
Abstract
Infant mortality is a key indicator of population health and health system performance. This national study analyzed infant mortality in Mexico, examining temporal trends, leading causes of death, territorial inequalities, and indicators of surveillance quality. Using official mortality microdata for 224 212 deaths, we assessed patterns by cause of death, sex, health system affiliation, city size, and state of residence. Infant mortality remained largely stable during the study period (10.7 per 1000 live births in 2014 to 10.6 in 2023), despite an increase in reported medical attendance at death to 99.5% in 2023. Neonatal conditions including respiratory disorders, sepsis, prematurity, and congenital heart malformations accounted for most deaths. Territorial gradients were evident: smaller localities had lower probabilities of medical attendance and autopsy performance and higher proportions of deaths recorded as presumed external causes. Nearly 88% of infant deaths occurred among infants without social security affiliation, highlighting persistent inequities.
Keywords
Introduction
Infant mortality, conventionally defined as the death of a child before reaching 1 year of age, remains a central indicator of population health, health system performance, and social development. 1 Because survival in the first year of life depends on conditions operating before conception, throughout pregnancy, at birth, and during early infancy, infant mortality reflects not only biomedical risk but also the capacity of health systems to deliver timely, continuous, and equitable care to mother–newborn dyads.
Infant mortality cannot be fully understood without situating it within the perinatal continuum. Perinatal mortality (encompassing late fetal deaths and early neonatal deaths) shares many determinants with infant mortality and represents an upstream window where failures in antenatal care, intrapartum management, and immediate postnatal support have lasting consequences for survival in the first year of life. 2 Evidence from Latin American settings indicates that prematurity, neonatal sepsis, congenital anomalies, and birth asphyxia dominate both perinatal and infant mortality profiles, underscoring the biological and system-level continuity between these outcomes. This continuity highlights the need to analyze infant mortality as a downstream manifestation of maternal and perinatal care performance rather than as an isolated pediatric endpoint.
Maternal health and maternal care represent critical upstream determinants of infant survival. Conceptual and empirical work emphasizes that maternal and infant health are inseparable, with inadequate antenatal, intrapartum, and postpartum care increasing risks of prematurity, low birth weight, neonatal infection, and early infant death. 2 Recent evidence from Mexico shows that inequities in effective maternal care, particularly among Indigenous women and those without social security, are driven by structural discrimination and system-level barriers, and that these inequities extend into early infant outcomes.3,4 These findings reinforce the importance of linking maternal, birth, and infant data to identify preventable pathways to infant death.
Health system organization also plays a critical role in shaping infant mortality patterns. A growing body of literature demonstrates that expanded health coverage, defined as increased insurance enrollment or formal eligibility for health services, does not necessarily translate into effective access to timely and high-quality care or into improved infant survival. 5 Similar patterns have been documented in Latin America, where reductions in infant mortality have not consistently been accompanied by decreases in health inequities, particularly in countries characterized by segmented or fragmented health systems. 6 These findings suggest that increases in service utilization or facility density alone are insufficient to reduce infant mortality when continuity of care, service quality, and coordination across levels of care remain limited.7,8 In countries with fragmented health systems, reductions in infant mortality have not always been accompanied by reductions in health inequities.9 -11
Beyond the organization of health services, social and geographical determinants strongly shape infant survival. Multilevel analyses demonstrate that infant mortality is influenced by cumulative exposures across households, neighborhoods, communities, and institutions, including education, income, housing conditions, and access to basic services. 12 Place-based disadvantage has been shown to exert an independent effect on infant mortality even after accounting for individual and healthcare-related factors, supporting the need for subnational and city-level analyses. 13 Housing instability and poor living conditions represent additional upstream mechanisms through which social inequality influences infant survival. 14
In Latin America, urbanization has not uniformly conferred a survival advantage for infants. Analysis of 286 cities across 8 countries demonstrates substantial intra-urban heterogeneity in infant mortality, with many large cities exhibiting outcomes comparable to or worse than rural areas despite higher infrastructure density. 13
Primary health care (PHC) has emerged as a key protective factor against infant and child mortality in the region. Longitudinal, multicountry evidence shows that higher PHC coverage is associated with significant reductions in infant, post-neonatal, and under-five mortality, particularly for causes sensitive to prevention and early management, such as respiratory and infectious diseases. 15 Importantly, these effects persist after adjustment for poverty, inequality, water and sanitation, and hospital density, highlighting PHC as a central mechanism through which health systems can reduce preventable infant deaths.
