
Abstract
Background:
Psychological distress is common among individuals with stimulant use disorder (StUD) and may affect treatment outcomes, with potential differences in men and women. We examined the impact of comorbid psychological distress on StUD treatment outcomes across behavioral interventions, with a focus on differences by sex.
Methods:
Data were pooled from 4 randomized controlled trials of behavioral interventions (eg, motivational interviewing, 12-step, and smoking-cessation) for StUD (n = 1858) from the National Institute on Drug Abuse Data Share. Psychological distress was assessed using the Addiction Severity Index-psychiatric problems subscale (≥0.246 cutoff). Outcomes included (a) any reduction in stimulant use frequency from baseline to the end of trial, (b) stimulant-positive urine test, and (c) other drug-positive urine tests at the end of trial. We used individual participant data meta-analysis with regression models, adjusting for sociodemographic factors, treatment arms and trial duration, and clustering by trials. We used inverse probability weighting to address missing data. Analyses were conducted on the full sample and stratified by sex.
Results:
Overall, 57.1% of women and 38.7% of men experienced psychological distress. Among men, psychological distress was associated with decreased odds of reducing stimulant use (adjusted odds ratio [aOR] = 0.70, 95% confidence interval [CI] = 0.49, 0.99), and increased odds of having a stimulant-positive urine test (aOR = 1.23, 95% CI = 1.03, 1.47). Among women, distress was not significantly associated with reduced stimulant use or with having a stimulant-positive urine test. However, psychological distress moderated the treatment effect: women with psychological distress who received behavioral interventions were more likely to reduce stimulant use than those without psychological distress.
Conclusion:
Psychological distress was associated with poorer treatment outcomes for men but appeared to enhance treatment response for women. Screening and addressing psychological distress may improve StUD treatment. Sex differences highlight the need for sex-specific approaches to managing psychological distress in StUDs.
Keywords
Highlights
Nearly half of individuals with stimulant use disorder (StUD) experienced psychological distress.
Women reported a higher prevalence of comorbid psychological distress than men.
Among men, psychological distress was associated with poorer StUD treatment outcomes overall.
Among women, psychological distress moderated the treatment effect and improved treatment outcomes.
Introduction
Stimulant use disorders (StUDs), including cocaine, amphetamine, and methamphetamine use disorders, remain major public health concerns affecting approximately 4.3 million people in the United States. 1 StUDs frequently co-occur with mental health disorders,2-4 particularly psychological distress, defined as a state of emotional suffering characterized by mental and somatic symptoms that are associated with normal fluctuations of mood. 5 Psychological distress often manifests as symptoms of anxiety, depression, and emotional dysregulation. Many individuals with StUDs experience significant but subthreshold symptoms of mood and anxiety disorders that do not meet full diagnostic criteria, and as a result, often remain untreated despite experiencing substantial distress and functional impairment. Such comorbid psychological distress is associated with greater health and social burden in individuals with StUDs and other substance use disorders,6-9 including greater legal, family, and medical problems.10-13 These social and health factors, in turn, can impact the outcomes and effectiveness of StUD treatment.
