
Abstract
The iLet Bionic Pancreas (iLet) is an FDA-approved automated insulin delivery system designed to manage glycemia through use of the iLet Dosing Decision Software. It uses real-time glucose data from a compatible continuous glucose monitor to automatically adjust and deliver insulin without the need for manually calculating, programming, and adjusting insulin therapy settings. The iLet autonomously determines all insulin dosing. For this context, autonomous insulin delivery is referring to the fact that all system dosing is independently determined by the system without requiring baseline clinician determined settings, but the system does require qualitative meal announcements by the user. It is shifting the paradigm for glycemic management toward simplification and expanding technology access to a broader population. The shift from adjusting settings to behavioral education represents a return to the art of medicine for the clinician. While the clinician no longer needs to adjust settings, they are not powerless when faced with dysglycemia. Clinical interventions are education focused. In this review, we provide clinical guidance for diabetes management with the iLet Dosing Decision Software (Beta Bionics, Irvine, CA, United States). Other systems with similar autonomous functionality and learning capability will likely be available in the coming years.
Keywords
Introduction
The Diabetes Control and Complication Trial (DCCT) and United Kingdom Prospective Diabetes Study clearly demonstrated strong association between glycemic outcomes (A1c) and diabetes complications.1,2 Unfortunately, the optimal glycemic outcomes in the intensive insulin treatment arms in the DCCT were achieved with increased incidence of severe hypoglycemia. With significant advances in automated insulin delivery systems, achieving glycemic goals without significant hypoglycemia is now feasible and without increasing significant burden on users. 3
The progress in insulin delivery started from low-glucose and predicted low-glucose suspension of insulin delivery to algorithm-driven semiautomated insulin delivery based on sensor glucose with manual meal and correction boluses.4–6 Ongoing advances include autocorrection boluses, scaling correction dosing based on the rate of glucose change, multiple glucose target set points and the latest, a fully adaptive system available commercially in the United States.7,8 A number of studies have shown improved glycemic outcomes without increasing risk for hypoglycemia with automated insulin delivery (AID) systems. Hence, the American Diabetes Association (ADA) Standards of Care recommend AID for all individuals with insulin-requiring diabetes. 3
Despite strong evidence, the use of AID systems in the real-world, while increasing, remains low. 9 Barriers to using AID include lack of knowledge, provider inertia, cost, and perceived complexity in initiating AID systems. Progressively more autonomous insulin dosing is shifting the paradigm for glycemic management toward simplification and expanding technology access to a broader population. The shift from adjusting settings to behavioral education represents a return to the art of medicine for the clinician. While the clinician no longer needs to adjust settings, they are not powerless when faced with dysglycemia. Clinical interventions are education focused. In this review, we discuss management strategies for the clinician managing individuals using the iLet Dosing Decision Software (Beta Bionics, Irvine, CA, United States).
Background/Evidence
The iLet Bionic Pancreas (iLet) is an FDA-approved AID system designed to manage glycemia through use of the iLet Dosing Decision Software. It uses three adaptive closed-loop algorithms along with a compatible continuous glucose monitor (CGM) to automate insulin delivery, autonomously titrating all therapeutic insulin, including basal, correction, and prandial insulin. 10 Current adaptive closed-loop algorithms, such as the iLet system, describe the algorithms as closed in that the dosing is independently determined by the system versus influenced by adjustable background insulin settings. User interaction is still required to initiate qualitative meal announcements for the iLet system to adapt to the user’s mealtime insulin needs. The next stage in AID development would be optional or have no need for meal announcements.
In the 13-week pivotal randomized controlled clinical trial in 440 subjects with type 1 diabetes, iLet use led to a 0.5% absolute reduction in A1C compared with control treatment (the participant’s usual insulin delivery method), with no increase in hypoglycemia and with improvements in diabetes distress and self-management burden.10,11 A sub-analysis showed that use of the iLet led to similar improvements in A1C among both white and minority participants. 12 In research conducted on the psychosocial impact of iLet use, pivotal trial subjects and their families reported less worry, less time talking about diabetes, less friction with loved ones, and more freedom to enjoy their lives. 13 Adult study participants reported significant decreases in fear of hypoglycemia and in diabetes distress.
