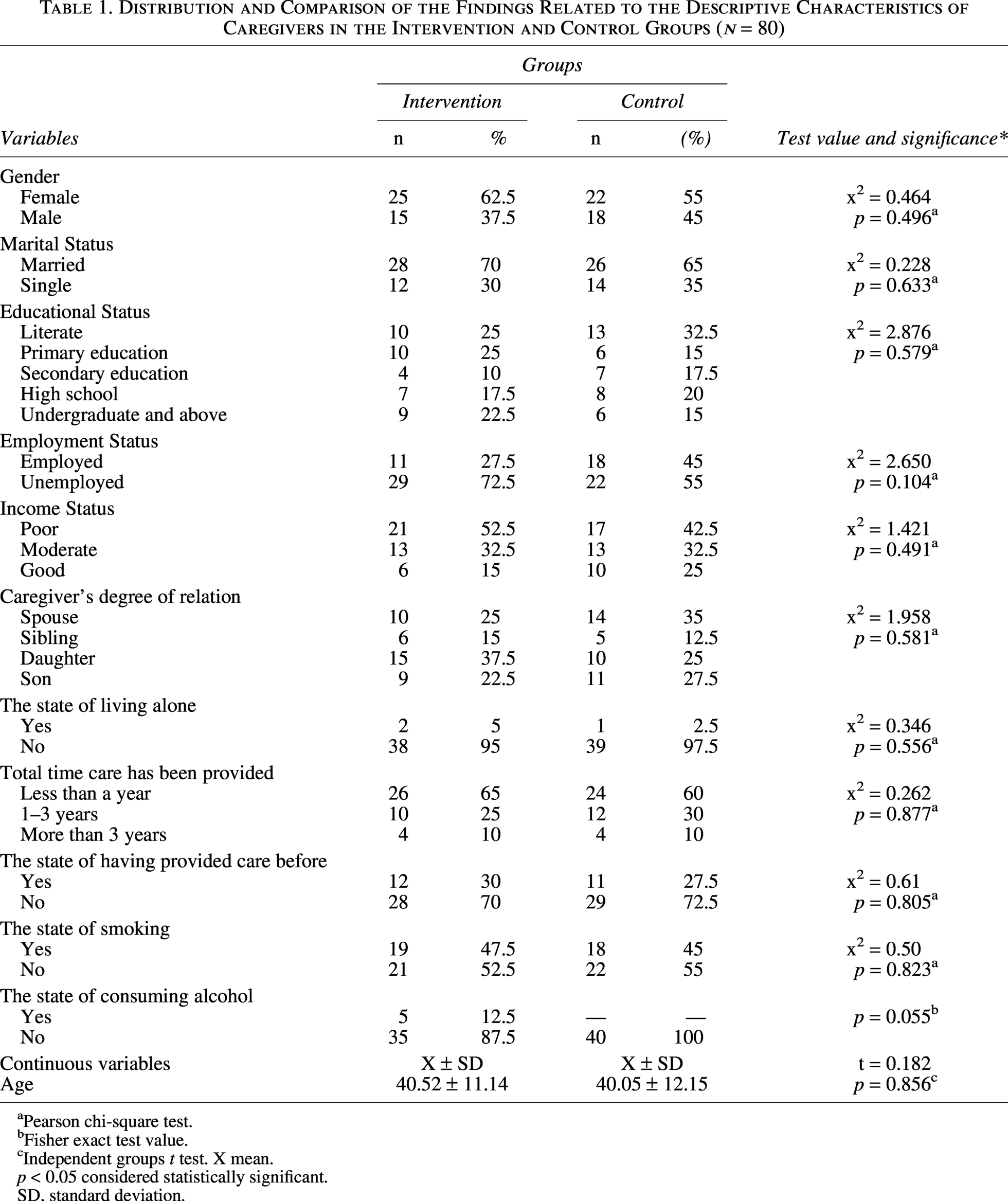
During the study period, 120 caregivers were reached. After excluding those who did not meet the eligibility criteria (n = 25) and those who declined participation (n = 15), a total of 80 caregivers completed the study—40 in the intervention group and 40 in the control group (Fig. 1). All participants were family members who provided unpaid care to palliative patients; no professional caregivers were included. The socio-demographic characteristics of caregivers in both groups are presented in Table 1. The two groups were found to be homogeneous in terms of gender, age, marital status, education, employment, income level, and caregiving experience (p > 0.05).
