
Abstract
Background
Respiratory therapy education includes both associate (AAS/AS) and baccalaureate (BS) degree programs. This dichotomy has created discussions about the potential benefits of academic progression for entry-level practice. Little empirical evidence exists comparing the critical-thinking abilities of participants from these different educational pathways. This study was undertaken to investigate whether differences in critical-thinking skills exist between participants nearing graduation from AS and BS respiratory therapy programs.
Methods
This cross-sectional study recruited respiratory therapy participants (1 month pre- to 3 months post-graduation) from associate and baccalaureate programs nationwide. Critical thinking was assessed using the Health Sciences Reasoning Test-Numeracy (HSRT-N). Independent samples t-tests compared HSRT-N scores between degree types, gender, and ethnicity, with statistical significance set at P ≤ .05.
Results
A total of 184 participants (81 associate and 103 baccalaureate) completed the HSRT-N. No significant differences were found in any critical-thinking measure between associate and baccalaureate participants. Gender analysis showed borderline significance for numeracy (P = .05) with male participants scoring higher, though the sample had substantially more women (n = 150) than men (n = 34). Significant differences were observed between white and non-white participants in all measures except evaluation (P < .01), with white participants scoring higher.
Conclusion
Alignment between AS and BS programs in the teaching of critical-thinking skills is essential to ensure those skills are systematically developed and extended through academic progression. Both program types share responsibility for addressing the gaps identified in this study, particularly in the lower-performing domains of interpretation, evaluation, deduction, and numeracy. Future research should incorporate clinical performance measures and examine long-term development of critical-thinking skills throughout respiratory therapists’ careers.
Keywords
Critical thinking is a core competency for respiratory therapists, enabling accurate analysis of clinical data and timely decision-making that impacts patient outcomes. Both associate and baccalaureate respiratory therapy programs emphasize developing these skills. Existing evidence suggests that critical-thinking ability may be influenced more by instructional strategy and cumulative coursework across a student’s educational background, including general education and foundational sciences, than by the specific length of a respiratory therapy program or degree awarded. Prior studies in other health professions, such as nursing, have demonstrated links between higher educational attainment and improved patient outcomes, though similar findings in respiratory therapy remain limited. This study found no statistically significant differences in critical-thinking abilities, as measured by the Health Sciences Reasoning Test-Numeracy, between associate and baccalaureate respiratory therapy participants near graduation. White participants scored significantly higher than non-white participants in all domains except evaluation, and male participants scored higher in numeracy, though gender differences did not reach statistical significance for the overall score. Compared to other health professions, respiratory therapy participants’ scores ranked below average percentile levels.Quick look
Current knowledge
What this paper contributes to our knowledge
Introduction
Critical thinking is a cornerstone of effective healthcare delivery and is particularly vital in respiratory therapy, where clinicians must make complex, time-sensitive decisions that directly impact patient outcomes. As the respiratory care profession continues to evolve with technological advancements and expanding scope of practice, the cognitive abilities of its practitioners—specifically critical thinking and clinical judgment—have become increasingly significant determinants of quality care. 1 The importance of critical thinking and effective clinical decision-making has been well-researched in medical literature, and generally accepted to be dependent upon both educational preparation and experience.2–6 Critical thinking is a prerequisite for efficient and effective clinical judgment, and its presence in the clinical arena has been shown to result in faster and more accurate diagnoses and improved health outcomes for patients. 7 These cognitive skills are generally accepted to be dependent upon both educational preparation and clinical experience, making them crucial areas for investigation as the respiratory therapy profession examines possible revision of its educational standards and pathways.
In 2007, the American Association for Respiratory Care (AARC) created a task force charged with providing recommendations for the future direction of the profession beyond 2015. 8 Published in 2009, one of the nine recommendations included academic progression that would require a baccalaureate degree as the entry level to the profession. The AARC Board of Directors amended that goal, proposing that 80% of respiratory therapists (RTs) would either earn a bachelor’s degree or pursue an advanced degree by 2020. 9 The Task Force adjusted its position and set a new goal that by 2030 all new respiratory therapists should obtain a minimum of a bachelor’s degree for entry into the profession. 10 In January 2018, the Commission on Accreditation for Respiratory Care (CoARC) mandated that any new RT program must award baccalaureate or master’s degrees. 11 This mandate has since been removed partially due to the lack of significant growth in baccalaureate level respiratory care programs, increased need for therapists, and public demand to address critical shortages.