In ongoing real-world analysis, commercial iLet users have a higher baseline A1C than participants in the pivotal trial and achieve larger decreases from baseline A1C to iLet glycemic management indicator (GMI) values. 14 Derived from CGM data, the glycemic management indicator (GMI) provides an average estimate of a person’s blood glucose levels over a specified time period. GMI is frequently used in real-world analysis of data from users of diabetes technology including CGM and AID, to approximate A1C. Recent research reports that the change in GMI is influenced by the baseline A1C of the participants and it underestimates the true change in A1C; thus it may not fully capture the efficacy of an intervention in real-world studies or other research. 15 The GMI equation has been updated to overcome the stated limitation and, hopefully, the updated GMI may serve as a useful marker for clinical and real-world studies in the future.16,17
How the iLet Dosing Decision Software Works
The iLet Dosing Decision Software is currently utilized by the iLet Bionic Pancreas(™) but could be utilized in future alternate controller enabled pumps. Clinicians should be aware that software updates are frequently made in diabetes technology and it is important to stay current with ongoing updates. The system determines insulin doses every 5 min in response to glucose values from a CGM, insulin dosing history, and user input (e.g., meal announcements and, when CGM glucose values are not available, manually entered blood-glucose values). The system does not require any information about the user’s total daily dose of insulin, basal or long-acting insulin requirements, or insulin correction factors. The system has three algorithms running in parallel: an adaptive basal insulin algorithm, which continually adapts to each individual’s basal metabolic need for insulin; an adaptive correction algorithm, which provides doses that are required above and beyond the basal metabolic needs; and an adaptive meal dose algorithm which provides insulin in response to a meal announcement (Fig. 1). The only user input is qualitative meal announcements when eating, and the system will adapt to the user’s identified insulin needs for each meal type. All basal and correction dosing is automated by the system. 18
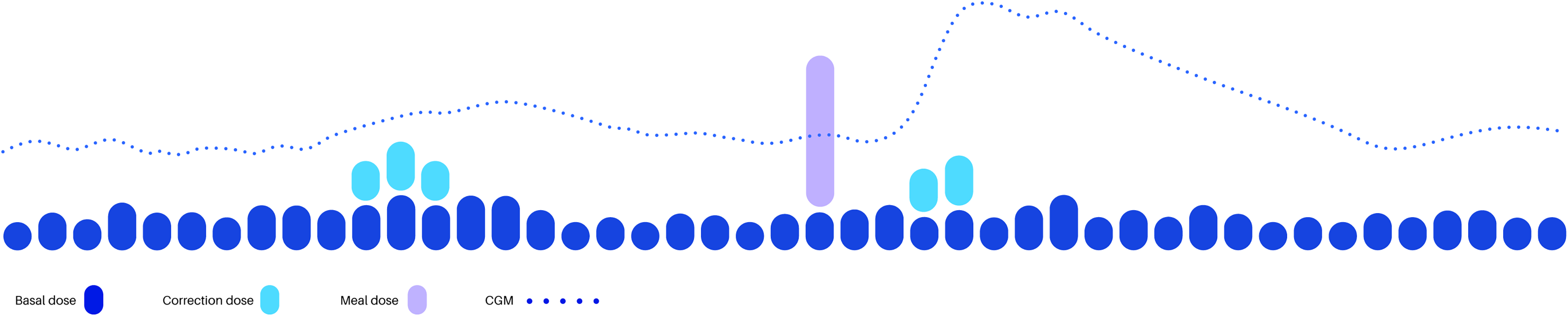
iLet Dosing Decision Software. CGM, continuous glucose monitoring.
If the apparent need for insulin decreases (e.g., a change in health condition resulting in increased insulin sensitivity, an increase in physical activity, or the effect of non-insulin medications), the insulin dosing aggressiveness will respond with relatively smaller doses. If the apparent need for insulin increases (e.g., a change in health condition resulting in decreased insulin sensitivity, a reduction in physical activity, the effect of non-insulin medications, or intercurrent illness), the insulin dosing aggressiveness will respond with relatively larger doses. The adaptation of meal doses is entirely separate from the adaptation of basal and correction insulin doses and is intended to track and continually update user insulin requirements around the three available meal types (breakfast, lunch, and dinner). Each algorithm references both historical and real-time data to determine dosing for the user. The basal and correction algorithms are most heavily influenced by the previous rolling 24 h. The meal dose algorithm references the insulin needs for meal announcements of each announcement type (breakfast, lunch, and dinner) over the last seven meal announcements of that type.
To fully remove the dosing decision burden from the end user in an insulin only AID system, it is important that the system receives high quality data to determine appropriate therapeutic dosing. For example, should a user experience a hypoglycemic event, it is important that the user recognizes the need to return to euglycemia versus hyperglycemia, as the latter could trigger correction insulin dosing and negatively impact learning in an autonomous system.
A case study (Fig. 2) demonstrates the importance of a fully adaptive system in times of rapidly shifting insulin needs.