Distribution and Comparison of the Findings Related to the Descriptive Characteristics of Caregivers in the Intervention and Control Groups (n = 80)
Pearson chi-square test.
Fisher exact test value.
Independent groups t test. X mean.
p < 0.05 considered statistically significant.
SD, standard deviation.
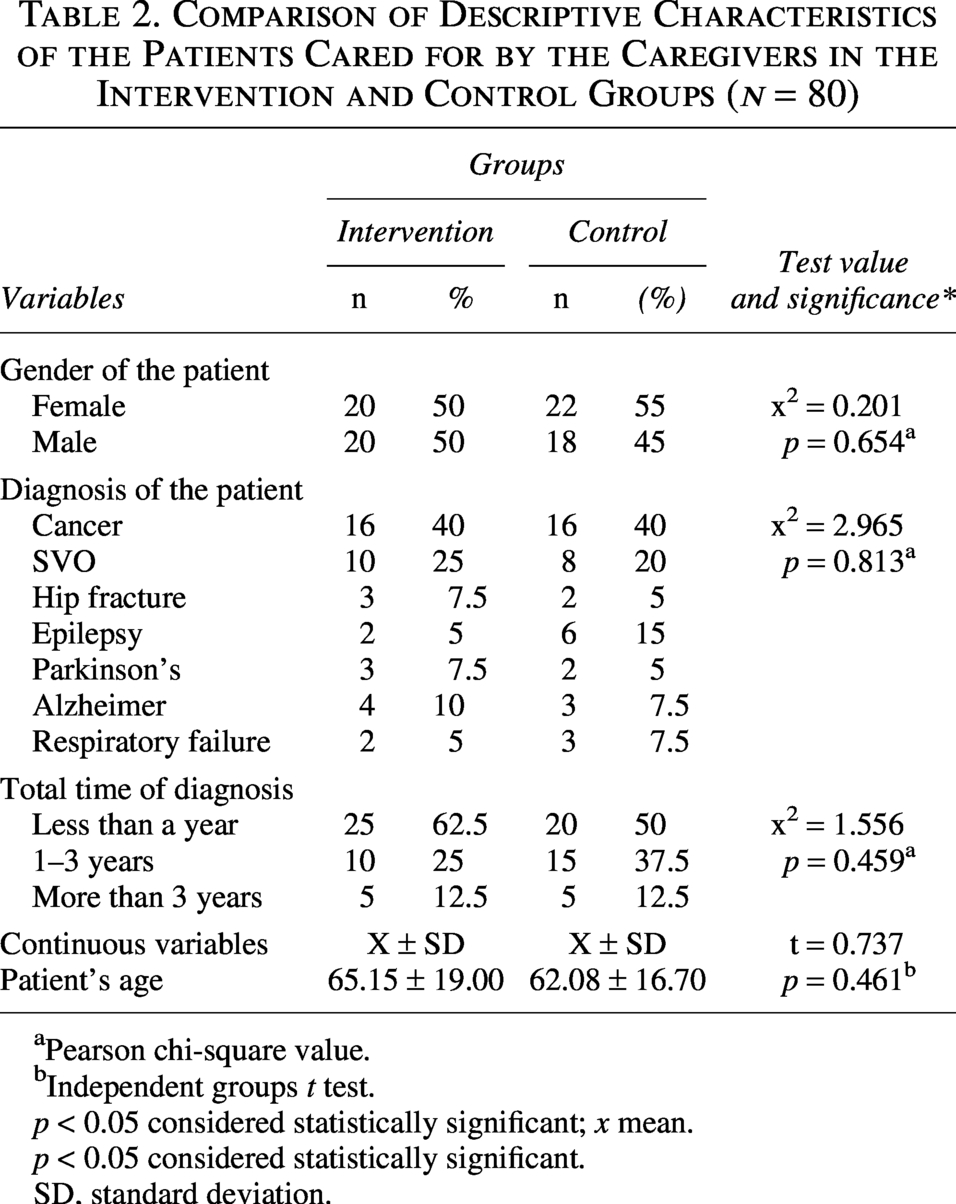
Characteristics of the patients cared for by the participating caregivers are shown in Table 2. Patients were not participants in the study; their data are presented only to describe the care context. The two groups were also homogeneous in terms of patient gender, diagnosis, and disease duration (p > 0.05).