While considerable attention has been given to the structural and policy aspects of academic progression in respiratory therapy, there has been relatively little empirical investigation into whether different educational pathways result in measurable differences in critical-thinking abilities, the very cognitive skills that underpin clinical excellence. This represents a significant gap in our understanding of how educational preparation influences the development of these essential skills in respiratory therapy practitioners. Other healthcare professions have addressed this issue through evidence-based approaches. In nursing, for example, research has demonstrated relationships between educational preparation and various outcomes, including critical-thinking abilities and patient care metrics. A systematic review of 29 studies published in 2015 found that higher levels of nursing education were related to significantly fewer patient falls. 12 Aiken et al 13 analyzed discharge data for 422,730 patients aged 50 or older who underwent common surgeries in 300 hospitals in nine countries, estimating mortality risk. 13 After considering severity of illness and hospital characteristics, the authors found that nursing education was significantly associated with mortality (P = 0.002), reporting that for every 10% increase in the number of Bachelor of Science in Nursing (BSN)-prepared nurses, mortality decreased by 7%. Beyond better patient outcomes, improved education levels of clinicians may be cost effective. Yakusheva et al 14 conducted an economic analysis of meeting the recommended 80% BSN threshold on both patient outcomes and cost, using data from 8526 medical-surgical patients. 14 They found that patients who received care at institutions where ≥80% of RNs were bachelor’s prepared had shorted length-of-stay (P = .03) and lower readmission rates (P = .04).
In 2010, the National Academy of Medicine (formerly the Institute of Medicine) published a report recommending that the percentage of RNs with a BSN increase to 80% by 2020. 15 Although the American Association of Community Colleges published an opposition paper in response, the American Association of Colleges of Nursing (AACN) drafted a position statement in 2017 stating that, while they do not intend to prevent graduates of associate degree programs from entering the profession, they strongly believe that “registered nurses should be minimally prepared with the bachelor of science degree in nursing.” 16 The position paper also reported that more than 70% of Chief Nursing Officers perceived differences in practice between BSN-prepared nurses and those with an associate degree or hospital diploma, explicitly citing stronger critical-thinking skills and leadership abilities among baccalaureate-prepared nurses; however, it should be noted this evidence reflects perceived rather than empirically measured differences. The Accreditation Council for Occupational Therapy Education is also currently considering increasing entry-level degree requirements for occupational therapy assistants from an associate to a baccalaureate degree. A study by Smith and colleagues reported that respiratory therapists in NY State were in favor of both requiring the baccalaureate degree as entry level to the profession (64%) and remaining in the profession (78%). 17 Most respondents (70%) further acknowledged that, in the current climate, respiratory care is at risk of losing clinicians due to limited ability for growth and/or lack of confidence in the future of the profession. 17 The study concludes that only by increasing educational preparation and scope of practice can RT be competitive with other healthcare professions in the current healthcare environment. 17
A search of the medical literature reveals a lack of research comparing RT graduates from 2- and 4-year institutions regarding critical-thinking and decision-making skills, representing a gap in knowledge. The aim of this study was to evaluate whether differences exist in critical-thinking skills between recent graduates of 2-year and 4-year respiratory therapy programs (defined as 1 month prior to through 3 months post-graduation). This research seeks to inform the ongoing discourse on academic progression in respiratory therapy by exploring how educational pathways may impact cognitive development relevant to high-quality patient care.
Do critical-thinking abilities differ between individuals nearing graduation or recently graduated from associate (2-year) versus baccalaureate (4-year) respiratory therapy programs?
Methods
Our research began as a mixed-methods cohort study comparing critical-thinking and clinical decision-making abilities between participants near graduation from associate degree and baccalaureate respiratory therapy (RT) programs. A convenience sample of 184 participants was recruited from 18 associate and baccalaureate respiratory therapy programs across the United States, with the intent of achieving balanced representation from both educational cohorts. Participants were incentivized to participate with $20 gift cards.
