
Abstract
Background
Despite improved survival after pediatric hematopoietic stem cell transplantation (HSCT) in Thailand, many children experience physical and psychological distress. This pilot study evaluated the feasibility of a child life program and its preliminary effects on outcomes.
Methods
This pilot pre–post study included 10 children aged 2–8 years undergoing HSCT. The program comprised an HSCT educational video, therapeutic play, art therapy, online group activities, and homebound instruction after discharge. Outcomes were assessed at baseline and 6 months using the Pediatric Quality of Life Inventory (PedsQL), Child Behavior Checklist (CBCL), and Parenting Stress Index (PSI). Changes were analyzed using paired t-tests.
Results
PedsQL total, nausea, and nutrition scores improved significantly. PSI difficult child scores decreased slightly, whereas CBCL scores showed no significant changes. Six children returned to school within one year.
Conclusion
Child life services were feasible and showed potential to improve short-term quality of life in HSCT patients.
Introduction
Hematopoietic Stem Cell Transplantation (HSCT) is a standard treatment for many pediatric life-threatening hematologic/oncologic diseases, immune deficiencies, and metabolic disorders. Although the five-year survival rate for pediatric cancer patients in Thailand has improved from 39.4% (1990–2000) to 47.2% (2001–2011), 1 children undergoing HSCT continue to experience substantial long-term physical and psychological stress. These challenges, often related to complications such as infections and graft rejection requiring prolonged hospitalization, adversely affect quality of life and educational opportunities. Compared with children with other chronic illnesses, HSCT recipients are at higher risk for behavioral problems, emotional dysregulation, and impaired social skills. 2
During HSCT, pediatric patients are typically confined to isolation rooms with limited activities and prolonged hospitalization, and they often require long-term follow-up. They may experience fatigue, pain, sleep disturbances, and depression, which negatively affect psychological well-being. 3 Studies show that pediatric HSCT recipients have more behavioral difficulties and lower quality of life than their non-transplant peers.3,4 Moreover, mothers of HSCT patients experience significantly higher levels of psychological distress, 4 including high levels of anxiety and depression during hospitalization, as well as persistent distress years later. 5
HSCT is also associated with significant educational disruption. A report by the American Cancer Society revealed that children with cancer are significantly less likely to graduate from high school compared to their siblings 6 and are less likely to achieve age-appropriate educational milestones, with increased need for special education services, particularly in younger children. 7
These findings highlight the need for care that extends beyond medical treatment to include psychosocial support. “Child life services” provide a holistic approach by preparing children for medical procedures, reducing stress and anxiety, managing discomfort, and supporting educational development. Interventions include developmentally appropriate education, therapeutic play, expressive arts, and stress-reduction techniques. Evidence shows that such approaches reduce caregiver anxiety, improve psychological adjustment and recovery, and enhance long-term quality of life.8-10 They also reduce behavioral and emotional difficulties and support reintegration into mainstream education. 11 However, evidence on structured child life interventions in pediatric HSCT settings, particularly in low- and middle-income countries, remains limited. 12 In response, the Pediatric Recreation Program, the Hospital-Based Educational Service, and the Division of Developmental and Behavioral Pediatrics at the Faculty of Medicine Ramathibodi Hospital have implemented child life services for children undergoing HSCT.
Aim
This pilot study aimed to describe the implementation of child life service activities and to evaluate the feasibility and preliminary impact on quality of life, behavioral and emotional outcomes among pediatric HSCT patients, and parental stress.
Methods
Study Design
This pilot pre–post study was conducted to describe the implementation of child life service activities and to explore preliminary changes in outcomes among pediatric patients undergoing HSCT.
Participants
This was a single-center study conducted at the Faculty of Medicine Ramathibodi Hospital. Participants were children who underwent HSCT between September 2023 and December 2025. Eligible participants were children aged 2–8 years who had received HSCT and whose parents provided informed consent. Parents were required to be able to speak, read, and write Thai. Children who were unable to participate in the intervention activities due to severe medical instability were excluded.
The sample size was based on feasibility, consistent with a pilot study design. Twelve participants were initially enrolled. One child was excluded due to unstable medical conditions that prevented continuation of the intervention, and one child died during the study period. The final sample consisted of ten children who completed the six-month follow-up assessment.
Ethical Approval and Informed Consent
This study was approved by the Human Research Ethics Committee, Mahidol University (approval number: COA.MURA2023/667). Written informed consent was obtained from all parents prior to enrollment.
Measures
Demographic Characteristics
Demographic data were collected using a structured questionnaire. Child characteristics included age, sex, diagnosis, educational background, and current educational status. Caregiver information included the relationship to the child, educational background, occupation, and household income.