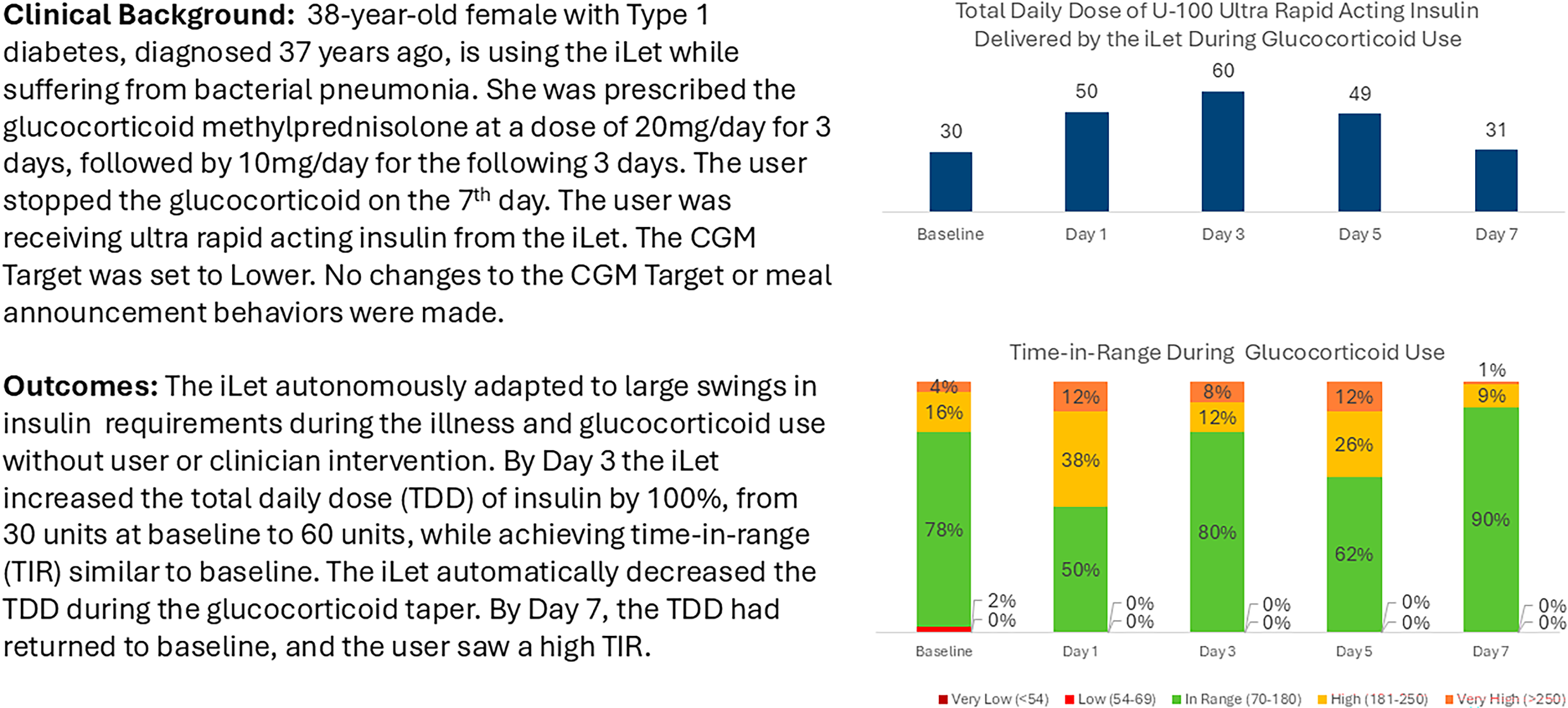
Case study illustration of total daily dose and time-in-range before, during, and after glucocorticoid use. CGM, continuous glucose monitoring; TDD, total daily dose; TIR, time-in-range.
Other systems differ from the iLet in their approach to glycemic management. Commercially available insulin delivery systems in the United States automate insulin differently and require somewhat different strategies for glycemic management versus a learning autonomous system. Systems such as the Insulet Omnipod 5 (Insulet Corporation, Acton, Massachusetts, United States), Minimed 780 g (Medtronic Diabetes Minimed, Northridge, California, United States), Tandem Control-IQ+ (Tandem Diabetes Care, Inc., San Diego, California, United States), and Sequel Twiist powered by the Tidepool Loop algorithm (Sequel Med Tech, Manchester, New Hampshire, United States) require clinicians to enter settings, either individually or through a setup wizard, such as basal insulin rates, insulin sensitivity factors, carbohydrate-to-insulin ratios, total daily insulin dose, or some combination of these. The systems can automate insulin delivery within set parameters around the static settings. For meals, the user is generally asked to enter an exact carbohydrate amount or a fixed carbohydrate amount so the system can calculate a bolus dose. Achieving glycemic goals may still rely on user-initiated correction boluses when hyperglycemia occurs. The static settings in these systems require intermittent adjustment by a clinician when the user’s insulin needs exceed the maximum ability of the system to adjust insulin delivery based on the system parameters. The degree of required adjustments varies by product. Some systems also have the capability of adjusting basal insulin dosing based on changes in the user’s total daily dose of insulin. Users can achieve glycemic goals by using any automated insulin delivery system, but the user and clinician experiences will differ depending on the amount of system interaction required by both the user and clinician to achieve those outcomes.