Critical-thinking skills were measured by the Health Sciences Reasoning Test-Numeracy (HSRT-N), a 38-item multiple choice assessment that is an enhanced version of the Health Sciences Reasoning Test (HSRT). Numeracy is a vital component of clinical reasoning and includes understanding how quantitative information is gathered, represented, and correctly interpreted using graphs, charts, tables, and diagrams. The HSRT-N is taken on a secure, encrypted online testing system. The test also measures interpretation, analysis, evaluation, inference, induction, deduction, explanation, and overall reasoning skills. 18 It is not discipline-specific—scores are reflective of the correct application of critical-thinking skills, not knowledge of memorized information. The HSRT-N total score discriminates between novice and expert critical-thinking skills, consequently establishing construct validity. 19 Clinical judgment was to be assessed through evaluation of student performance in two high-fidelity simulations using a third-party simulation vendor for outcome assessment. Simulations included components from the following AARC Evidence-Based Clinical Practice Guidelines: Effectiveness of both Pharmacologic and Nonpharmacologic Airway Clearance Therapies in Hospitalized Patients; Care of the Ventilator Circuit and Its Relation to Ventilator-Associated Pneumonia; and Weaning and Discontinuing Ventilatory Support. Each student’s performance was to be evaluated by one of the researchers and one high-fidelity simulation vendor.
Due to the impact of COVID-19 in 2019–2020, established methodology plans to assess clinical judgment through evaluation of student performance in two high-fidelity simulations using a third-party simulation vendor for outcome had to be suspended from the study. As the pandemic continued to affect travel and university/college closures continued to be barriers to clinical simulation assessment, the HSRT-N became the focus of the study. Therefore, the qualitative component of the mixed-methods study was dropped and the team continued with the quantitative portion. This shift in methodology was not without concern. By relying solely on the HSRT-N, the study lost the opportunity to observe how participants perform in realistic clinical scenarios, the kind of hands-on, time-pressured decision-making that defines respiratory therapy practice. Standardized critical-thinking assessments, while valuable, capture reasoning ability in the abstract rather than in action. Readers should therefore interpret the findings with the understanding that differences, or similarities, in HSRT-N scores between degree types may not fully reflect how participants would perform at the bedside. Conclusions about the relationship between educational pathways and clinical reasoning should be drawn with appropriate caution. Nevertheless, comparison of critical-thinking and decision-making skills between associate degree and baccalaureate degree RT programs remains an important foundational research question that has not been definitively answered in the literature for the RT profession. The revised quantitative approach remains well-suited to address the study’s central research question: whether measurable differences in critical-thinking ability exist between associate and baccalaureate respiratory therapy participants near graduation. The HSRT-N is a validated, widely used instrument in health sciences education research with established construct validity for discriminating critical-thinking ability. Its standardized format allowed for consistent, objective comparison across multiple programs during a period when in-person assessment was not feasible. While the findings should be interpreted within these constraints, the quantitative data provide a meaningful and necessary foundation for understanding critical-thinking development across RT educational pathways.
Independent samples t-test was selected as the most appropriate statistical method for comparing mean scores between two independent groups (associate vs baccalaureate). The parametric test was suitable given our continuous outcome variables (HSRT-N scores) and independent group structure. Prior to all comparisons, Levene’s test for equality of variances was used to confirm homogeneity of variance between groups. We compared HSRT-N scores between AAS/AS and BS degree programs, participants, gender, and ethnicity, with P ≤ .05 considered to be statistically significant. All statistical analyses were performed using IBM SPSS Statistics, Version 27 (IBM Corp., Armonk, NY). Prior to all comparisons, Levene’s test for equality of variances was used to confirm homogeneity of variance between groups, and equal variances were assumed for all analyses. No additional assumption checks or supplementary analyses were conducted beyond variance testing. This study was approved by the Texas State University Institutional Review Board (approval #5792).