Although prior studies estimate that over 40% of individuals with StUDs experience significant psychological distress,4,14,15 research examining the impact of distress on StUD treatment outcomes is limited. While one study found that comorbid psychiatric disorders may not directly impede recovery, the study found that the presence and severity of depressive symptoms can negatively affect treatment completion. 16 Other studies have found psychological distress to be associated with higher craving and lower self-efficacy to refrain from drug use, poorer treatment retention, higher methadone dosing, and more substance-related complications, including hepatitis C and HIV risk behaviors.11,17,18
Furthermore, sex differences in the association of psychological distress with StUD outcomes and treatment response are rarely examined, while these differences have been consistently observed in stimulant use behaviors, StUDs, and psychological distress. Men are more likely to have a higher prevalence and report higher frequency of stimulant use, 19 whereas women tend to progress more rapidly to dependence following initiation.20-22 Women with StUDs are also more likely to present with co-occurring symptoms of depression, anxiety, and distress,4,23,24 while men often demonstrate antisocial and risk-taking behaviors.25,26 Importantly, comorbid psychological distress appears to interact with substance use differently among men and women, with women more likely than men to use substances as a way of coping with psychological distress.23,27
Collectively, these findings underscore the need for consideration of sex-specific pathways in the relationship between psychological distress and StUD outcomes and treatment response to inform the development of more integrated, sex-responsive treatment strategies. However, prior studies have been limited by small sample sizes, heterogeneous measures of psychological distress, and limited assessments by sex, making it difficult to draw robust conclusions. Building on our research team’s previous work demonstrating that comorbid psychological distress decreases StUD treatment retention and that sex differences shape methamphetamine use disorder treatment outcomes,14,18 the current study used harmonized individual participant-level data from 4 randomized controlled trials (RCTs) of behavioral interventions for StUDs to examine the effect of comorbid psychological distress on treatment outcomes. The study capitalized on a large pooled and harmonized sample of participants from 4 RCTs using very similar methodology and measures to assess the associations of psychological distress, measured consistently across trials, with outcomes and behavioral treatment response for StUDs. We further assessed whether these associations differed between men and women.
Methods
Study Design and Sample
Data were drawn from 4 completed multisite RCTs of behavioral interventions for StUDs. The data are publicly available through the National Institute on Drug Abuse (NIDA) Data Share Website (https://datashare.nida.nih.gov). These 4 RCTs were selected because the trials shared a core set of measures and employed similar study designs, eligibility criteria, and quality assurance procedures. The data harmonization methods and original studies have been previously described. 28
The combined dataset comprised 1866 participants who were at least 18 years old and had a Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) diagnosis of a StUD. Participants were excluded from the trials if they were pregnant, had severe psychiatric disorders that required ongoing treatment, were at significant risk for suicide, or were deemed unable to safely participate in RCTs based on the investigators’ judgment.
Each of the StUD RCTs (Table 1) examined the effects of one behavioral intervention, including motivational interviewing,29,30 12-step, 31 and smoking cessation, 32 compared to treatment as usual (TAU). Across all 4 RCTs, TAU included standard weekly group counseling sessions provided at community treatment programs along with family counseling as needed. The duration of the trials ranged from 8 to 12 weeks. The current study involves the secondary analysis of publicly available deidentified data of trial participants; therefore, analysis was deemed exempt from review by the Institutional Review Board of the Johns Hopkins Bloomberg School of Public Health.
Any Stimulant Use Disorder RCT Characteristics and Participant Demographic Characteristics.
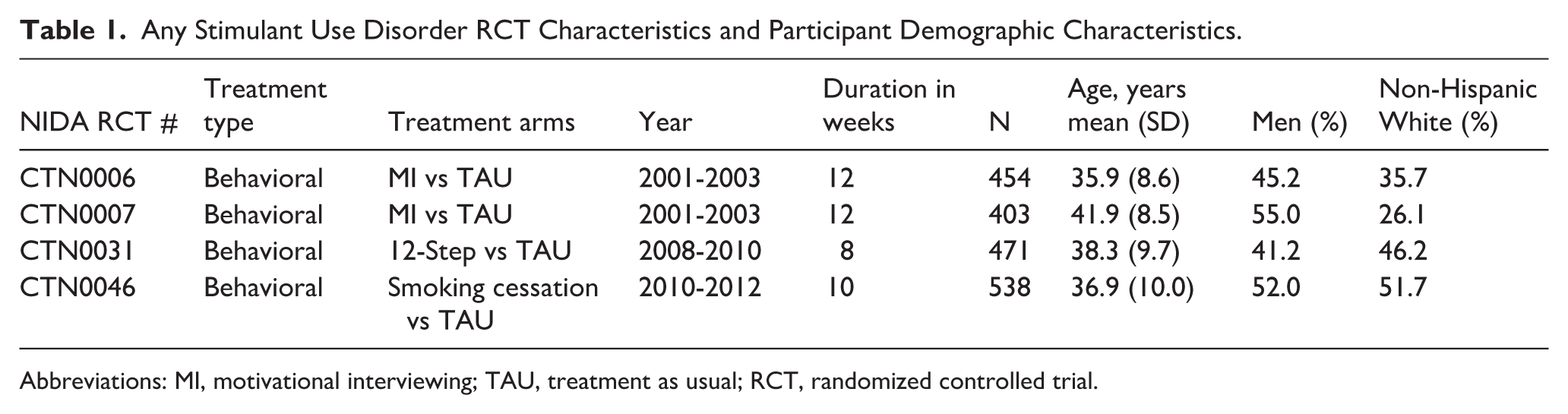
Abbreviations: MI, motivational interviewing; TAU, treatment as usual; RCT, randomized controlled trial.