Initiating the System
Patient identification
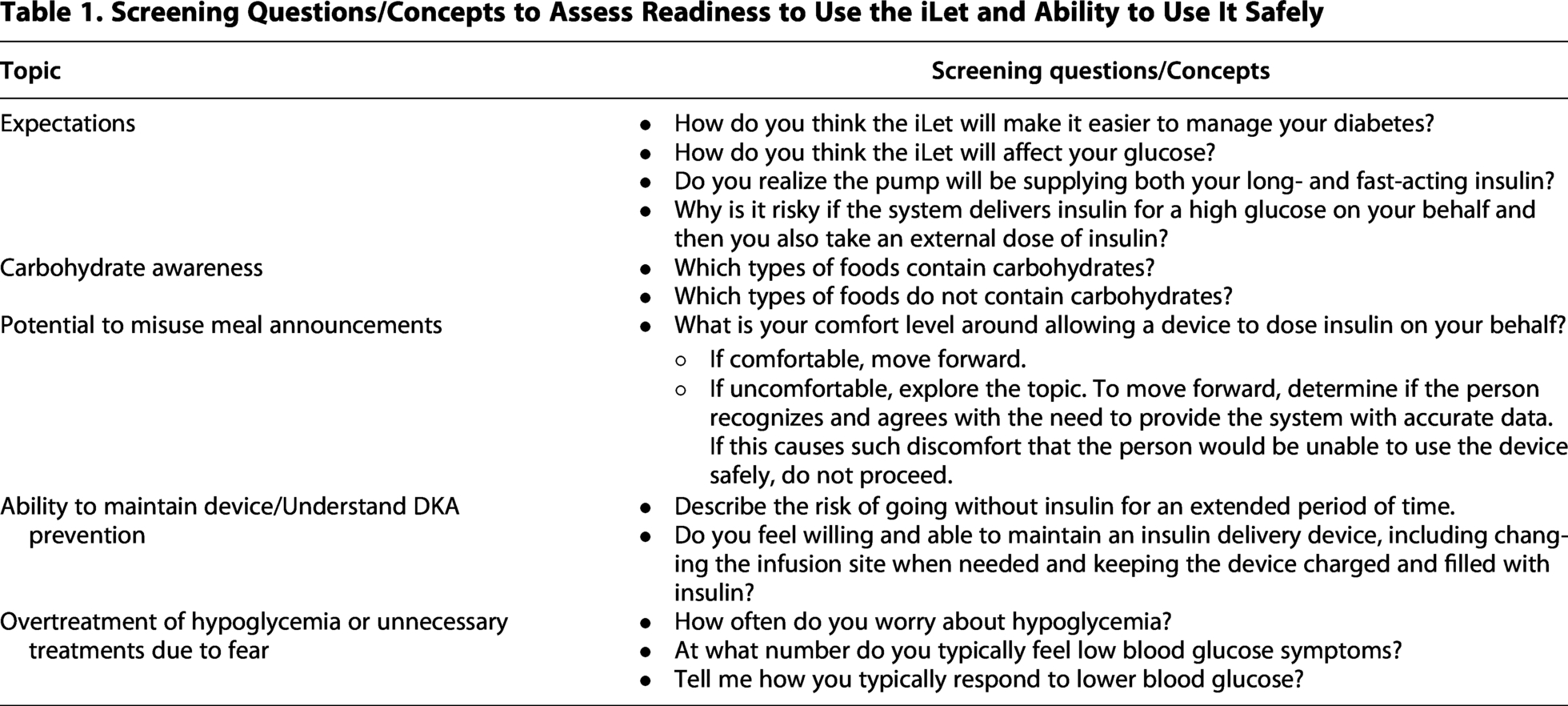
AID systems are recommended by the ADA as the preferred insulin delivery method over injections and other pump-based systems in people with diabetes, with early initiation of AID therapy noted to be beneficial. 3 Before initiating therapy, clinicians should confirm that individuals and their families clearly understand their responsibilities for safe device use. Screening questions support assessment of the patient’s and/or caregiver’s comprehension of the iLet system’s function, required maintenance, and safety considerations (Table 1). An essential learning objective is to facilitate understanding of the transition from manual diabetes management, or AID systems requiring more user/clinician interaction, to an adaptive system that learns from daily glucose patterns and responds to insulin needs in real time, relying on minimal user interaction.
Screening Questions/Concepts to Assess Readiness to Use the iLet and Ability to Use It Safely
Patient onboarding for success
When starting the iLet, the user should have a current body weight available. All device-related safety topics are addressed during initial training. In addition to device maintenance-specific topics, the user receives education on helping the system to efficiently adapt to their specific insulin needs.
For the first few days, users are instructed to eat meals that have their “Usual” amount of carbohydrate for each meal type and to announce them as “Usual for me.” The system will perform best if allowed the opportunity to fully adapt to the “Usual for me” amount of carbohydrate before the user begins to choose “More” or “Less” options (Fig. 3). During the initialization period, users should be advised to avoid impacting glycemia with snacks/meal announcements in the 4-h postprandial window. The meal algorithm has adapted to the appropriate dose once postprandial glucose values are at goal.