Results
HSRT-N difference based on program type. a
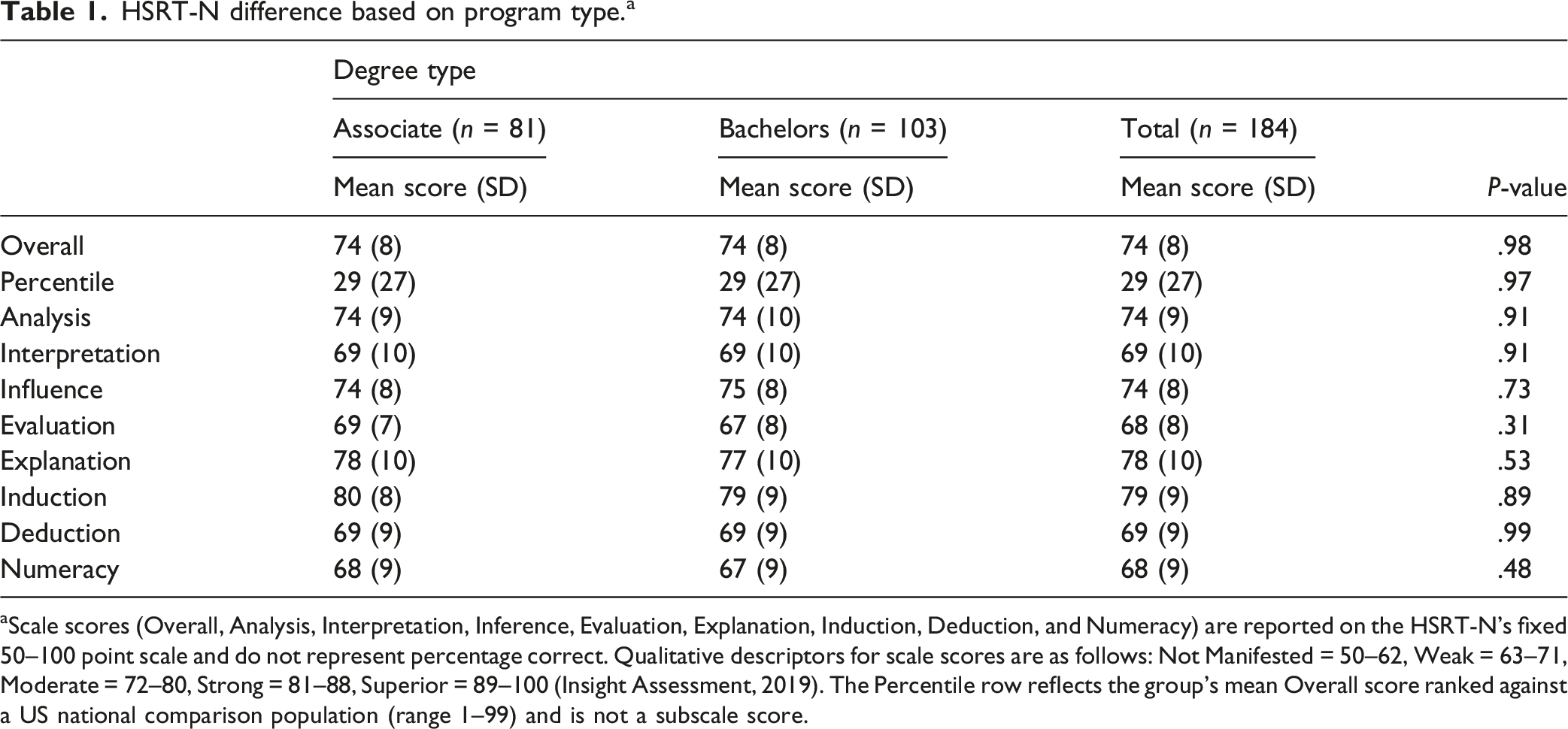
aScale scores (Overall, Analysis, Interpretation, Inference, Evaluation, Explanation, Induction, Deduction, and Numeracy) are reported on the HSRT-N’s fixed 50–100 point scale and do not represent percentage correct. Qualitative descriptors for scale scores are as follows: Not Manifested = 50–62, Weak = 63–71, Moderate = 72–80, Strong = 81–88, Superior = 89–100 (Insight Assessment, 2019). The Percentile row reflects the group’s mean Overall score ranked against a US national comparison population (range 1–99) and is not a subscale score.