Measures
Psychological distress was measured using the psychiatric domain of the Addiction Severity Index (ASI-Psych), a standardized semi-structured clinical interview. The ASI-Psych provides a comprehensive assessment of psychological distress by incorporating a wider range of symptoms that frequently co-occur and shape functioning and recovery among individuals with substance use disorders, 33 including depression, anxiety, psychosis, cognitive difficulties, problems with impulse control and aggression, and suicidal ideation and attempts. Importantly, ASI administration guidelines instruct interviewers to distinguish symptoms that reflect underlying psychological problems from those attributable to acute intoxication or withdrawal, helping ensure that participant responses reflect broader psychological distress rather than transient substance-related effects. 34
The ASI-psych composite score was derived from 11 items, which include 7 yes/no items evaluating the presence of psychological symptoms, excluding symptoms directly attributable to substance use, that were experienced for a significant duration within the past 30 days. These symptoms included serious depression, anxiety or tension, hallucinations, trouble understanding or concentrating, trouble controlling violent behaviors, and thoughts or attempts of suicide. The eighth item assessed the use of prescribed medications for emotional or psychological issues. The remaining 3 items measured the number of days participants reported experiencing emotional or psychological problems (scored continuously from 0 to 30), the degree to which these problems were considered troublesome, and the perceived importance of treatment for these problems. The latter 2 items were scored on a 5-point ordinal scale ranging from 0 (“not at all”) to 4 (“extremely”). Composite scores were calculated according to guidelines from the Composite Scores Manual, 35 yielding values from 0 to 1, with higher scores indicating more severe psychological distress. A dichotomous variable was also created to distinguish between individuals with and without significant psychological distress in the past 30 days. A threshold of 0.246 was validated in a large multi-site sample of individuals with substance use disorders, the majority of whom had StUD. 33 The cutoff demonstrated moderate accuracy for detecting psychiatric disorders based on diagnoses from the Structured Clinical Interview for DSM or Mini International Neuropsychiatry Interview (Area Under the Curve = 0.74) among individuals with StUDs.
The primary treatment outcome was any reduction in the frequency of stimulant use from baseline to the end of trial, measured using the ASI drug domain. Consistent with prior studies,36-38 the frequency of use was categorized into 3 levels: no use (0 days), low-frequency of use (1-4 days), and high-frequency of use (≥5 days). Because of sample size limitations with the three-category variable, we derived a binary outcome variable to indicate any reduction in stimulant use, that is, any versus no reduction. Participants who transitioned from high-frequency to low-frequency use or to abstinence were classified as having reduced their use, whereas participants whose use remained the same or increased were categorized as having no reduction in use.