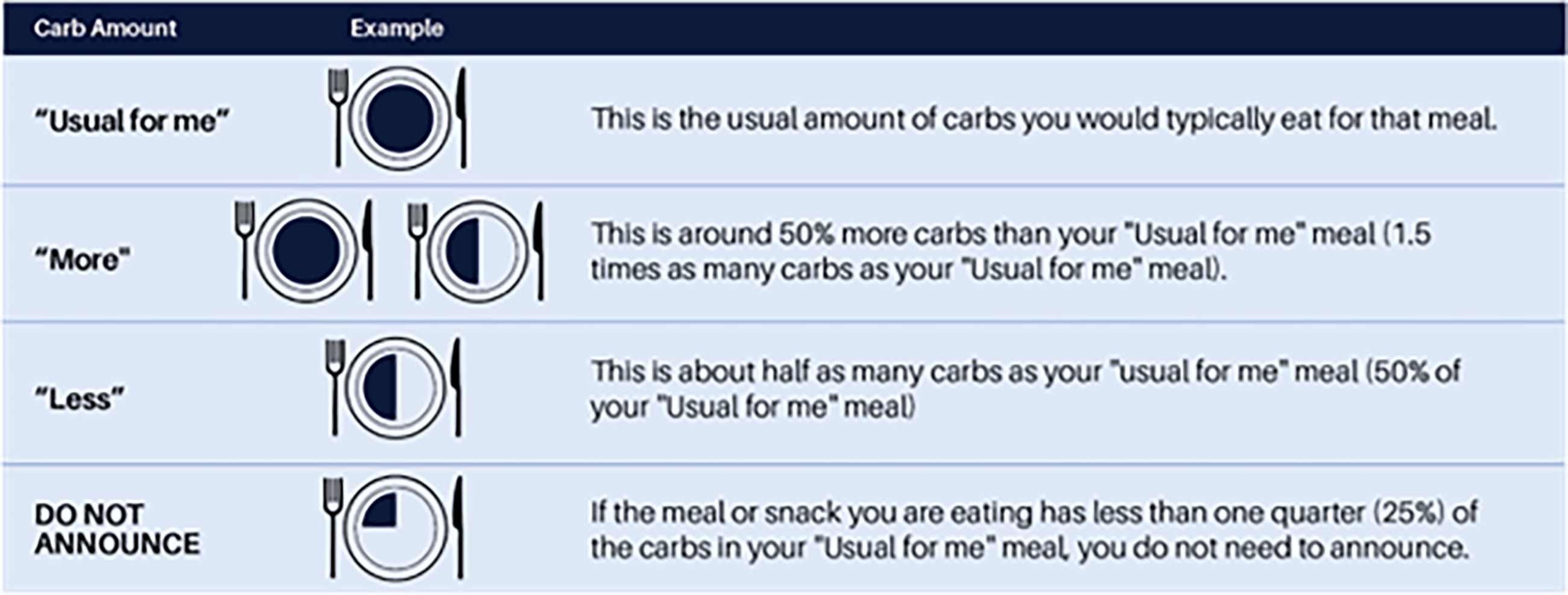
Meal announcement guidance.
Keys to Achieving Optimal Outcomes
Addressing dysglycemia through coaching and education
The continuous learning of an autonomous insulin dosing system adds importance to these key factors to managing glycemia: device/site maintenance, responding to alerts, and appropriate use of meal announcements. Addressing dysglycemia requires patient education rather than setting adjustments. The clinician must assess and address any gaps in these key factors. The clinician should use the Bionic Report to evaluate these three factors. The report provides an overview of glycemic outcomes, meal announcement us, and recent insights that can assist the clinician with identifying areas of success as well as behavioral education opportunities. During this time the clinician should also assess any diabetes distress signals that could impact outcomes and quality of life.
Device and site maintenance
All AID users must keep the device charged/powered, filled with insulin, and connected to CGM. It is also important to be sure the infusion site is viable. If the iLet loses connection with the CGM, the system will continue insulin delivery and only adjust basal or correction dosing if a blood glucose value is entered. Clinicians should instruct patients to request replacement sensors to retain for backup in the event a sensor fails or does not last its expected time frame. All AID users should be encouraged to proactively order supplies and carry back-up supplies. Counsel on tips for addressing skin problems or difficulty with keeping the sensor on, potentially using barrier preps, tackifiers, over-tapes, or adhesive remover wipes as necessary. Patients should be advised to change infusion sets every 2 to 3 days, or if suspected of being compromised, and to rotate sensor insertion sites (arms, hips, buttocks, abdomen). A compromised infusion site that is unaddressed could negatively impact learning in a system such as the iLet that uses historic data to adapt insulin dosing.