Pediatric Quality of Life Inventory (PedsQL)
Health-related quality of life was assessed using the Pediatric Quality of Life Inventory (PedsQL) Stem Cell Transplant Module. The Thai version has previously demonstrated good reliability and validity. 13 The questionnaire includes 31–39 items depending on the child’s age, with scores ranging from 0 to 100, where higher scores indicate better quality of life. For children aged 8 years or younger, the questionnaire was completed by parents, with assistance from a researcher when necessary.
Parenting Stress Index – Short Form (PSI-4-SF)
Caregiver stress was assessed using the Thai version of the Parenting Stress Index – Short Form (PSI-4-SF), which consists of 36 items measuring three domains: Parental Distress, Parent–Child Dysfunctional Interaction, and Difficult Child. Items are rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Raw scores are converted to standardized T-scores; scores below 62 indicate normal stress levels. 14
Child Behavior Checklist (CBCL)
Children’s behavioral and emotional problems were assessed using the parent-report version of the CBCL. Two age-specific forms were used: the CBCL for ages 1.5–5 years (100 items) and the CBCL for ages 6–18 years (120 items). Each item is rated on a 3-point scale (0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true). T-scores were calculated for total, internalizing, and externalizing problems. A T-score≥60 indicates borderline to clinical levels of behavioral problems. 15
Procedure
Baseline data were collected on the first day of hospital admission for HSCT. The PedsQL, PSI-4-SF, and CBCL were administered prior to the intervention and reassessed 6 months after the intervention. In addition, caregivers completed a satisfaction survey at the end of the intervention period.
The Child Life Services Intervention for Pediatric HSCT Patients

HSCT=Hematopoietic Stem Cell Transplantation.
Statistical Analysis
All statistical analyses were conducted using Stata/SE version 18.5 (StataCorp LLC, College Station, TX, USA). Descriptive statistics were used to summarize the baseline characteristics of pediatric patients and their caregivers. Categorical variables were reported as frequencies and percentages, while continuous variables were presented as means and standard deviations (SD).
Given the exploratory nature of this pilot study and the small sample size, the analyses focused on describing changes in outcomes before and after the intervention. Normality assumptions were assessed prior to applying parametric tests. Paired t-tests were used to examine within-participant differences between baseline and six-month follow-up for continuous outcomes, including patients’ quality of life, caregiver stress levels, and children’s behavioral and emotional problems. All statistical tests were two-sided, and p-values<0.05 were considered statistically significant. Results should be interpreted as preliminary and hypothesis-generating.
Results
Demographic Characteristics of Pediatric Patients and Caregivers
Descriptive Characteristics of Children and Parents (n=10)

HSCT=Hematopoietic Stem Cell Transplantation.
Changes in Patients’ Quality of Life, Parental Stress, and Behavioral Outcomes (Table 3)
Comparison of the PedsQL, PSI-4-SF, and CBCL Scores Between Pre-intervention and Post-intervention (n=10)