Comparison of Descriptive Characteristics of the Patients Cared for by the Caregivers in the Intervention and Control Groups (n = 80)
Pearson chi-square value.
Independent groups t test.
p < 0.05 considered statistically significant; x mean.
p < 0.05 considered statistically significant.
SD, standard deviation.
As shown in Table 3, separate ANCOVAs revealed statistically significant group differences in all subscales of the PSS after controlling for pre-implementation scores. Even after applying the Bonferroni correction for multiple testing (adjusted significance level p < .0083), A significant group effect was observed for perceived stress (F[1,77] = 88.71, p < 0.001, ηp2 = .535), perceived coping (F[1,77] = 93.07, p < 0.001, ηp2 = .547), and total PSS scores (F(1,77) = 133.30, p < 0.001, ηp2 = .634). The adjusted post-implementation mean score for perceived stress was lower in the intervention group (Madj = 11.52, SE = 0.40) than in the control group (Madj = 16.85, SE = 0.40). Similarly, the adjusted post-implementation perceived coping score was lower in the intervention group (Madj = 6.14, SE = 0.24) compared with the control group (Madj = 9.45, SE = 0.24). The adjusted post-implementation total PSS score was also lower in the intervention group (Madj = 17.69, SE = 0.52) than in the control group (Madj = 26.27, SE = 0.52).
ANCOVA Results for Perceived Stress Scale and Subscales
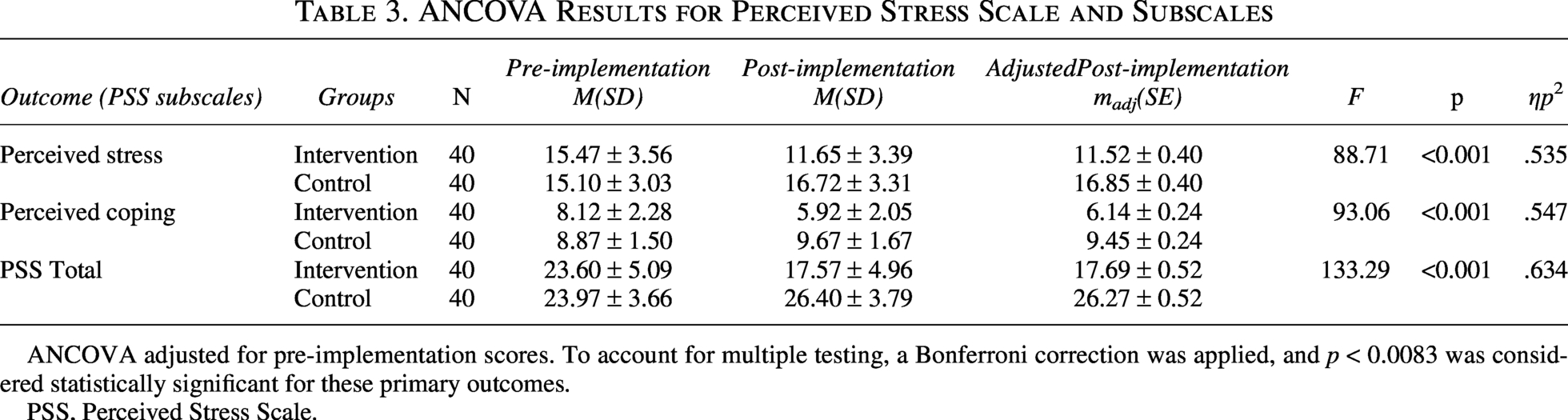
ANCOVA adjusted for pre-implementation scores. To account for multiple testing, a Bonferroni correction was applied, and p < 0.0083 was considered statistically significant for these primary outcomes.