HSRT-N difference based on gender selection. a
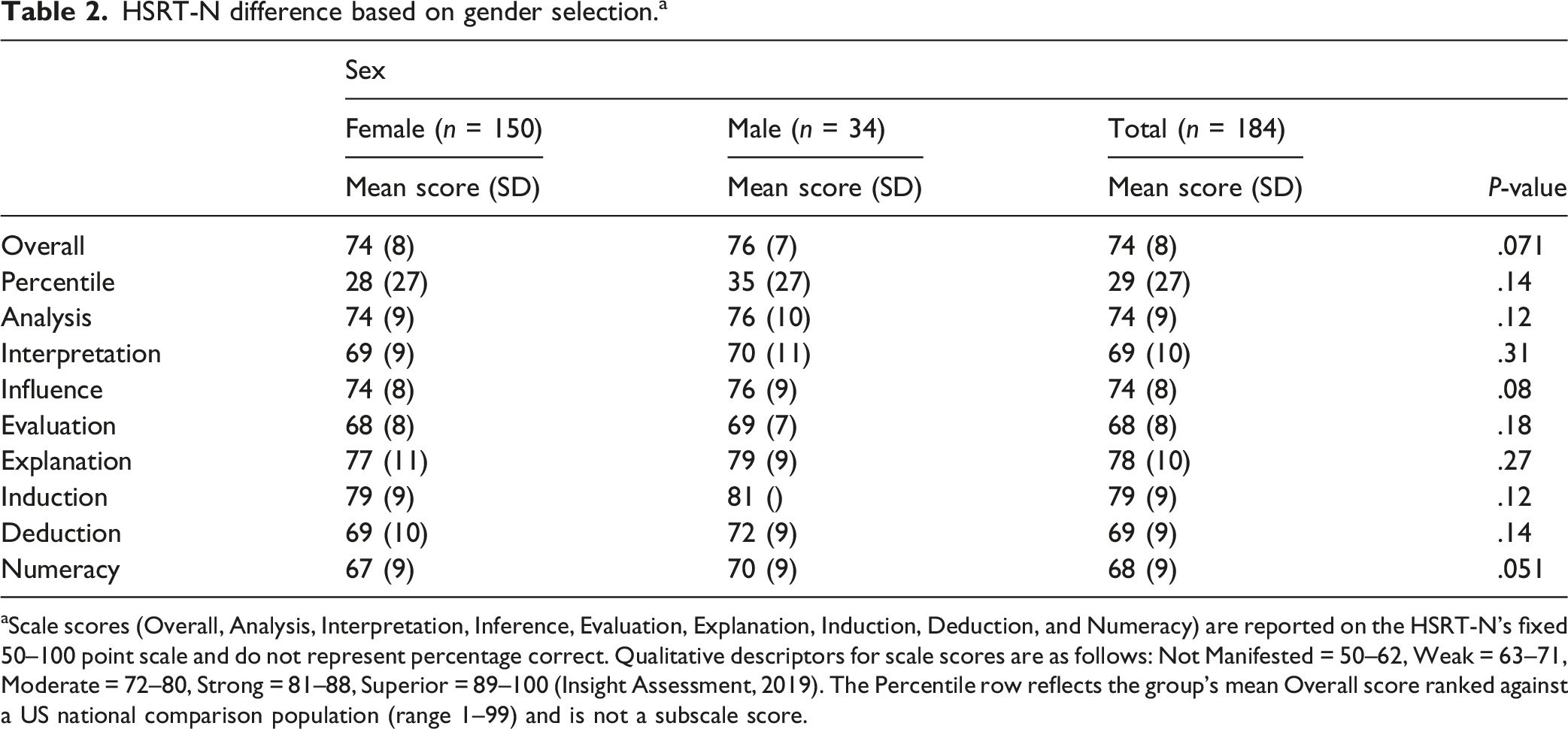
aScale scores (Overall, Analysis, Interpretation, Inference, Evaluation, Explanation, Induction, Deduction, and Numeracy) are reported on the HSRT-N’s fixed 50–100 point scale and do not represent percentage correct. Qualitative descriptors for scale scores are as follows: Not Manifested = 50–62, Weak = 63–71, Moderate = 72–80, Strong = 81–88, Superior = 89–100 (Insight Assessment, 2019). The Percentile row reflects the group’s mean Overall score ranked against a US national comparison population (range 1–99) and is not a subscale score.