Responding to alerts
All iLet alerts and alarms are designed to be actionable to minimize alarm fatigue (Table 2). Accordingly, users/caregivers should be instructed not to turn off important alarms and to always respond to alerts/alarms indicated on the device. Caregivers can receive glucose alerts on accompanying applications. Advise avoidance of preventative hypoglycemia treatment, unless receiving a predicted low glucose alert. Since the iLet will suspend insulin delivery prior to/during hypoglycemia, smaller treatments are needed and the user should not use the pause feature as a way to treat hypoglycemia. As with all AID systems, the user should aim to return the glucose to euglycemia to avoid triggering any correction insulin related to overtreatment of hypoglycemia. If the iLet system is regularly influenced by unnecessary unannounced rapid acting carbohydrate consumption it could cause the system to deliver more insulin than the user truly needs.
Appropriate Responses to Glucose Alerts

CGM, continuous glucose monitor.
Appropriate use of meal announcements
Patients should be instructed to announce meals solely based on the carbohydrate amount of their meal/snack, not on protein, fat, or calorie content or the quantity of food. The carbohydrate amount is relative to each user and their eating habits. Clinicians should review the user’s eating history to identify the meals they eat most often for each meal type (“Usual for me” meals) as well as their level of carbohydrate awareness. “Usual” meals are foundational to the system’s meal adaptation (Fig. 3). The clinician can use the Bionic Report to assess the appropriate use of meal announcements by focusing on timing, size, frequency, and postprandial glycemia (Table 3).
Managing Meal Announcements

Meal adaptation applies across all dose sizes for a given meal type. When the system learns that a higher (or lower) dose is needed for that meal type, it automatically scales dosing and the “More” and “Less” doses will remain 50% more and 50% less than the “Usual” dose as the doses scale. If user behavior leads to inappropriate adaptation, a factory reset may be needed to restart learning (see Table 4).
Special Considerations for Managing Glycemia

CGM Targets and Special Considerations
After prioritizing patient education and proper system use, adjusting the CGM target can be considered to address dysglycemia. The Usual target (120 mg/dL) is recommended for most patients when starting. The Lower target (110 mg/dL) may be helpful during times of the day that meals are eaten. This can help reduce postprandial spikes by responding faster to a rise in glucose. Increasing the target may be helpful if there is a pattern of drifting overnight hypoglycemia. The higher target (130 mg/dL) is typically not necessary except in cases of extreme insulin sensitivity. Follow up is essential to assessing the appropriateness of the CGM target. Users consuming fewer carbohydrates, especially simple carbohydrates, typically achieve lower mean glucose levels than those with higher-carbohydrate diets. When users make major dietary changes, the iLet requires time to adapt to new meal patterns. 10
Table 4 outlines scenarios that require special consideration when managing glycemia for iLet users. The system’s ability to deliver all required correction insulin doses and to autonomously adapt changes the way clinicians should manage these scenarios for those on the iLet versus other AID systems. The guidance below is based on the iLet pivotal trial (exercise) and an understanding of how the system responds to changing glycemia and insulin needs. In the 2024 Position Statement, The Use of Automated Insulin Delivery Around Physical Activity and Exercise in Type 1 Diabetes, EASD and ISPAD recommend that iLet users reduce the meal announcement carbohydrate amount for meals consumed prior to physical activity. 19 This approach has not been formally studied, and the impact on the system’s meal adaptation should be considered as a glycemic excursion postprandially would prompt both correction insulin dosing and meal adaptation upward if using a “Less” announcement for what would normally be announced as a “Usual” carb amount. Additional research on the impact of autonomous insulin delivery in these scenarios is needed to develop more specific guidance.
Potential Barriers
Potential barriers to achieving optimal outcomes include the system’s dependence on continuous and accurate CGM data and the user’s ability to recognize when their symptoms do not match the CGM glucose. It is also critical for the user to maintain blood glucose monitoring supplies in the case of CGM unavailability. The system’s ability to learn from historical data allows for the optimization of insulin dosing. However, if the system is frequently provided with low-quality data related to the user’s attempts to override the autonomous dosing, the system’s learning and subsequently insulin dosing are compromised.
Other potential barriers include candidate selection. In addition to using the screening questions in Table 1, clinicians should consider the user’s ability to safely use the product. Anyone who cannot independently maintain and operate the device and has insufficient caregiver support should not be considered as a safe candidate for this technology. The initial learning phase can be a challenging experience particularly for those individuals who experience some level of anxiety as they relinquish management tasks to the system. If the individual will not be able to allow the system to correct glucose excursions at its measured rate but is compelled to intervene/override the system to return to euglycemia faster, they are likely not good candidates for the technology. The iLet is not indicated for use and has not been tested for use in certain populations such as pregnancy and those on hemodialysis. Other AID systems may be more appropriate for these populations. Successful use of any AID system requires assessing and addressing the social drivers of health.