The present study analyzes national infant mortality data in Mexico between 2014 and 2023, examining temporal trends and state-level variation in mortality rates, leading causes of death, and healthcare-related characteristics of recorded deaths. By integrating cause-of-death profiles with indicators of access, medical attendance at the time of death, and contextual inequities, this work aims to identify persistent structural and system-level determinants of infant mortality and to inform strategies for reducing avoidable infant deaths within a fragmented health system.
Methods
Study Design and Data Source
This study was a retrospective, population-based analysis using national vital statistics from the National Institute of Statistics and Geography (INEGI). The INEGI system captures deaths occurring both within and outside health facilities, including those at home that are subsequently certified through the national death registration system. The study population comprised all registered deaths of infants younger than 12 months in Mexico between 1 January 2014 and 31 December 2023, regardless of place of death or health system affiliation. Annual infant mortality rates were calculated using official live birth data reported by INEGI as denominators. Records with missing or implausible age at death were excluded. The final analytical dataset comprised 224 212 infant deaths.
Outcome Variables
The primary outcome was infant mortality, defined as death occurring before 365 days of life. Underlying causes of death were coded according to the International Classification of Diseases, 10th Revision (ICD-10).
For descriptive and comparative analyses, causes of death were grouped into clinically and epidemiologically meaningful categories based on frequency and relevance to preventable and care-sensitive conditions. These included:
Respiratory disorders of the newborn
Neonatal bacterial sepsis
Prematurity and low birth weight
Birth asphyxia
Congenital heart malformations
Other infectious causes (eg, pneumonia and diarrheal disease)
These groupings were used to characterize national patterns and subnational variation in leading causes of infant death.
Sociodemographic and Territorial Variables
The following characteristics recorded on the death certificate were analyzed:
Sex (female or male)
Age at death
Year of death
State of residence (32 federal entities)
City of residence, used to derive measures of territorial context. Territorial classification was based on the city of residence recorded in the death certificate rather than the location of the health facility where death occurred.
Health system affiliation, categorized as with or without social security coverage
Urban–Rural Classification
Urban and rural residence was not available as a binary variable in the mortality records. Therefore, an urban–rural classification was derived from city population size, using official thresholds established by the National Institute of Statistics and Geography (INEGI). Localities with fewer than 2500 inhabitants were classified as rural, while those with 2500 inhabitants or more were classified as urban.
To capture territorial heterogeneity beyond a simple dichotomy, city size was additionally examined using disaggregated categories (<2500; 2500-14 999; 15 000-99 999; and ≥100 000 inhabitants). These categories were used to explore gradients in access to care, health system performance, and surveillance quality. When appropriate for interpretation, categories were grouped into rural versus urban areas.
Health Care-Related Variables
To assess health system performance and characteristics of mortality surveillance, we analyzed the following variables recorded on the death certificate:
Medical attendance at the time of death (yes/no)
Place of death (health facility vs non-facility)
Autopsy performed (yes/no)
Medical attendance at the time of death does not indicate the duration, quality, or completeness of clinical care. It may include cases in which the infant arrives in critical condition, is declared dead shortly after arrival, or dies immediately upon entering a health unit. This variable reflects the context of death certification rather than the quality or timeliness of care received prior to death, as deaths attended by health professionals are more likely to receive medically certified causes of death. 16
These variables were examined descriptively and in relation to city size and state-level patterns as indicators of effective access, continuity of care, and quality of death certification, rather than as measures of individual clinical decision-making.
Finally, presumed external causes refer to deaths recorded on death certificates as involving suspected violence, accidental injury, or self-inflicted harm affecting either the infant or the mother; these records do not represent confirmed forensic diagnoses.
Infant Mortality Rates
Annual infant mortality rates (IMR) were calculated as the number of infant deaths per 1000 live births, using official live birth estimates as denominators. Rates were estimated at the national level and by state to assess temporal trends and subnational heterogeneity between 2014 and 2023.
Statistical Analysis
All analyses were performed using Stata version 19.5 (StataCorp, College Station, TX). We first conducted descriptive analyses, reporting absolute frequencies and percentages for categorical variables and identifying the leading causes of infant death overall and by sex. Associations between city size and mortality surveillance indicators were examined using linear probability regression models with robust standard errors, with city population size modeled as a continuous predictor.
