
Abstract

Introduction
Today the acupuncture profession in the United States is simultaneously more widely accepted and more endangered than ever before. Patient demand is increasing,1,2 as are insurance coverage, scientific evidence, and integration into major health care systems. Yet the workforce is shrinking, with fewer acupuncture schools and students, fewer practitioners, and new federal legislation that could decimate the acupuncture workforce within a decade unless successful action is taken. This commentary summarizes the main institutional approaches being taken to date and proposes a new one.
Declining Acupuncture Workforce
Licensed Acupuncturist numbers in the United States peaked at nearly 38,000 in 2018, and have since declined approximately 10%. 3 Student enrollment in acupuncture schools has fallen by roughly 25% since 2013, from approximately 8,000 to 6,000. 4 The number of accredited institutions has dropped 27% since 2015, from 62 schools to 44. 3
This is not simply weak programs failing: some that closed were among the oldest and most respected in the field. Enrollment is declining all across United States higher education, with lower birth rates during the 2008 financial crisis 5 compounding broader socioeconomic changes; health care labor shortages are widespread. 6 Other forces driving acupuncture school destabilization and workforce shrinkage are interrelated. A 3- or 4-year master’s or doctoral program often results in six-figure student loan debt. Some 80% of graduates then face the challenge of solo entrepreneurship: salaried positions remain a minority. The pandemic also caused significant workforce decline as acupuncturists closed their practices. 3
Increased Acupuncture Acceptance and Integration
Even as the workforce shrinks, acupuncture itself has gained widespread recognition and integration into mainstream health care. This reflects increased evidence demonstrating efficacy, effectiveness, and mechanistic understanding and also acupuncture’s adoption by the U.S.’s largest health care system, the Veterans’ Health Administration (VHA). Acupuncture research publications grew at a rate more than double that of biomedicine, from 1995 to 2014, 7 and continue to increase.
Acupuncture’s mainstreaming is evident in fertility care, as well as oncology, pain, and rehabilitation medicine, where most salaried positions for licensed acupuncturists exist within health systems. In 2025 the NIH launched a research initiative on whole person health, aiming towards an understanding of healthy physiological function that integrates body systems, 8 congruent with East Asian medicine (EAM)’s multi-system models for illness and salutogenesis. EAM and its diagnostic patterns were also represented in the 2019 World Heath Organization (WHO) International Classification of Diseases, version ICD-11. 9 In 2020, the WHO released benchmarks for “basic” and “advanced” training in acupuncture, each with modifications for conventionally trained health care providers.
Increased evidence and demand have led to (limited) private insurance coverage for acupuncture.10,11 Medicare also added acupuncture coverage for chronic lower back pain in 2020.12,13 However, licensed acupuncturists must be supervised by a medical doctor (MD) or other prescribing provider and cannot be directly reimbursed by Medicare; they are less likely to be reimbursed, and at lower rates, than others with less acupuncture training. 14
Success at a Cost