Ongoing Implications for Clinical Practice
Expanding technology access to nontraditional candidates and prescribers
As noted, CGM systems and insulin pumps, in particular AID, are now recommended as the standard of care for all persons with T1D. 3 A serial, cross-sectional analysis of data from the Optum Labs Data Warehouse analyzed data from 186,590 youth and adults with T1D in the United States from January 1, 2009, to December 31, 2023. A rapid increase in the use of diabetes technology and notable improvements in glycemia among youth and adults were reported during the 15 years studied, however, the prevalence of achieving glycemic targets remained low, and racial, ethnic, and socioeconomic differences grew over time. The prevalence of achieving glycemic targets and the use of diabetes technology were lowest in Hispanic, non-Hispanic Black, and Medicaid-insured youths and adults with the differences persisting or even increasing over time. 20 A systematic review of observational studies published between 2017 and 2024 reported significant differences in diabetes technology prescription and use by race/ethnicity, with White non-Hispanic patients having the highest prescription rates (average 56.3% [range 12%–79%]), followed by patients that identify as Hispanic (average 28.8% [range 4%–76%]), and then Black (average 21.3% [range 3%–52%]). 21
With the iLet’s capability to provide substantial, rapid improvements in glycemia without increasing the risk of hypoglycemia, including in those with high baseline A1C levels and across racial and socioeconomic backgrounds, 12 it has the potential to serve as a powerful public health intervention, including among high-risk, underserved populations.10,22 Significant barriers remain to widespread implementation, including cost, insurance coverage, digital access, supply maintenance, and the availability of longitudinal support for underserved populations.
The reduction in burden for the user potentially makes the system more accessible to a broader population, including those who struggle with the complexities of insulin management, including carbohydrate counting. Those capable of insulin management but experiencing burnout are potential candidates if they are willing and able to allow the system to assume their glucose management, which may involve more deliberate relinquishing of closely held personal control for some people more than for others. The reduced user interaction compared with other systems may lead to AID adoption by a wider range of persons with type 1 diabetes10,13,22 and be able to be deployed by a broader spectrum of clinicians including primary care, 23 thus helping to address disparities in technology adoption and outcomes.24–28
AID systems are typically provided in the endocrinology clinic due to the intensive setup and programming required and the need for trained staff and adequate time and resources for ongoing support of most systems. However, three out of four counties in the United States do not have endocrinologists practicing within their borders. Around half of adults with type 1 diabetes rely on primary care for diabetes management. 29 It is vital to be able to offer technology including AID in primary care to meaningfully expand technology access for people with type 1 diabetes regardless of where they live. A randomized clinical trial including 40 subjects with type 1 diabetes compared deployment of the fully adaptive iLet in primary care versus endocrinology and in-person versus virtually. Of the participants, 97% achieved an average glucose < 183 mg/dL, representing an A1C level < 8%, while 64% achieved an average glucose < 154 mg/dL, representing an A1C level < 7%. An overall average glucose reduction of 17 mg/dL and a time-in-range increase of 11% with no change in sensor-measured hypoglycemia using iLet compared with usual care was reported. Similar outcomes were seen between initiation in endocrinology versus primary care or in-person versus virtual care. 23 A larger trial is currently enrolling. Trial designs such as this should be considered for other automated insulin delivery systems.
The evolving role of the clinician
As clinicians transition from manual settings adjustments as a primary focus of care to guiding patients in effective use of autonomous insulin delivery systems, they must embrace the reduced need for clinician intervention that these systems both allow and require for optimal performance. Clinical focus should shift toward supporting patient–system interactions and reinforcing appropriate behaviors related to when and how to engage with the system. This approach can improve time-in-range from baseline without increasing time-below-range. It may involve redefining success for each individual, achieving an acceptable level of glycemic management for the individual with less effort while improving the quality of life. 30 It is essential to set realistic expectations and to emphasize both the glycemic benefits and reduced treatment burden, while acknowledging that relinquishing direct control over insulin dosing may initially feel uncomfortable for both clinicians and patients who are historically accustomed to a high level of control over insulin dosing. 31 The clinician’s role shifts to explaining how user–system interactions affect glycemia and safety, including downstream effects on algorithm adaptation beyond the user’s immediate intent, and to guiding patients toward safer strategies to achieve desired outcomes.
This is a partnership between the patient and the device, not a handoff. It requires learning how to share control safely. With less time required during clinical encounters to adjust insulin dosing, more time can be devoted to assessing and addressing psychosocial issues or other aspects of care. The clinical encounter is focused on the individual and their experience rather than settings and numbers.