Temporal trends in infant mortality rates were examined descriptively across the study period. Geographic variation was explored through state-level comparisons and analyses by city size. Differences in health care-related variables (such as medical attendance at the time of death and autopsy performance) were assessed across rural and urban areas and across city size categories.
Given the descriptive and health-systems-oriented objectives of the study, analyses focused on stratified and comparative patterns rather than causal inference or multivariable modeling.
Data Quality Considerations
Indicators of data quality and surveillance performance were explicitly examined, including the frequency of non-specific or residual ICD-10 codes (commonly referred to in mortality surveillance literature as “garbage codes”) which reduce the epidemiological usefulness and comparability of cause-specific mortality statistics (16).
The frequency of non-specific or residual ICD-10 codes
The underuse of autopsy, including among deaths with recorded aggression or injury
Internal consistency between reported medical attendance at death and place of death
These elements were incorporated into the interpretation of findings as potential sources of misclassification or underestimation of preventable causes of infant death.
Ethical Considerations
This study used publicly available anonymized secondary data from the national vital statistics system maintained by the National Institute of Statistics and Geography (INEGI). The study protocol was reviewed and approved by the Institutional Review Board and exempted from informed consent.
Results
Overall Infant Mortality and Temporal Trends
Between 2014 and 2023, a total of 224 212 infant deaths were registered in Mexico. At the national level, the IMR showed minimal variation across the study period, remaining essentially stable. In 2014, the IMR was 10.72 deaths per 1000 live births, compared with 10.62 deaths per 1000 live births in 2023, representing an absolute change of 0.10 deaths per 1000 live births over the decade. Although modest year-to-year fluctuations were observed, no sustained downward trend was evident during the study period.
The proportion of infant deaths with reported medical attendance at the time of death increased modestly over the study period. In 2014, 86.5% of infant deaths were reported as having received medical attendance, and this proportion remained relatively stable through 2020. After 2020, the proportion increased slightly, reaching 88.4% in 2021 and 88.1% in 2022. In 2023, a marked increase was observed, with 99.5% of infant deaths reported as having received medical attendance at the time of death.
Sex Distribution
Across the entire period, male infants accounted for a higher proportion of deaths than female infants. This pattern persisted after accounting for differences in the number of live births by sex. Male excess mortality was observed consistently across years and across most causes of death.
Leading Causes of Infant Death
The distribution of causes of infant death was dominated by neonatal and perinatal conditions, many of which are considered preventable or care sensitive. The 5 leading causes of death accounted for approximately 39% of all infant deaths during the study period and included (1) Respiratory disorders of the newborn, (2) Neonatal bacterial sepsis, (3) Congenital heart malformations, (4) Prematurity and low birth weight, and (5) Birth asphyxia. The main causes and their frequencies are presented in Table 1. External causes of death were also recorded and are defined as deaths recorded as involving suspected violence, accidents, or self-inflicted injuries, affecting either the infant or the mother, without forensic confirmation.
Leading Causes of Infant Mortality in Mexico, 2014 to 2023 (n = 224 212).

Footnotes. Percentages are calculated using the total number of infant deaths registered between 2014 and 2023 (n = 224 212). Causes of death were grouped according to ICD-10 categories. Male excess mortality was observed across all listed causes. Remaining causes (not shown) accounted for 40.1% of infant deaths.
Most leading causes listed in Table 1 occur primarily during the neonatal period, reflecting the predominance of perinatal conditions in infant mortality. Additional frequent causes included pneumonia (organism unspecified), neonatal aspiration syndromes, congenital pneumonia, sudden infant death syndrome, and diarrhea and gastroenteritis of presumed infectious origin. Infectious causes (both neonatal and post-neonatal) accounted for approximately 21% of infant deaths.
Health System Affiliation
A large majority of infant deaths occurred among infants without social security coverage, representing approximately 88% of all deaths during the study period. This distribution remained relatively stable across years and across federal entities.
Urban–Rural Differences and City Size
When residence was classified using the urban–rural definition derived from city population size, no substantial differences were observed in the overall proportion of deaths receiving medical attendance at time of death between urban and rural areas.