Medicare reimbursement vividly illustrates the current paradox. As acupuncture has moved into health care systems, the profession has added doctoral programs, standardized degree titles, and added curriculum on evidence- and systems-based practice often exceeding physical therapist (PT) and physicians’ assistant programs. However, acupuncture reimbursement rates remain generally low, which has stifled job creation and dampened student enrollment.
With increasing patient demand and scientific evidence and more available reimbursement for Western medical professionals, it is not surprising that many states have added acupuncture needles to the practice scope of MDs, nurses, and allied health professions, including PTs, dentists, chiropractors, occupational therapists, athletic trainers, and naturopaths. 15 These certification programs are typically 300 or fewer hours. 16 The term “dry needling” 17 is often used to describe the practice of needling without reference to EAM theory, though dry needling is a form of acupuncture. 18
The Current Crisis
In this context (see Fig. 1, The Acupuncture Education Pipeline Crisis: a Systems Map), two provisions of the ‘One Big Beautiful Bill Act’ (P.L. 119-21), 19 are set to begin July 1st, 2026. The Reimagining and Improving Student Education (RISE) Committee will limit total federal student loans for acupuncture and other graduate programs to $100,000. More problematic is The Accountability in Higher Education and Access through Demand-driven Workforce Pell (AHEAD) Committee, which requires that programs be evaluated by comparing 4-year average annual postgraduate earnings (from 2021 forward) against those of bachelor’s-prepared graduates (approximately $60,000 nationally). An estimated 98% of complementary and integrative health educational institutions will fail this metric. 20
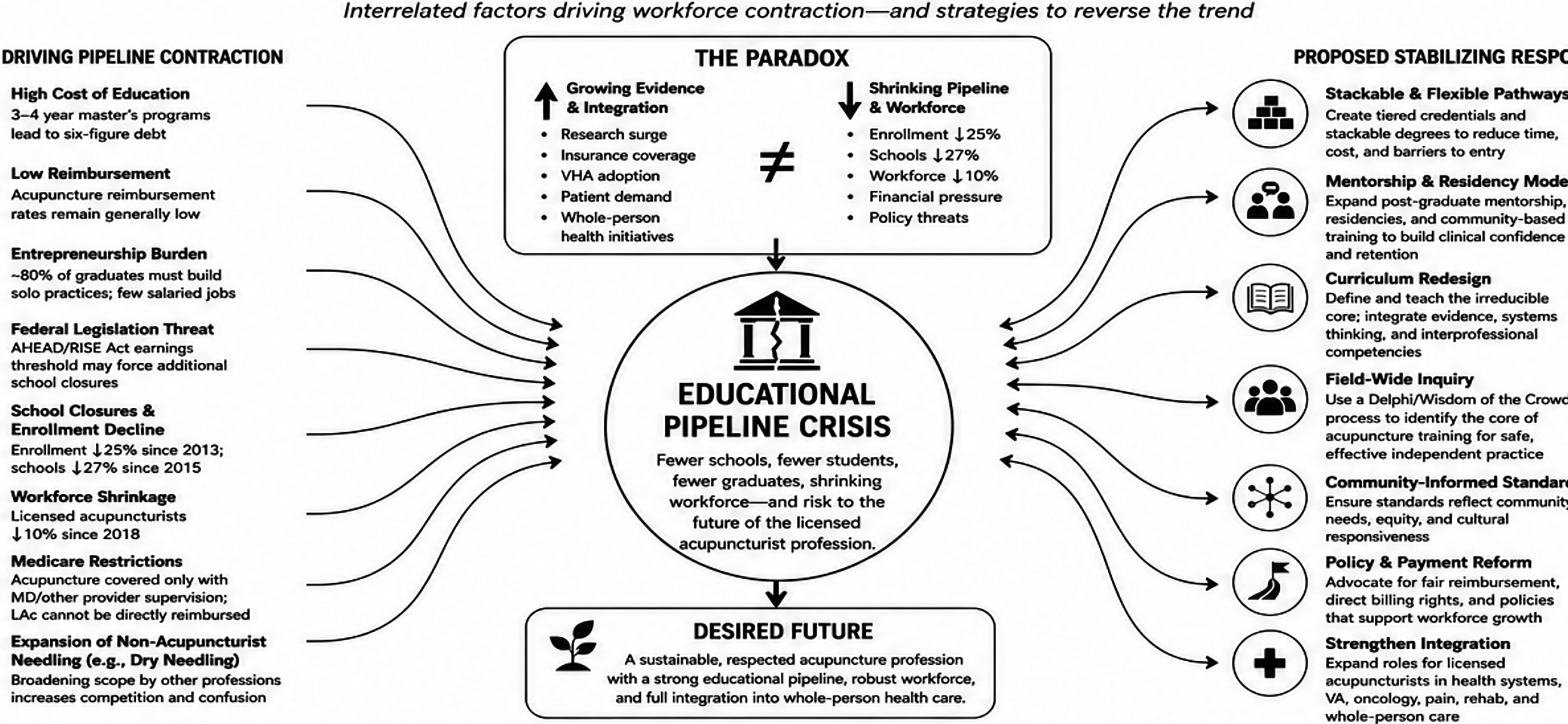
The Acupuncture Education Pipeline Crisis: A Systems Map.
Acupuncture school graduates, many of whom start new practices, are likely to underperform baccalaureates entering the conventional work force—particularly for the pandemic years. Institutions whose graduates on average fail this comparison will lose eligibility for federal student loans. For schools relying heavily on loans, failure will lead to school closure. If a large number of acupuncture schools close, this will threaten the sustainability of the regulatory and institutional structures that currently support acupuncture licensure and practice nationwide.
These structural organizations are briefly introduced below, along with actions they are taking to improve the trajectory (to our best current understanding; web links are provided for verification over time). Also briefly introduced are several schools and other organizations representing a range of approaches to the coming financial shock.
It seems clear that patient demand for acupuncture will continue to be met, particularly in the VHA and military where acupuncture is well established. The question is whether action can be taken quickly enough to secure a sustainable educational pipeline for licensed acupuncturists or whether some form of dry needling will take its place.
Roles and Responses by Core Institutions and Organizations
The
The
The
Comprehensive restructuring
Online coursework with hands-on clinic
Avoiding loans altogether
Additional Institutional and Organizational Approaches
These state-by-state efforts reflect both the urgency practitioners feel and the absence of a shared evidentiary basis for what training reform should preserve or change. Without a field-wide account of what acupuncturists in different practice contexts actually need from entry-level education, fragmentation at the state level is the predictable alternative to coherent national reform.