The secondary treatment outcome included results from urine drug screens for any stimulant and other substances (eg, opioids, benzodiazepines, cannabis, and barbiturates) at the end of the trial. Binary outcome variables were created for each substance based on results from the 2 most recent assessments prior to trial completion, that is, positive versus negative. If either assessment yielded a positive result, it was considered treatment failure. Conversely, 2 consecutive negative tests were considered treatment success. If one test was negative and the other was missing, the outcome was coded as missing.
Covariates included participants’ sociodemographic and clinical characteristics, including age, sex (man/woman), marital status (legally married/cohabiting, divorced/widowed/separated, and single/never married), homelessness, years of education completed, history of chronic medical illness, and race-ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, and other). The “other” category included participants who identified as Multi-Racial, Native Hawaiian or Other Pacific Islander, American Indian/Alaska Native, and Asian.
Statistical Analysis
Of the total study sample (n = 1866), 3 participants had no information available for any of the study measurements, and 5 had missing ASI-psych items, precluding the computation of the ASI-psych composite score. Therefore, the analytic sample was limited to 1858 participants with complete data.
First, we compared sociodemographic and clinical characteristics for men and women with and without psychological distress using chi-squared tests for binary and categorical variables and t-tests for continuous variables. We also compared the psychological symptoms from the ASI-psych between men and women.
Next, we conducted a series of regression analyses using the methods of one-stage individual participant data (IPD) meta-analysis, 39 to assess the association between psychological distress and each of the 3 outcomes: (1) reduction in the frequency of stimulant use, (2) urine toxicology ascertained stimulant use at the end of the trial, and (3) urine toxicology ascertained use of other drugs at the end of the trial. IPD meta-analysis methods were used to enhance methodological rigor and account for between-trial variability.40,41
Using both binary (ASI-psych score ≥0.246) and continuous (ASI-psych composite score 0-1) exposure variables of psychological distress, 3 hierarchical logistic regression models were conducted for each outcome. Model A was the crude model, Model B adjusted for sociodemographic covariates, including age, sex, race-ethnicity, education, treatment arm, and duration of the trials. We also incorporated clustering by trial in the model to account for heterogeneity across trials. Model C further addressed missing outcome data using inverse probability weighting (IPW). All the analyses were conducted for the total sample and also separately for men and women. We report odds ratios (OR), adjusted odds ratios (aOR), and their corresponding 95% confidence intervals (95% CI).
Finally, we examined if the overall treatment effect (behavioral intervention vs TAU) on StUD treatment outcomes was moderated by psychological distress using two-way interaction terms (psychological distress × StUD treatment) in both the total sample and stratified by sex. These models were adjusted for sociodemographic covariates and accounted for missing outcome data. All statistical analyses were performed in Stata/MP version 18.0. 42
Results
Description of Sample
Of the total sample (n = 1858), 48.2% experienced serious psychological distress. Compared to men, women had higher prevalence of psychological distress (57.1% vs 38.7%, P < .001) and had a higher average ASI-Psych composite score (0.25 vs 0.19, P < .001). Baseline sociodemographic and clinical characteristics associated with psychological distress varied among men and women (Table 2). Among individuals with psychological distress, women were more likely to be younger than 35 years (42.5% vs 33.9%), whereas men were more likely than women to be over 50 years of age (14.9% vs 7.7%); a similar pattern was observed among participants without psychological distress. For education, among those with psychological distress, women had slightly higher mean years of education compared to men (12.1 vs 11.7), whereas among those without psychological distress, men had higher mean years of education (12.0 vs 11.7). Differences in race/ethnicity were small and did not follow a specific pattern across both groups.
Baseline Sociodemographic and Clinical Characteristics, Stratified by Gender.

Bold values indicates statistical significance (P < 0.05).