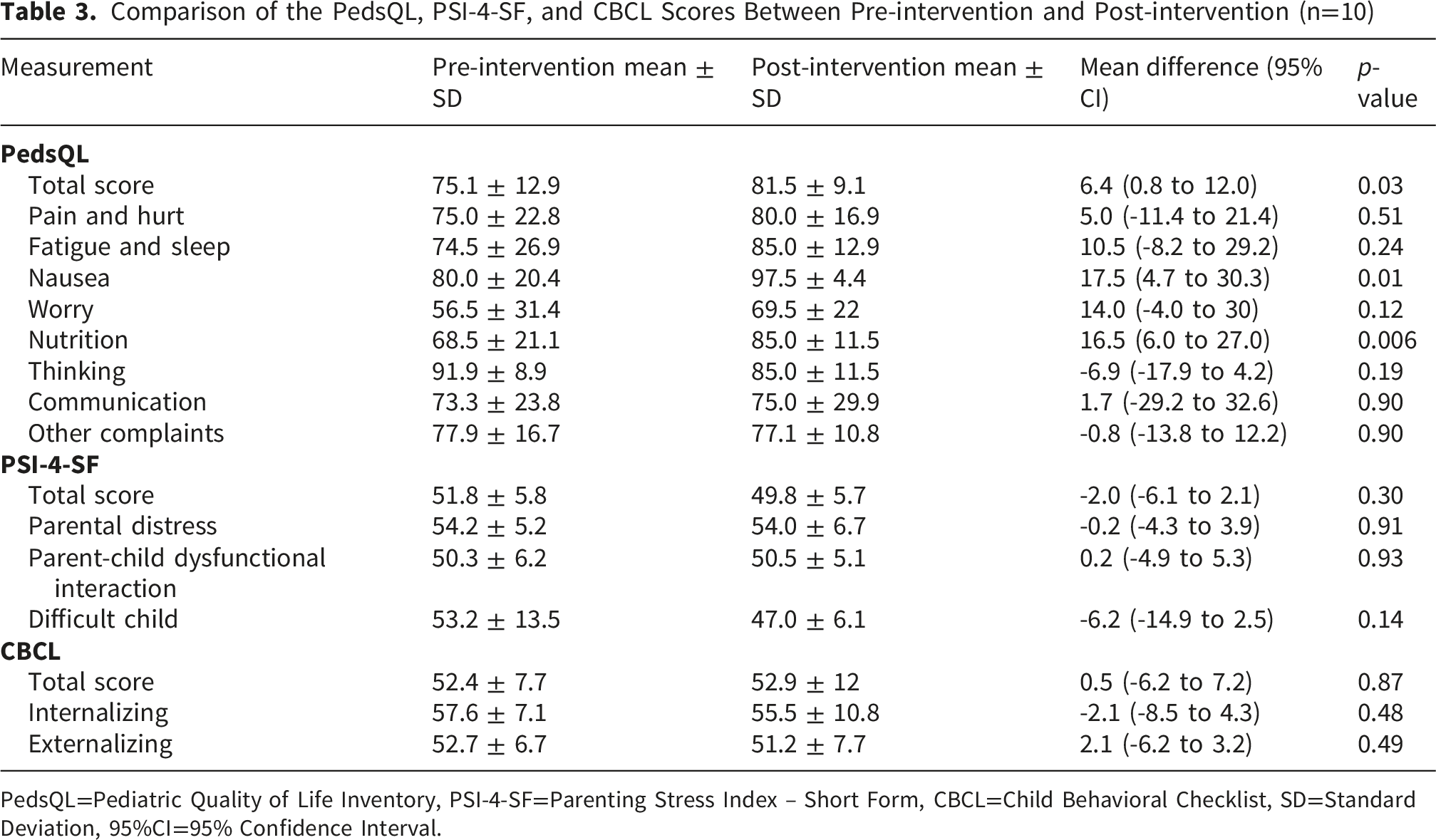
PedsQL=Pediatric Quality of Life Inventory, PSI-4-SF=Parenting Stress Index – Short Form, CBCL=Child Behavioral Checklist, SD=Standard Deviation, 95%CI=95% Confidence Interval.
No statistically significant differences in overall parental stress scores, measured by the PSI-4-SF between the pre- and post-intervention assessments. However, a non-significant reduction in mean scores was noted in the “difficult child” domain.
For behavioral and emotional outcomes, no statistically significant changes were observed in the CBCL total scores or in the internalizing and externalizing domains. Baseline CBCL scores were generally within the non-clinical range. One participant demonstrated worsening CBCL scores across domains at follow-up. This case was associated with significant family stress during the study period, as the child’s mother experienced a stroke during the first month of hospitalization.
At one-year follow-up, six of the ten participating children had returned to mainstream schooling without special educational support. Two children were not yet of school age. The remaining two had not returned to school due to disease relapse or the need for ongoing immunosuppressive treatment.
Caregiver Satisfaction With the Intervention
Most caregivers reported high levels of satisfaction with the intervention components, including the educational video, child life activities, and the individualized educational program. Only one caregiver reported low satisfaction with the individual educational program and overall intervention experience; this caregiver was from the same family in which the child’s CBCL scores increased at follow-up. Caregivers also provided positive feedback regarding the program, noting that the activities helped keep children engaged during hospitalization and reduced boredom. Some caregivers reported perceived improvements in their children’s emotional well-being and coping during treatment.
Discussion
This pilot study describes the implementation of a child life service program for pediatric patients undergoing HSCT in Thailand and explores preliminary changes in patient and caregiver outcomes following the intervention. This study adds to the limited evidence on structured child life interventions in pediatric HSCT, particularly in a low- and middle-income country (LMIC) setting, where such services are not routinely available. To our knowledge, this is among the first studies in Thailand to report the structured integration of child life services specifically for pediatric HSCT patients. The program provided sustained psychosocial and educational support throughout the transplantation and follow-up periods. After six months, improvements were observed in the PedsQL total score and in the nausea and nutrition subscales, suggesting potential benefits for certain aspects of health-related quality of life during recovery. Physical symptoms such as nausea and nutritional difficulties are common following intensive chemotherapy and transplantation and may substantially affect children’s daily functioning and well-being. Previous research has highlighted the important role of physical symptoms in shaping health-related quality of life among pediatric HSCT survivors. 3 Interventions addressing both psychosocial coping and physical discomfort may therefore support overall adjustment.