The
Notable at early WPC conversations were (A) minimal practitioner awareness of AHEAD implications and (B) minimal shared understanding of diverse patient priorities. In one conversation, community-based acupuncturists reported (their) patients’ indifference to degree titles, while practitioners treating oncology patients in health care settings argued that (for their patients) both the doctoral degree and its biomedical/research content are indispensable. This commentary and proposed study originated with the White Pine conversations; they aim to address practitioner information gaps as well as financial challenges through a ‘Wisdom of Crowds’ approach.
Shortening (or Lengthening) Degree Programs: What Is Essential?
As seen above, a number of parties are moving to reduce student debt by streamlining entry-level acupuncture curricula. However, others argue that employment opportunities and compensation in health care systems depend on high public and professional perception of standards and advocate for maintaining (or increasing) them.26,27
These two positions, each widely held and deeply entrenched, appear logistically incompatible within the current context of United States health care and legislation. The World Health Organization’s 2020 benchmarks for acupuncture education, from international consensus panels, recommend two tiers (basic 1,568 h; advanced 2,468 h). Tiering would seem a promising approach to the diverging priorities of community- and system-based acupuncturists. However, challenges to United States implementation would be considerable, from educational regulation to VHA and other institutional pay scales to meaningful differences between WHO basic recommendations and longstanding United States community-oriented curricula. A practitioner-wide inquiry could surface what changes address which United States needs while building the profession’s shared understanding of what is and isn’t feasible for whom. Approaches already garnering some broad agreement include stackable credentials and formal mentorship analogous to the internship and residency structures common across medical and mental health professions. 28 It is clear that changes will be made to national curricular standards in response to the current crisis. The question is, based on what evidence?
ACAHM’s straw poll should provide a rapid, urgently needed account of practitioners preferences among three approaches presently under discussion. Conversely, NCBAHM’s Job Analysis (conducted every 5–7 years, most recently in 2024) does not concern curriculum but provides a record of what practitioners report actually doing in their clinic. What neither of these provides is evidence, or analysis, of which patient needs, in which populations, acupuncturists currently work to meet using what essential skills; and how acupuncturists see their practices being impacted by lowering, raising, or tiering standards.
Proposal for a Timely Study
We propose a rapid (6 month), qualitative, community-focused research initiative. Conducted by practitioner-researchers, independently from ACAHM or NCBAHM, the study will provide impartial evidentiary support for those and other institutions’ decision-making. Also—crucially—it will increase practitioners’ own understanding of the field’s diversity and their sense of genuine engagement in the existential institutional decisions that will inevitably be taken over the coming few years.
It is well understood that a robust group decision-making process dampens the noise of individual variations in judgment; however, group dynamics can amplify that noise. 29 When curriculum decisions are made by committee, existing hierarchies are reproduced in a format that may look like consultation but ignore the concerns of less empowered members. 30 The Delphi method addressed this problem in Cold War strategy through iterative, anonymous, facilitated communication between experts. Subsequent modifications have included online structures to reduce researcher bias, as well as ‘Policy Delphi’ strategies for crafting coherent policy decisions by collectively identifying and exploring the full range of diverging and dissenting approaches. 31 See Figure 2, Wisdom of Crowds Delphi Study.