Symptoms of Psychological Distress Among Men and Women
Overall, the prevalence of psychological distress symptoms was higher among women compared to men (Table 3). Women had significantly higher prevalence of serious depression (40.7% vs 31.2%), serious anxiety and tension (50.6% vs 39.0%), trouble understanding or concentrating (44.8% vs 31.7%), trouble controlling violent behavior (15.8% vs 11.4%), and serious thoughts of suicide (7.3% vs 3.9%). Women were also significantly more likely than men to have a greater mean number of days of experiencing psychological or emotional problems (11.1 vs 6.9 days) and to have been prescribed medication for psychological impairment (33.5% vs 15.5%). Furthermore, women were significantly more likely than men to report being “considerably” or “extremely” troubled or bothered by psychological or emotional problems (40.7% vs 26.5%) and to perceive treatment for psychological problems as more important (48.5% vs 29.2%).
Distribution of Psychological Distress (ASI-Psych) Symptoms in the Past 30 Days, Stratified by Gender.
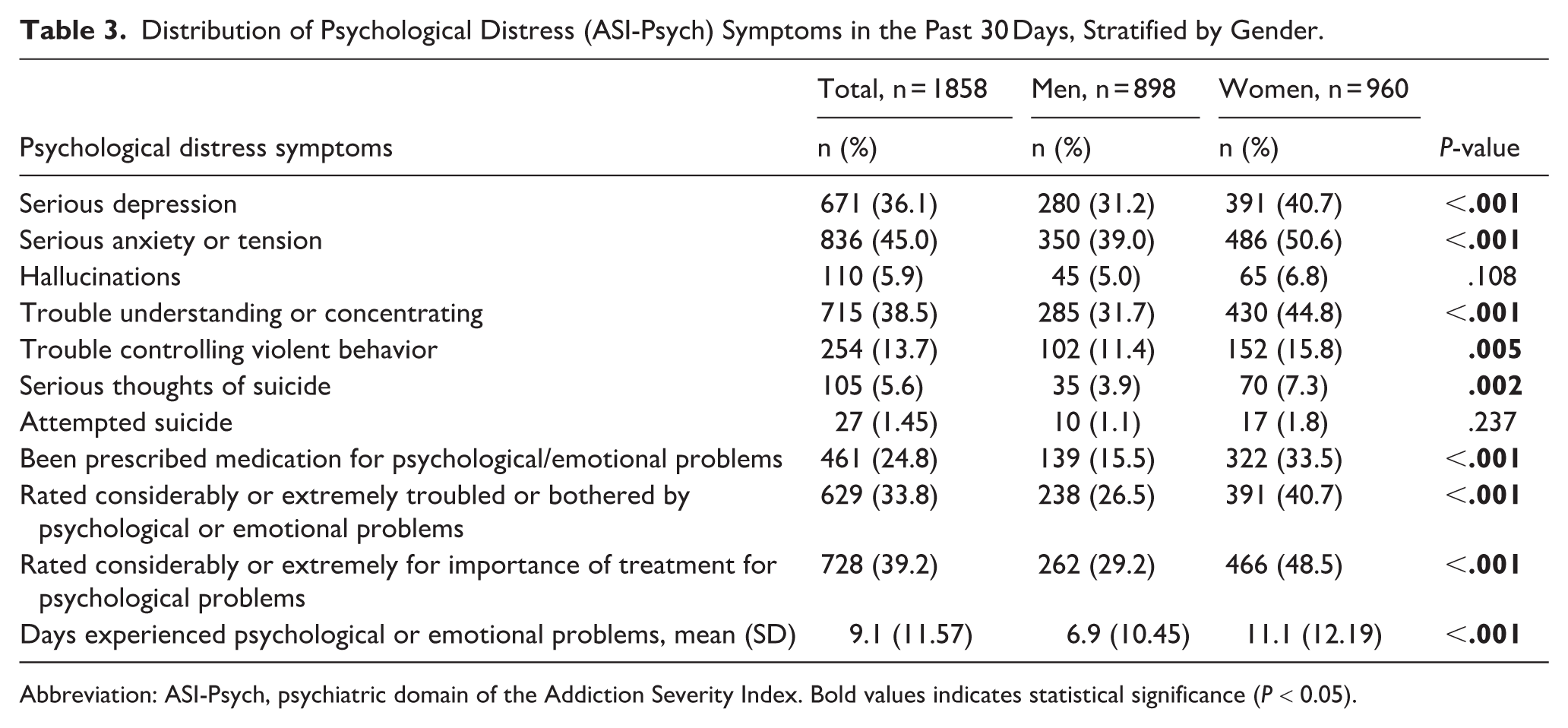
Abbreviation: ASI-Psych, psychiatric domain of the Addiction Severity Index. Bold values indicates statistical significance (P < 0.05).