PSS, Perceived Stress Scale.
As shown in Table 4, an analysis of covariance (ANCOVA) was conducted to examine differences in SAS scores between the intervention and control groups while controlling for pre-implementation anxiety levels. After adjusting for baseline scores, a statistically significant difference was observed between the groups in post-implementation SAS scores (F[1,77] = 38.57, p < 0.001, ηp2 = .334; which remains significant below the Bonferroni-adjusted alpha of 0.0083). The adjusted post-implementation mean score was lower in the intervention group (Madj = 47.25, SE = 1.30) than in the control group (Madj = 58.74, SE = 1.30).
ANCOVA Results for State Anxiety Scale

To account for multiple testing, a Bonferroni correction was applied, and p < 0.0083 was considered statistically significant for these primary outcomes.
As shown in Table 5, after controlling for baseline scores, ANCOVA demonstrated a statistically significant difference between the intervention and control groups in the SF-36 Physical Health dimension (F = 86.31, p < 0.001, partial η2 = .529; which remains significant below the Bonferroni-adjusted threshold of 0.0083). The adjusted post-intervention mean score was higher in the intervention group (Madj = 63.24, SE = 1.58) than in the control group (Madj = 42.29, SE = 1.58), indicating a large effect size. Similarly, as presented in Table 5, a significant group difference was found for the SF-36 Mental Health dimension after adjustment for pre-intervention scores (F = 112.05, p < 0.001, partial η2 = .593; significant at the adjusted p < 0.0083 level). The intervention group had a significantly higher adjusted postintervention mean score (Madj = 52.37, SE = 1.52) compared with the control group (Madj = 29.40, SE = 1.52), reflecting a large effect.
ANCOVA Results for SF-36 Health Survey Dimensions

To account for multiple testing, a Bonferroni correction was applied, and p < 0.0083 was considered statistically significant for these primary outcomes.
No adverse events or intervention-related discomfort were reported or observed during the study period. The mandala coloring intervention was found to be safe and well-tolerated by all caregivers in the intervention group. Given the non-invasive and low-risk nature of the intervention, no standardized adverse event assessment tool was required
A post-hoc power analysis indicated that the achieved statistical power was greater than 99% under the Bonferroni-adjusted significance level (p < 0.0083), based on the observed effect sizes (partial η2 = 0.334–0.634).
Discussion
This study examined the effects of mandala coloring on perceived stress, anxiety, and quality of life in caregivers of palliative care patients. The results suggest that mandala coloring may help reduce stress and anxiety while improving quality of life, indicating its potential as a supportive intervention in this setting.
The study showed a significant reduction in perceived stress among caregivers in the intervention group. This result is consistent with the stress-relieving effects of mandala coloring and other art therapy approaches reported in research conducted with different populations, such as oncology patients, dementia patients, nurses, adolescents, and individuals experiencing pandemic-related stress.15,17,33,34 These studies collectively indicate that structured creative activities help individuals manage emotional distress in demanding care environments.
Several mechanisms may explain the stress-reducing effect of mandala coloring. The symmetrical and repetitive structure of mandalas promotes attentional focus, facilitates cognitive organization, and induces a meditative state. This process reduces rumination, enhances mindfulness, and supports emotional regulation.30,35 Through coloring, caregivers can externalize distress, transform internal tension into symbolic visual form, and access a sense of calm and control. Therefore, the present findings support the use of mandala coloring as a practical and low-cost tool that nurses can integrate into routine care to alleviate caregiver stress.