However, analyses by city size categories revealed a clear gradient. Infant deaths occurring in smaller localities were less likely to have received medical attendance at the time of death compared with those occurring in larger localities. This inverse association between city size and medical attendance was consistent throughout the years.
Association between city size and health care-related characteristics. Regression analyses examining the association between city size and health care-related and surveillance characteristics of infant deaths demonstrated consistent territorial gradients.
Larger city size was positively and significantly associated with the likelihood of receiving medical attendance at the time of death (β = .02; SE = 0.01; P = .011; 95% CI: 0.00-0.03).
Similarly, city size was positively associated with autopsy performance (β = .05; SE = 0.02; P = .005; 95% CI: 0.02-0.09).
In contrast, city size showed a negative association with deaths recorded as involving presumed external causes (β = −.02; SE = 0.01; P = .057; 95% CI: −0.04 to 0.00), indicating a tendency for such deaths to be more frequently recorded in smaller localities, as presented in Table 2.
Association Between City Size and Health Care-Related and Surveillance Characteristics of Infant Deaths, Mexico 2014 to 2023.
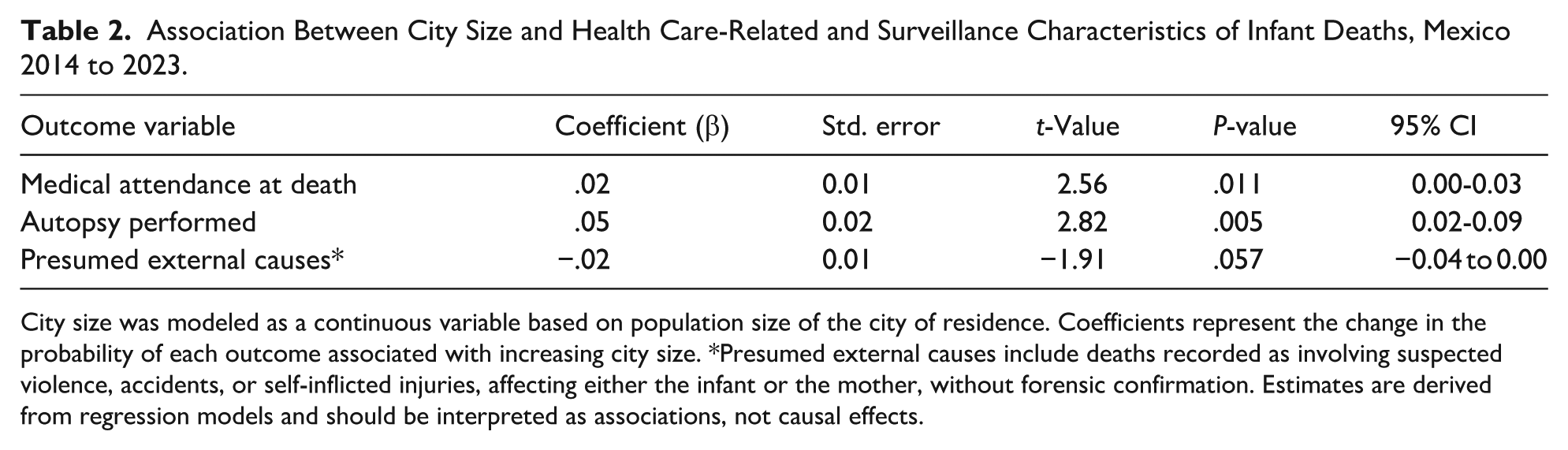
City size was modeled as a continuous variable based on population size of the city of residence. Coefficients represent the change in the probability of each outcome associated with increasing city size. *Presumed external causes include deaths recorded as involving suspected violence, accidents, or self-inflicted injuries, affecting either the infant or the mother, without forensic confirmation. Estimates are derived from regression models and should be interpreted as associations, not causal effects.
Monthly Variation in Infant Mortality
Incidence rate ratios (IRR) were estimated to assess monthly variation in infant mortality, using January as the reference month (IRR = 1.00). Monthly fluctuations were modest, with no clear evidence of pronounced seasonality. December showed a slightly higher incidence of infant deaths compared with January (IRR = 1.09).