HSRT-N difference based on white versus non-white selection. a
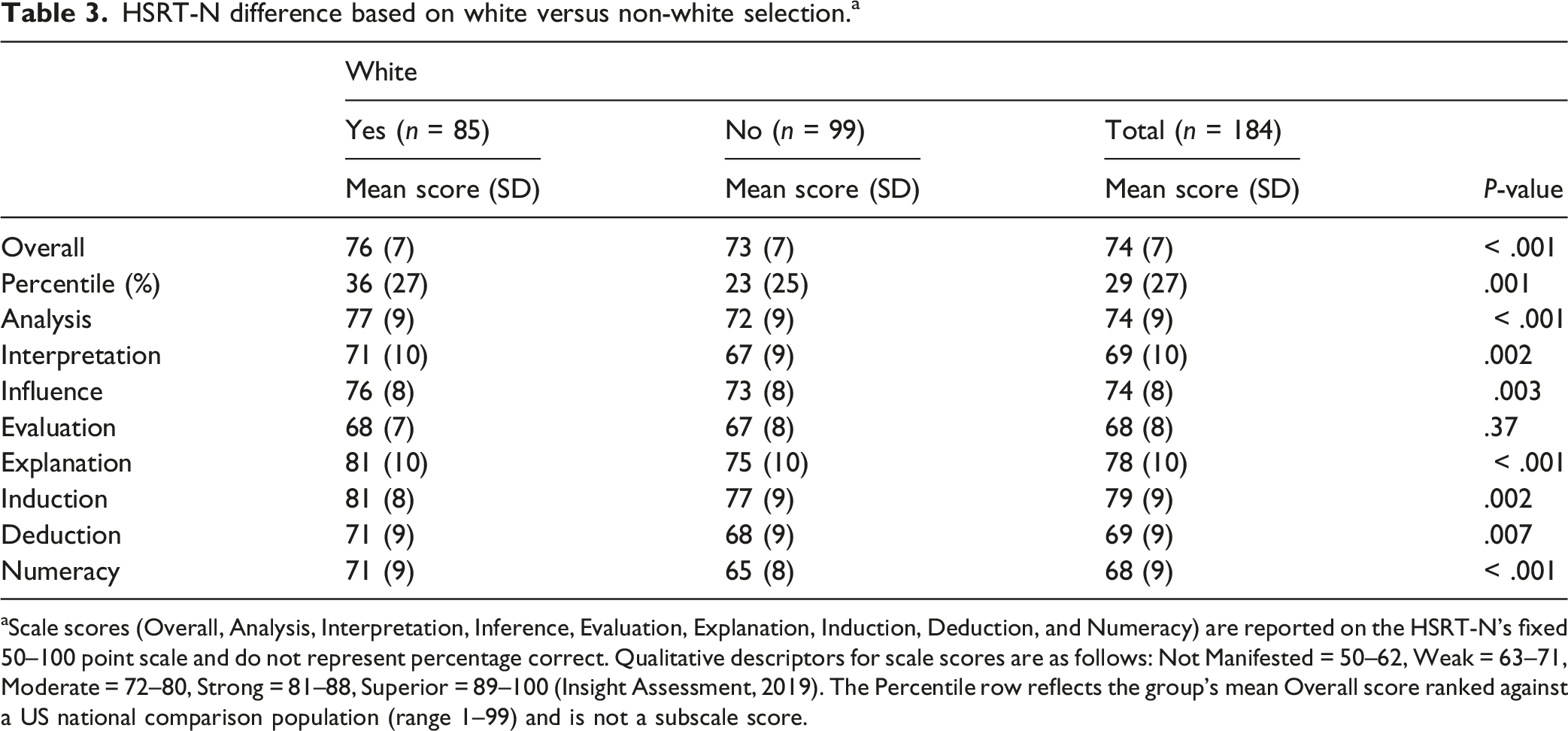
aScale scores (Overall, Analysis, Interpretation, Inference, Evaluation, Explanation, Induction, Deduction, and Numeracy) are reported on the HSRT-N’s fixed 50–100 point scale and do not represent percentage correct. Qualitative descriptors for scale scores are as follows: Not Manifested = 50–62, Weak = 63–71, Moderate = 72–80, Strong = 81–88, Superior = 89–100 (Insight Assessment, 2019). The Percentile row reflects the group’s mean Overall score ranked against a US national comparison population (range 1–99) and is not a subscale score.