Association of Psychological Distress With StUD Outcomes
We did not find any significant associations between psychological distress and StUD outcomes in the crude models (Model A). However, after adjusting for covariates in Model B, in the total sample, using the dichotomous ASI-psych exposure variable (Table 4A), individuals with psychological distress had lower odds of achieving reduced frequency of stimulant use (aOR = 0.73; 95% CI = 0.55, 0.98; P = .035). When IPW was applied to address missingness (Model C), the association was slightly attenuated and the statistical significance was reduced to a trend level (aOR = 0.77; 95% CI = 0.57, 1.03, P = .083).
The Association of Psychological Distress and Outcomes of Stimulant Use Disorders, Stratified Analysis by Gender.

Abbreviations: OR, odds ratio; aOR, adjusted odds ratio; CI, confidence interval; ASI-Psych, psychiatric domain of the Addiction Severity Index; RCT, randomized controlled trial. Bold values indicates statistical significance (P < 0.05).
Model A was not adjusted for any covariates; bModel B was adjusted demographic characteristics (sex, age, race, and education), treatment arm and duration of treatment, and clustering within RCTs; cModel C was adjusted demographic characteristics (sex, age, race, and education), treatment arm and duration of treatment, clustering within RCTs, and inverse probability weighting (IPW) to address missingness in outcome measures.
Sex-stratified analyses revealed notable differences in these associations in Models B and C. Using the dichotomous ASI-psych exposure variable, men with psychological distress had a higher likelihood of experiencing unfavorable outcomes, such as a lower odds of reduced frequency of stimulant use (aOR = 0.64; 95% CI = 0.43, 0.96; P = .033), and higher odds of a positive urine test for stimulants (aOR = 1.22; 95% CI = 1.01, 1.48; P = .048). Similarly, the continuous ASI-psych exposure variable (Table 4B) was associated with lower odds of reduced frequency of stimulant use (aOR = 0.38; 95% CI = 0.15, 0.95; P = .040) and higher odds of a positive urine test for stimulants (aOR = 2.01; 95% CI = 1.38, 2.91; P < .001) among men. These results remained consistent in the IPW models, demonstrating lower odds of reduced use (dichotomous exposure: aOR = 0.70; 95% CI = 0.49, 0.99; P = .046; continuous exposure: aOR = 0.43; 95% CI = 0.20, 0.92; P = .029), and higher odds of a positive urine test for stimulants (dichotomous exposure: aOR = 1.23; 95% CI = 1.03, 1.47; P = .024; continuous exposure: aOR = 2.00; 95% CI = 1.41, 2.85; P < .001) associated with ASI-psych in men.
In contrast, women with psychological distress did not significantly differ from those without psychological distress across outcomes of reduced frequency of stimulant use and positive stimulant urine test using both dichotomous and continuous ASI-psych. Additionally, men and women with distress did not significantly differ from their counterparts without distress on the outcome of positive urine test for other drugs at the end of the trial.
Impact of Psychological Distress on Treatment Effect
In the total sample, no statistically significant interactions were found between psychological distress and treatment (behavioral intervention vs placebo) for any of the StUD treatment outcomes (Table 5).
Treatment Effect on Outcomes of Stimulant Use Disorders Among Those With and Without Psychological Distress, Stratified by Gender.