Several potential mechanisms may explain the observed improvements in quality of life. Therapeutic play and developmentally appropriate activities may help children cope with hospitalization by providing a distraction from illness-related stress and introducing a sense of normalcy during treatment. 16 Previous studies indicate that children undergoing HSCT frequently experience fear and uncertainty during treatment 17 and play-based interventions may reduce distress by facilitating emotional expression, distraction, and engagement in age-appropriate activities during hospitalization. 18
Despite these potential benefits, no statistically significant reduction in overall parental stress was observed. A modest decrease was observed in the “difficult child” dimension of the PSI-4-SF. This finding may reflect indirect benefits of the intervention on children’s coping and behavior, which may influence caregiver perceptions. The intervention primarily targeted the child rather than caregiver stress, which may explain the limited impact. This finding is consistent with a prior study showing that child-focused interventions may not significantly reduce parental stress but can improve aspects of parental well-being. 19 Additionally, parental adjustment during HSCT is influenced by factors such as coping strategies, optimism, and family support, which were not directly addressed. Baseline parental stress levels were also within the normal range, potentially limiting the detectability of change. However, there is a need for individualized parental supportive care that extends beyond acute hospitalization into long-term follow-up after pediatric HSCT. 5
No significant changes were observed in children’s behavioral and emotional problems as measured by the CBCL. This may be due to baseline scores being within the normative range, leaving limited room for improvement. Similar findings have been reported in pediatric HSCT populations, where behavioral functioning remains relatively stable over time. 20
The study population included children undergoing HSCT for a variety of underlying diseases rather than oncology diagnoses alone, the psychosocial impact of HSCT appeared to vary according to diagnosis, with children diagnosed with leukemia being slightly more adversely affected. These findings suggest that interventions aimed at improving quality of life and addressing behavioral issues should be tailored to the specific underlying condition. 21
Caregiver feedback suggested several perceived benefits of the program beyond the quantitative outcomes. Given the prolonged school absence associated with HSCT, hospital-based education and homebound instruction supported continued learning during treatment. Online group activities also allowed children to interact with peers, which may support social development and facilitate reintegration into school and community settings.
Study Limitations
Several limitations should be considered when interpreting the findings of this study. First, the absence of a control group limits the ability to attribute observed changes directly to the intervention, as improvements may also reflect the natural course of recovery following HSCT. Second, the small sample size and single-center design limit the generalizability of the findings. Third, the follow-up period was limited to six months for most outcomes, which may not fully capture longer-term psychosocial adjustment following transplantation. Last, potential reporting bias due to parent-reported outcomes cannot be excluded. Future research should include larger samples and controlled study designs to further evaluate the effectiveness of child life interventions for pediatric HSCT patients. Longer follow-up periods may also help clarify the potential impact of these interventions on children’s long-term psychosocial adjustment and school reintegration.
Implications for Practice
Despite these limitations, the findings of this pilot study suggest that implementing child life services in pediatric HSCT care is feasible and may offer supportive benefits to children undergoing intensive treatment, with potential for scalability in similar resource-limited settings. Developmentally appropriate interventions, including therapeutic play, art-based activities, and hospital-based educational support, may help address psychosocial challenges during hospitalization and recovery. Future interventions may benefit from incorporating individualized needs assessments and family feedback to better tailor psychosocial support to each child’s and family’s unique experiences and priorities. In addition, family involvement and structured educational activities may help support continuity of learning and facilitate children’s transition back to school following transplantation.
Conclusion
This pilot study describes the implementation of a child life service program for pediatric HSCT patients and provides preliminary evidence of potential improvements in selected quality-of-life domains. Although no significant changes were observed in behavioral outcomes or parental stress, the findings suggest that structured psychosocial and educational support shows potential to contribute to children’s overall adjustment during and after HSCT. Larger controlled studies are needed to further evaluate the role of child life interventions in supporting recovery and long-term well-being in this population.
Footnotes
Acknowledgments
We would like to thank the Pediatric Recreation Service and the Hospital-Based Educational Service for hospitalized children at Ramathibodi Hospital.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Faculty of Medicine Ramathibodi Hospital, Bangkok, Thailand (RF_67010).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical Trial Registration
This study was registered in the Thai Clinical Trials Registry (TCTR20240804001). The study protocol was finalized before participant recruitment and no major protocol modifications were made during the study period.