Geographic Variation by State
Substantial state-level heterogeneity was observed in IMR and across all indicators. Higher IMR were found in states of the north (Chihuahua, Coahuila and Tamaulipas), center (Mexico City and State of Mexico) and south east (Campeche y Tabasco) of the country. Some states exhibited higher proportions of medical attendance and autopsy performance than others, even when contrasted with Mexico City, which concentrates a large share of the country’s health infrastructure (Figure 1).
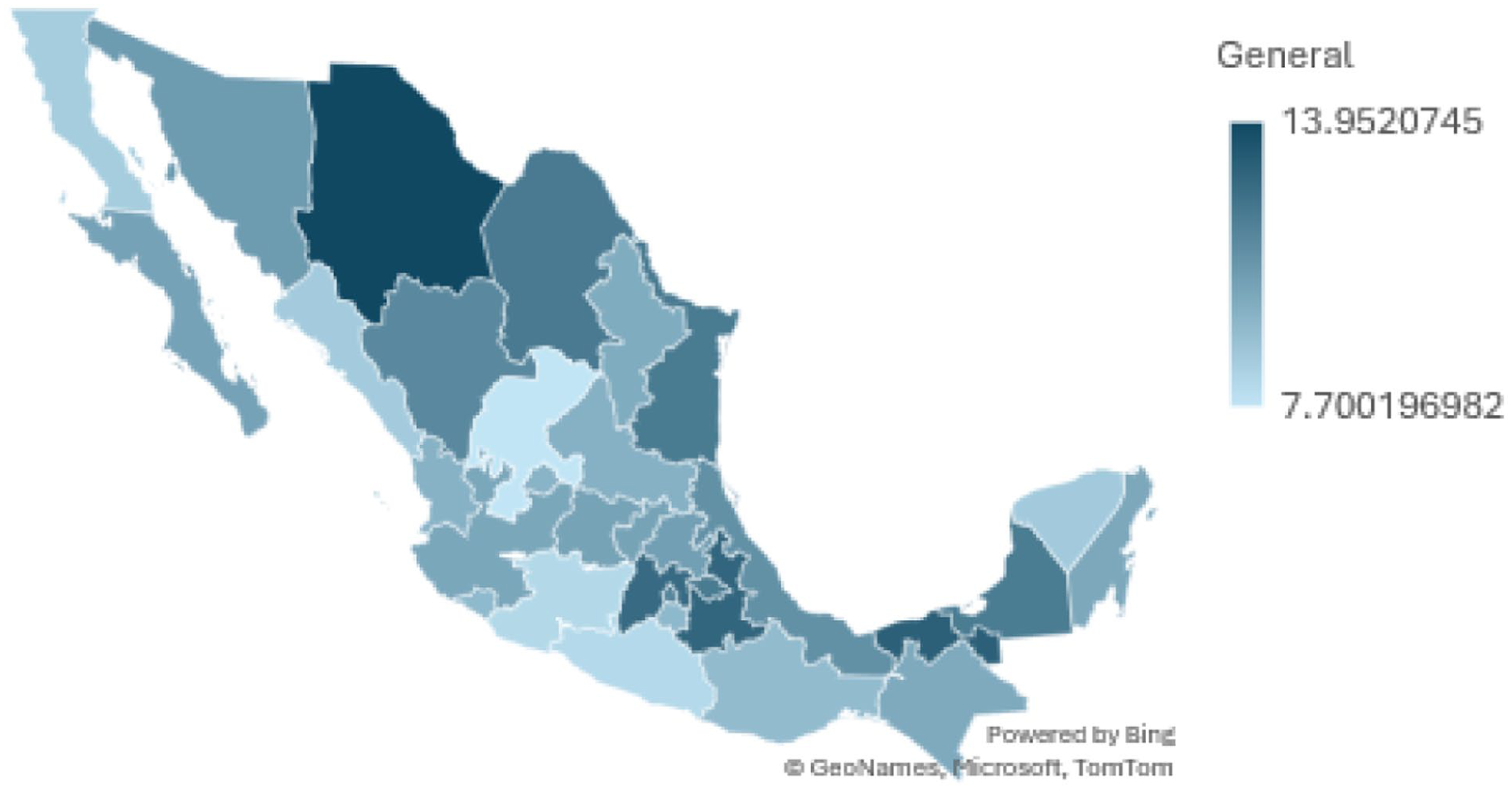
Spatial distribution of cumulative infant mortality rates across Mexican states, 2014 to 2023. Spatial distribution of infant mortality rates by state in Mexico from 2014 to 2023. Differences across federal entities reflect territorial inequities in effective access to maternal and infant health services and mortality surveillance.