Bold values indicates statistical significance (P < 0.05).
Indicates a two-way interaction (stimulant use disorder treatment × psychological distress).
Sex-stratified analyses showed that psychological distress moderated the treatment effect on achieving reduced frequency of stimulant use (χ2 = 31.10, P < .001) in women. Among women with psychological distress, those who received the behavioral intervention were more likely to have reduced stimulant use compared to those who received TAU (64.0% vs 59.0%, respectively). Conversely, among women without psychological distress, those who received the behavioral intervention were less likely to have reduced stimulant use compared to TAU (62.0% vs 67.8%, respectively). However, no significant interaction was found for reduced frequency of stimulant use from baseline to the end of trial among men. Similarly, psychological distress did not moderate treatment effect on achieving a positive urine test for stimulants and other drugs, neither for men nor for women.
Discussion
In this study of 4 multisite RCTs of behavioral interventions for StUDs, we found that comorbid psychological distress was common among individuals with StUDs, affecting nearly half of the sample, with significantly higher prevalence and severity among women compared to men. Women reported higher rates of depressive and anxiety symptoms, greater use of prescribed medication for psychological problems, and a greater perceived need for treatment. These findings are consistent with previous research demonstrating high rates of psychiatric comorbidity among individuals with substance use disorders,43-46 particularly among women.20,47,48
The impact of psychological distress on StUD outcomes differed by sex. Among men, psychological distress was consistently associated with unfavorable outcomes, such as lower odds of reduced frequency of stimulant use and higher odds of a stimulant-positive urine test at the end of treatment. One plausible explanation for this finding is that distress among men may exacerbate risk-taking behaviors or impair impulse control, contributing to poorer treatment response. 49 Additionally, cultural and social norms around masculinity often discourage men from expressing emotional vulnerability and seeking psychological support.50-52 Consequently, psychological distress in men may remain untreated, increasing the likelihood of maladaptive coping strategies such as continued stimulant use.
In contrast, although psychological distress was more prevalent and severe among women, its negative impact on treatment outcomes appeared to be less pronounced. One possible explanation is that women experiencing distress may perceive a greater need for treatment,53,54 leading to earlier engagement with treatment systems, thereby mitigating adverse outcomes. This corresponds with our finding that women with psychological distress who received behavioral interventions demonstrated higher rates of reduced stimulant use compared to those receiving TAU, suggesting that distressed women may have derived greater benefit from treatment.
Our findings highlight the need to better understand the mechanisms linking psychological distress with outcomes of StUDs and the impact of StUD treatments. Although the precise mechanism remains unclear, emotional stress has been associated with increased drug craving and drug-seeking behavior among individuals with StUDs,55-57 while depressive symptoms may reinforce the effects of stimulants and increase vulnerability to relapse. 58 Moreover, the physiological and psychological discomfort associated with withdrawal during treatment may further exacerbate distress, 59 creating a negative feedback loop in which substance use becomes a primary coping strategy to alleviate anxiety and dysphoria. 60 These interrelated processes may disproportionately affect men, who are less likely to seek support for psychological distress and may rely more heavily on stimulants as a coping mechanism, thereby contributing to poorer outcomes. In contrast, in women, psychological distress may have a buffering effect by increasing perceived need for care and treatment engagement. Future research needs to corroborate the study’s findings and further examine the possible mechanisms for sex differences.