Since ongoing adjustment of insulin therapy settings is not required with the iLet system, the diabetes care and education specialist (DCES) can play an expanded role in the ongoing management of the system in partnership with the user. Prescriptive authority is not required for providing the education regarding dosing behaviors that influence the functioning of the adaptive closed-loop algorithms. The DCES can shift from teaching advanced carbohydrate counting and math skills to person-centered conversations focusing more on healthy food choices and activity as part of an overall healthy lifestyle. This potentially opens mental space to problem-solve other aspects of diabetes management and potentially lessens the risk of maladaptive eating behaviors or eating disorders. 32 Precise carbohydrate counting is helpful with some AID systems to optimize glycemic outcomes. There are additional strategies, such as fixed carbohydrate entry, that could simplify the process of meal dosing, but this still requires numeracy skills. It is recognized that various methods for teaching simplified carbohydrate counting have been used over the years. 33 The iLet allows for a simplified approach, requiring only carbohydrate awareness for its qualitative meal announcements.
Clinicians must adopt a broader, person-centered definition of success. While A1C remains a valuable metric, it should be complemented by time-in-range, glycemic variability, and person-reported outcomes such as treatment satisfaction, perceived burden, and quality of life. For many patients, success may mean fewer interruptions in daily life, less cognitive load, and reduced diabetes distress, even if glycemia is stable rather than improved. This approach allows clinicians to align care goals with what matters most to patients, promoting sustained use and trust in the technology as well as engagement with their self-management.
Conclusion
As automation advances, there is a need for targeted professional development to equip clinicians with the knowledge and confidence to support users effectively. As the clinical role shifts from manual insulin titration to interpreting device outputs and supporting behavioral adaptation, clinicians will need training in understanding how user input, daily routines, and life contexts influence algorithm performance and glycemia. Training must extend beyond technical operation and include strategies for expanding technology access to a broader population, expectation-setting, and addressing psychosocial dimensions such as trust in automation and shifting roles in self-management.
There are research gaps to be addressed, including the long-term glycemic outcomes and use in physical activity. Additional topics could include the sustainability of behavioral engagement, the impact on diabetes distress, quality of life over time, disordered eating, and caregiver burden across different life stages. Data on real-world access, use, and outcomes in diverse populations, including those with limited health literacy or numeracy, mental health conditions, or historically marginalized backgrounds, are needed. Integration of AID into broader models of diabetes care is essential for scalability and sustainability. This includes aligning with primary care workflows and leveraging digital health platforms and virtual coaching to provide longitudinal support.
Research is currently underway to explore the use of autonomous insulin dosing in those with cystic fibrosis, pregnancy, and for a longer duration than previously studied in primary care. Device manufacturers and academia continue efforts to optimize algorithm functionality. The future of AID will be impacted by artificial intelligence and improvements in the field of sensing, including but not limited to the dual sensing of glucose and ketones. Future systems may also incorporate additional drug delivery options, such as glucagon. 7 Wearability and form factor improvements continue to evolve as well. All of these advancements should lead to a better future for people living with diabetes and those that care for them.
Authors’ Contributions
All authors contributed substantially to the design of the work and critical review and revision of the work to a finalized version. All authors approved the final version of the article.
Footnotes
Acknowledgments
Medical writing support was provided by Janice MacLeod, Janice MacLeod Consulting.
Author Disclosure Statement
I.B.H. has a research grant from Sequel Medical Technology and receives consulting funds from Abbott, Roche, and Hagar. D.I. is a speaker/consultant for Dexcom, Abbott, Medtronic, Insulet Corporation, Tandem, Beta Bionics, Novo Nordisk, Lilly, Sanofi, Sequel Medical Technology. P.M. has received honoraria for serving on advisory committees for Novo Nordisk, Biomea Fusion, Dexcom, Insulet, Medtronic, Abbot, and speaking fees for Novo Nordisk, Eli Lilly, Dexcom, Insulet, Medtronic, Abbot, and Beta Bionics. S.M.O.’s institution has received research support from the Helmsley Charitable Trust, Dexcom, Abbott Diabetes, Insulet, and Sequel Medical Technology, as well as honoraria for consulting from Dexcom and Insulet. V.N.S.’ institution has received research support from Dexcom, Eli Lilly, Enable Bioscience, Zucara Therapeutics, DEKA research, Cystic Fibrosis Foundation, Breakthrough T1D and NIH. V.N.S. has received honoraria for speaking, consulting or advising from Sanofi, NovoNordisk, Eli Lilly, Dexcom, Insulet, Tandem Diabetes Care, Sequel Medical Technology, Biomea Fusion, Roche, Abbott Diabetes, and T1D Scout; outside of this submitted work. B.S. has received speaking fees from Insulet Corporation, Beta Bionics, and Medtronic. B.S. has received fees for patient training from Beta Bionics, Insulet Corporation, Medtronic, and Tandem. K.W. has received speaking honoraria from Beta Bionics. K.P.C. is an employee and stockholder of Beta Bionics. J.M. is a consultant with Beta Bionics. S.R. is an employee and stockholder of Beta Bionics.
Funding Information
There was no funding for this work. Article processing charges for open access were paid by Beta Bionics (Irvine, CA).