The study also found a significant decrease in anxiety levels among caregivers after the intervention. Caregivers often experience high anxiety due to uncertainty, anticipatory and the inability to predict disease progression. 36 Similar to our results, research among students, patients with cancer, prisoners, and individuals undergoing stressful circumstances has consistently shown that coloring or drawing activities reduce anxiety by promoting psychological relaxation and supporting adaptive emotional processing.37–40
In addition to psychological mechanisms, neurophysiological explanations have been proposed. Creative engagement increases dopamine release, which contributes to a reduction in anxiety and enhances feelings of pleasure and relaxation. 36 By focusing attention on shapes and colors, individuals temporarily disengage from intrusive thoughts and worries, enabling an experience of mental harmony and emotional balance. 41 The present findings thus reinforce the evidence that art-based interventions can be used to support anxiety management in caregivers who are exposed to emotional strain in palliative contexts.
This study revealed that mandala coloring significantly increased caregivers’ quality of life. The literature consistently notes that palliative caregivers often experience a decline in quality of life because they prioritize patient needs over their own physical, emotional, and social well-being.32,42 International studies examining art therapy interventions—such as drawing, painting, theater activities, and creative expression—have shown improvements in emotional well-being, communication skills, social connection, and overall life satisfaction across different age groups and settings.33,43,44
Mandala coloring may enhance quality of life by providing caregivers with moments of personal time, enjoyment, and positive engagement outside their caregiving routine. This mechanism aligns with previous studies showing that creative and art-based activities improve emotional well-being, promote psychological comfort, and strengthen coping capacity by offering individuals a restorative break from caregiving demands.33,43,44 The findings of the present study, therefore, extend existing evidence by demonstrating that even short and low-intensity creative interventions can contribute meaningfully to the well-being of palliative caregivers.
While mandala coloring is only one form of art-based intervention, its effects are comparable to other approaches such as free drawing, painting therapy, and creative expression programs. Studies suggest that both structured and unstructured visual arts interventions reduce stress and anxiety. 39 However, mandala coloring may offer additional advantages due to its inherent geometric symmetry, which facilitates cognitive focus and reduces the cognitive load typically associated with free drawing. This structured nature makes mandala coloring a particularly accessible and manageable option for caregivers who may have limited time and mental energy.
Limitations
The study has several limitations. All outcome measures were self-reported using validated instruments, which may introduce response bias. The sample size was small, and participants were recruited from a single center, limiting generalizability. Future research should include larger and more diverse populations and assess long-term effects to confirm the intervention’s effectiveness and guide best practices for caregiver support in palliative care settings. Although cluster randomization was used, post-intervention outcomes were analyzed at the individual level using ANCOVA due to the small number of clusters (four wards), which may not fully account for cluster-level dependencies. Future studies should use mixed models or multilevel analyses to properly account for clustering. Another limitation is that the safety assessment was based on self-report and observation rather than standardized tools.
Conclusions
Mandala coloring may reduce perceived stress and anxiety and may improve quality of life among caregivers of palliative care patients. The intervention was noninvasive and well-tolerated. Due to the small number of clusters, these findings should be interpreted cautiously. Future studies with larger numbers of clusters are needed to confirm these results and to further investigate the intervention’s effectiveness in diverse palliative care settings.
Authors’ Contributions
G.B.: Conceptualization, methodology, investigation, writing—original draft, writing—review and editing. Supervision. F.K.: Conceptualization investigation, writing—original draft, writing.
Footnotes
Acknowledgment
This article is derived from the master’s thesis entitled “The Effects of Mandala Coloring on Perceived Stress, Anxiety Level and Quality of Life In Caregivers Providing Care to Palliative Care Patients: A Randomized Controlled Study,” conducted at the Institute of Health Sciences, Fırat University. In addition, it was accepted in the scientific research project unit of Fırat University with the project number SYO.23.01.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Author Disclosure Statement
The authors have no conflict of interest to disclose.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.