Several states achieved higher levels of medical attendance at the time of death and autopsy use than Mexico City, despite having fewer health facilities. This pattern suggests that differences in infant mortality and surveillance quality reflect effective access and system organization rather than simple availability of services.
Diagnostic Specificity
Across the dataset, a high frequency of non-specific ICD-10 codes was observed, particularly for infectious and respiratory causes. This pattern was more pronounced in smaller localities and in states with lower autopsy performance, indicating potential misclassification of causes of death and underestimation of preventable conditions.
Discussion
We have presented a nationwide analysis of infant mortality in Mexico between 2014 and 2023, and consistent with prior evidence from Latin America and other middle-income settings, infant deaths were concentrated in neonatal and perinatal causes that are largely preventable or care-sensitive. According to global patterns described in the UN IGME 2024 Levels & Trends in Child Mortality Report, Mexico occupies an intermediate position globally in infant mortality according to the UN IGME report which also documents continued declines in several LMICs in South Asia and sub-Saharan Africa following investments in neonatal care, maternal health, and community-based interventions. 17
The findings of this study are consistent with those reported by Milán et al regarding the importance of strengthening the perinatal continuum which may potentially reduce both fetal deaths and the neonatal conditions that account for a large share of infant mortality. Recognizing infant mortality as a downstream indicator of perinatal system performance may therefore facilitate more effective, integrated interventions. 18
One notable finding is the absence of a sustained decline in infant mortality during the study period, suggesting that increases in nominal coverage or service contact may not necessarily translate into reductions in infant mortality. Similar discrepancies between coverage expansion and mortality outcomes have been documented in both high-income and middle-income settings, underscoring the limitations of access-based indicators as proxies for effective care. 19 The sharp increase in reported medical attendance at the time of death in 2023 (99.5%) should be interpreted with caution, as this abrupt change is unlikely to reflect a true and immediate expansion in access. Instead, it may be associated with changes in administrative processes within the national vital statistics system. Improvements in certification completeness or shifts in classification criteria could artificially inflate the proportion of deaths recorded as medically attended.
In Latin America, Maceira et al demonstrated that declines in infant mortality have not been uniformly accompanied by reductions in inequities, particularly in countries with segmented health systems. Their findings suggest that improvements in aggregate indicators may conceal persistent subnational disparities and uneven gains across populations, but this regional pattern supports the interpretation that health system organization and integration, rather than service availability alone, are critical determinants of infant survival. 7
The predominance of neonatal and perinatal conditions (such as respiratory disorders of the newborn, neonatal sepsis, prematurity, and birth asphyxia) mirrors patterns described in settings where failures occur earlier in the continuum of care, during pregnancy, delivery, or immediate postnatal management.20 -22 Evidence from Mexico indicates that inequities in effective maternal care persist even in the context of expanded coverage, with structural barriers and discrimination limiting timely and high-quality care for vulnerable populations. 23
The absence of a clear downward trend in infant mortality is also consistent with global analyses showing that middle-income countries have experienced slower and more heterogeneous declines in infant mortality compared with high-income countries, particularly during periods of health system stress or transition. 2
Finally, the limited seasonal variation observed in infant mortality in our analysis contrasts with patterns expected if short-term environmental or infectious exposures were the primary drivers. This finding is concordant with studies emphasizing that structural determinants play a larger role in shaping infant mortality than seasonal fluctuations.14,19
A second major contribution of this study is the identification of systematic territorial inequities in infant mortality–related indicators, revealing that city size functions as a structural determinant of effective access and surveillance capacity. This pattern aligns closely with evidence from Latin America demonstrating that urban residence does not guarantee protection and that substantial heterogeneity exists within and across cities. Ortigoza et al 13 showed that many large Latin American cities exhibit infant mortality rates comparable to or worse than rural areas, despite greater infrastructure density, suggesting the presence of intra-urban and peri-urban “care deserts” embedded within ostensibly well-resourced regions. In these studies, neighborhood context shapes early-life outcomes in ways that are not captured by national averages or facility counts. Our results may possibly suggest that similar mechanisms operate in Mexico, where infants in smaller localities face compounded disadvantages across care provision and mortality investigation.