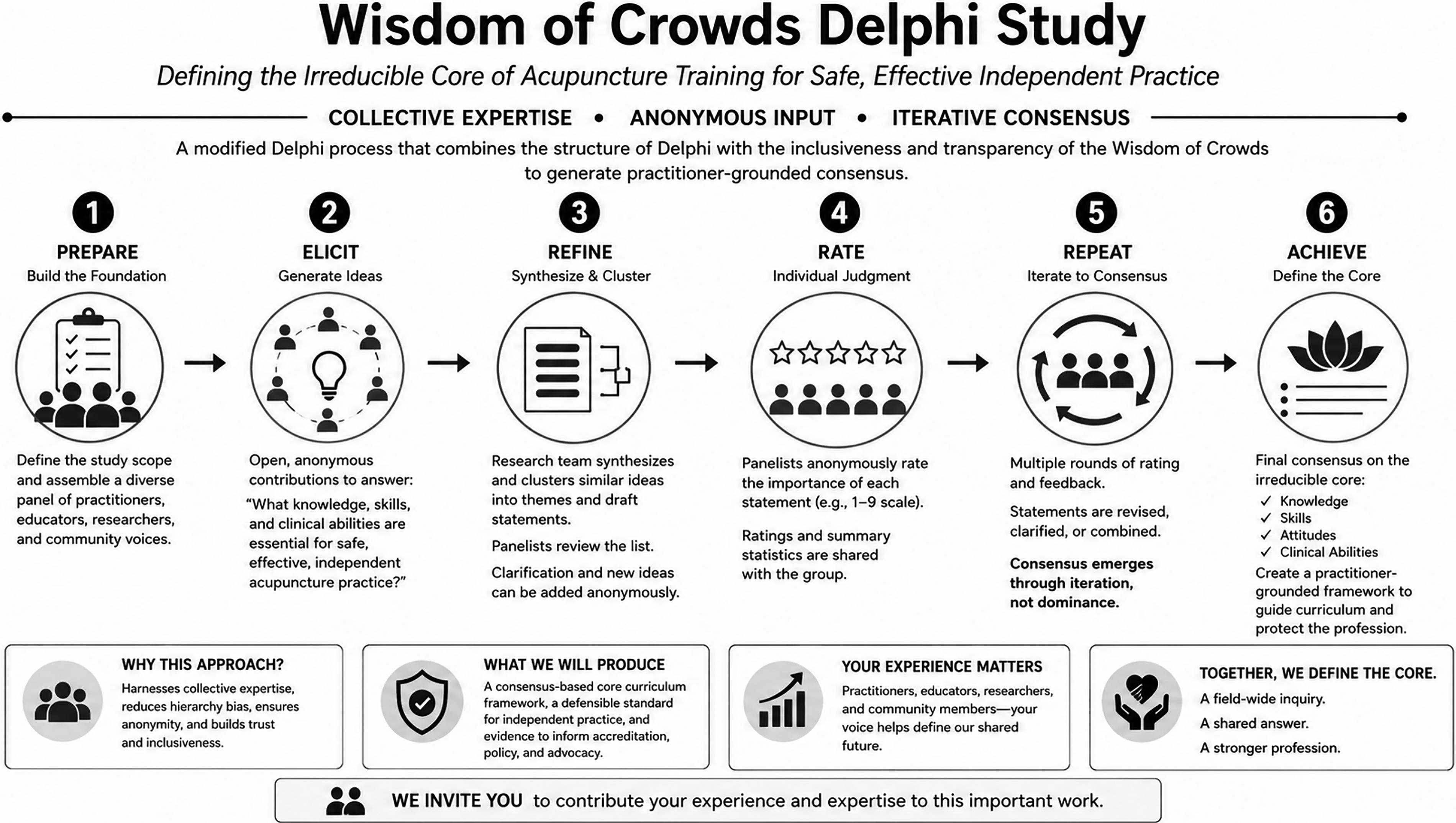
Wisdom of Crowds Delphi Study.
The Wisdom of Crowds approach specifies four conditions within which even expert opinion is reliably outperformed by community collective judgment: 1, contributors bring diverse perspectives; 2, their judgments form independently; 3, knowledge is distributed across the group; and 4, the aggregation mechanism does not introduce bias.32–34 This approach has been applied to health professions curriculum design, to identify core competencies.35,36 We have designed a modified Policy Delphi study (Fig. 1, Wisdom of Crowds Delphi Study), structured around these four conditions, aiming to both inform and engage 150–300 acupuncturists or others with expertise in delivering, researching, or otherwise financially or logistically supporting acupuncture therapy. Questions posed for iterative, AI-assisted synthesis and review include: What is the irreducible safety and efficacy core for entry-level practice? Which competencies belong in stackable post-entry credentialing rather than initial licensure? Where should a technician-versus-graduate scope line be drawn?
Importantly, this is not curriculum design: it is the use of research methods to transparently aggregate divergent experiences, mutually digesting them through two rounds of facilitated response to collected themes. Our output will not be an inclusion/exclusion binary but a faithful and collaborative distillation of what acupuncturists think is essential to be considered by those proposing new curricula or licensure. Results will be disseminated without advocacy.
A Call to Advocacy and Action Through Research
We propose to disseminate and implement this preliminary, brief query as a large-scale community action that simultaneously informs practitioners and also elicits foundational participation in their profession’s training process. Detailed methods can be found in our protocol paper online: https://www.evidencebasedacupuncture.org/acepathstudy. We hope that “snowball” sampling (in which diverse, purposively selected initial participants are asked to forward an invitation link to colleagues) will be leveraged through dissemination by the AHM Coalition and other organizations, including SAR and the practitioner-facing platform Evidence Based Acupuncture.
The acupuncture profession has long been fragmented in its advocacy. A field-wide study on core essentials will not resolve every institutional disagreement. But it would provide something that we currently lack: a shared account, arrived at through a rigorous and independent process, of what training acupuncturists and other impacted constituencies believe is foundational and cannot be cut.
Footnotes
Funding and Conflict of Interest Statement
The study is not funded. The authors each have academic affiliation listed above.