This study has several limitations. First, the RCTs excluded participants with severe psychiatric disorders, potentially underestimating the impact of comorbid psychological distress on treatment outcomes. Second, diagnoses of StUDs in these trials were based on DSM-IV criteria. Although the DSM-5 introduced changes by combining abuse and dependence into a single substance use disorder with severity specifiers and adding craving as a criterion, prior research indicates that DSM-IV substance use dependence more closely aligns with DSM-5 moderate and severe substance use disorder. 61 Third, the use of a binary outcome variable indicating any reduction in the frequency of stimulant use (ie, any vs no reduction) may treat small and large changes equivalently. However, the small sample size (<5%) in the “high- to low-frequency use” or “reduced use” category precluded our ability to model more granular changes. Fourth, the trials were relatively short, limiting our ability to assess long-term associations between distress and treatment outcomes. Fifth, the 4 RCTs included in our study had different durations and varied in the nature, quality, and intensity of substance use disorder treatments. We attempted to account for these differences by adjusting all analyses for duration and type of treatment. Lastly, our study was limited to adults who were willing to participate in an RCT, which does not necessarily represent all individuals with StUDs. Furthermore, the RCTs were all based in the United States. Therefore, generalizability of findings to individuals receiving StUD treatment in usual care settings and settings outside of the United States may be limited.
Nonetheless, our findings have important clinical implications for StUD treatment. Routine clinical screening for psychological distress can help identify individuals who may not voluntarily disclose stressful experiences or psychiatric symptoms, or who may attribute such symptoms solely to substance use. Systematic screening may also detect subclinical symptoms that would otherwise go unrecognized but that still interfere with treatment engagement and recovery. Brief, validated screening tools that are feasible for use in busy clinical settings, such as the General Health Questionnaire-12 or the Kessler-6,5,62,63 have strong psychometric properties and can facilitate identification of psychological distress, enabling timely referral to mental health providers and the integration of supportive services within StUD care.
The findings also highlight the need for sex-responsive approaches to StUD treatment. Women had higher levels of psychological distress, and distressed women receiving behavioral interventions demonstrated greater reductions in stimulant use compared to TAU, suggesting that expanding and tailoring psychosocial support for women may enhance treatment response. Prior research on sex-responsive and women-centered substance use treatment models has demonstrated improvements in retention, reduced substance use, and enhanced psychosocial outcomes compared to mixed-gender approaches, particularly among women with complex trauma histories.64-67 Therefore, StUD treatment programs for women should extend beyond addressing psychological distress to address broader psychosocial vulnerabilities, including relational risks, trauma histories, and caregiving responsibilities, that shape their substance use trajectories. 27 For men, who may be less likely to verbalize psychological symptoms and seek mental health services, routine psychological distress screening within clinical settings may improve detection and facilitate timely intervention. Future research should not only investigate sex-specific differences in the long-term effects of psychological distress on StUD treatment outcomes but also explore the mechanisms that may underlie these differences. Additionally, evaluation of sex-responsive treatment models is critical to determine their effectiveness and improve treatment retention, reduce relapse, and promote recovery.
Footnotes
Authors’ Note
Part of the study findings were presented at the 2025 Annual Meeting of the Association for Medical Education and Research in Substance Abuse (AMERSA).
Ethical Considerations
Institutional Review Board approval was not required.
Author Contributions
HB: Formal analysis (lead); investigation (lead); visualization (lead); writing—review and editing (lead); and writing—review and editing (lead).
MA-E: Conceptualization (supporting); formal analysis (supporting); methodology (supporting); and writing—review and editing (supporting).
RS: Conceptualization (supporting); formal analysis (supporting); methodology (supporting); and writing—review and editing (supporting).
RM: Conceptualization (lead); supervision (supporting); validation (supporting); project administration (supporting); writing—review and editing (supporting).
RMC: Conceptualization (lead); supervision (lead); validation (lead); project administration (lead); writing—review and editing (supporting).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (R01DA058008) to MPIs: Dr. Ramin Mojtabai and Dr. Rosa M. Crum. Dr. Mojtabai’s work was supported in part by the Louisiana Board of Regents Endowed Chairs for Eminent Scholars program. Contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Mojtabai has received royalties and consulting fees from UpToDate, Medscape, and MindMed, as well as providing consultation regarding social media litigation on behalf of the Plaintiffs.