We found that several states achieved higher levels of medical attendance at the time of death and autopsy performance than Mexico City. This observation resonates with regional analyses showing that segmented health systems can produce uneven outcomes even within countries that have expanded coverage. 8
The association between smaller city size and higher recording of presumed external causes raises additional concerns about child protection, rights and accountability in territorially disadvantaged settings. While these records do not represent confirmed violence, their concentration in smaller localities suggests environments where prevention, timely response, and postmortem investigation may be weaker. Similar concerns have been raised in reviews emphasizing the role of social and institutional contexts in shaping preventable infant deaths. 14
Together, these findings support reframing infant mortality in Mexico as a problem not solely of national policy or aggregate coverage, but also of territorial organization and governance. Strengthening infant survival will require interventions that explicitly address city-level and cultural barriers, improve integration across institutions, and ensure that primary, perinatal, and forensic services are equitably distributed. In this context, autopsy can reveal previously unsuspected diagnoses (such as pulmonary hemorrhage, infectious diseases, or genetic conditions) that may inform preventive strategies.22,23 Conversely, evidence suggests that weak postmortem investigation undermines prevention efforts by obscuring causal pathways and limiting the ability of health systems to learn from fatal outcomes. 3 Similar concerns have been raised in analyses of social determinants of infant mortality, which highlight that environments characterized by poverty, limited institutional capacity, and weak intersectoral coordination are more likely to experience both higher exposure to injury risks and lower investigative capacity. 11 In such contexts, infant deaths that warrant closer scrutiny may instead be inadequately documented, reducing opportunities for prevention and accountability.
These patterns also align with broader evidence on health system fragmentation in Latin America. Maceira et al 7 described how segmented systems often fail to ensure continuity between health care, forensic services, and social protection mechanisms, particularly for populations outside formal social security schemes. Place-based analyses from other settings have shown that neighborhood and territorial disadvantage shape not only health outcomes, but also the likelihood that deaths are adequately investigated and classified. 9
Limitations
The analysis relies on death certificate data, which are subject to misclassification and variability in reporting practices across regions. Information on medical attendance at the time of death does not allow an inference of the resources and infrastructure in the health unit assisting at the time of death. The absence of linked maternal and live birth data precluded direct assessment of maternal or perinatal risk factors. Finally, observed associations reflect patterns rather than causal relationships and must be interpreted with caution. Because this study uses ecological data aggregated at the state and city levels, the associations identified cannot be interpreted as causal or applicable to individual infants.
Conclusions
Between 2014 and 2023, infant mortality in Mexico remained largely stable, with minimal net change despite a substantial increase in reported medical attendance at the time of death. Infant deaths were predominantly due to neonatal and perinatal conditions that are largely preventable, and clear territorial gradients were observed by city size, affecting access to care, autopsy performance, and the recording of precise causes.
Our findings indicate that persistent infant mortality reflects structural and system-level factors rather than seasonal variation or short-term fluctuations. Strengthening the quality, continuity, and surveillance of maternal and infant health care will be essential to better understand and address preventable infant deaths in Mexico.
These findings suggest that improvements in nominal service coverage alone are unlikely to substantially reduce infant mortality without parallel investments in quality of perinatal care, continuity across levels of care, and stronger mortality investigation systems.
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
This study used publicly available anonymized secondary data from the national vital statistics system maintained by the National Institute of Statistics and Geography (INEGI). According to Mexican regulations for research using non-identifiable public datasets, the study qualifies for exemption from informed consent. The study protocol was reviewed and approved by the Institutional Review Board code CEI00120231011 (IRB No. 2022-016, amendment approved April 29, 2025).
Author Contributions
Conceptualization: N.M.D., G.C.; Methodology: N.M.D., G.C., H.A.; Data Curation: N.M.D., A.P.N., A.O.M.; Formal Analysis: N.M.D., A.P.N.; Investigation: A.O.M., N.M.D.; Software: A.P.N.; Validation: A.P.N., H.A.; Resources: A.O.M.; Visualization: N.M.D., A.P.N.; Writing – Original Draft: N.M.D.; Writing – Review & Editing: N.M.D., G.C., A.P.N., A.O.M., H.A.; Supervision: N.M.D.; Project Administration: N.M.D. All authors have read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: IMSS-BIENESTAR PP-Q008
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.