Each HSRT-N assessment is composed of the following parameters:
The
Discussion
The results of this study provide important insights into critical-thinking abilities among respiratory therapy participants pre- and post-graduation. Our analysis using the HSRT-N revealed several key findings that have implications for respiratory therapy education and the ongoing debate about academic progression in the profession.
The results of this study provide valuable insights into the critical-thinking abilities of respiratory therapy (RT) participants near graduation. Despite the lack of statistically significant differences in HSRT-N scores between associate degree (AAS/AS) and baccalaureate (BS) RT participants, these findings should not be interpreted as an argument against academic progression in the field. Instead, they highlight the complexity of critical-thinking development and underscore the need for continued emphasis on enhancing these skills at all educational levels. Our study found no significant differences in critical-thinking abilities between RT participants from associate and baccalaureate degrees. This finding is notable as it diverges from some of the literature in nursing education, where differences in clinical outcomes have been observed with higher levels of education.13,14 However, similar findings have been reported in previous studies of RT education, suggesting that critical-thinking development is multifactorial, which suggests that the impact of degree type, while important, may not be the only contributor.20,21
There is limited investigation into the factors that may influence critical-thinking development in RT participants. Research using the HSRT has shown that while associate degree participants demonstrate the development of critical-thinking abilities, factors such as final GPA, student graduation status, and admission GPA have the strongest link to those scores. 20 This aligns with prior research indicating that prior coursework contributes to critical-thinking ability rather than degree type alone. Participants in health-related disciplines who had a stronger background in foundational sciences—such as biology, kinesiology, or exercise physiology—tended to perform better on critical-thinking assessments, independent of their degree level. 22 Coursework in subjects like biology, chemistry, and physics significantly contributed to critical-thinking skills and clinical decision-making. 22 Additionally, the study by Wettstein et al. 23 found that baccalaureate RT participants demonstrated a positive relationship between critical-thinking ability and science-course background on the Watson-Glaser Critical Thinking Appraisal, reinforcing our findings that degree type alone may not predict differences in critical-thinking abilities.
Another factor potentially contributing to the findings in our study is that the core clinical competencies required for entry-level respiratory therapy practice may be effectively taught in both 2-year and 4-year programs, with CoARC accreditation standards ensuring consistency across program types. The HSRT-N assesses generalized critical-thinking ability rather than discipline-specific knowledge or skills; therefore, the differences between degree types may not be easily determined. Despite the statistical similarities in HSRT-N scores, there are several reasons why the Bachelor of Science in Respiratory Care (BSRC) degree remains an important advancement for the profession. First, the complexity of respiratory therapy practice is increasing, requiring a workforce with higher levels of cognitive reasoning and decision-making skills.21,24 Second, a higher level of education has been linked to improved patient outcomes in other healthcare fields that are similar to respiratory therapy, even when differences in standardized test scores are not immediately apparent.13,14 Third, there is emerging evidence that academic progression enhances professional identity, leadership opportunities, and career mobility for respiratory therapists. 17
While degree type did not yield significant differences, our analysis revealed significant differences based on ethnicity. White participants scored higher than non-white participants in all measures except Evaluation. This finding aligns with other healthcare education research showing disparities in standardized testing outcomes across ethnic groups. 25 These differences may reflect broader educational inequities, language and cultural factors affecting test performance, or potential cultural bias in standardized assessment tools. 26 Given the increasing diversity in the healthcare workforce, respiratory therapy programs may need to implement targeted interventions, such as mentoring programs, curriculum adjustments, and inclusive pedagogical approaches, to support critical-thinking development across diverse student populations.
The gender analysis approached significance for overall score (P = .07) and for Numeracy (P = .05), with male participants scoring higher. However, caution is warranted in interpreting these results given the unbalanced sample sizes between male (n = 34) and female (n = 150) participants. Najafi et al 27 performed a longitudinal study of medical participants in Tehran and found a higher critical-thinking score for men versus women. However, the authors did not use the HSRT-N and the difference was for only two of the seven items assessed. Gender differences in critical thinking are not universally observed, and other studies suggest female participants may excel in aspects such as interpretation and inference, particularly in patient-care scenarios. 28 Gender disparities in standardized assessments may be influenced by test design, educational expectations, self-perceptions, learning styles, and confidence levels in test-taking rather than actual cognitive differences.
Percentile comparison of respiratory therapy participants to other health professions.
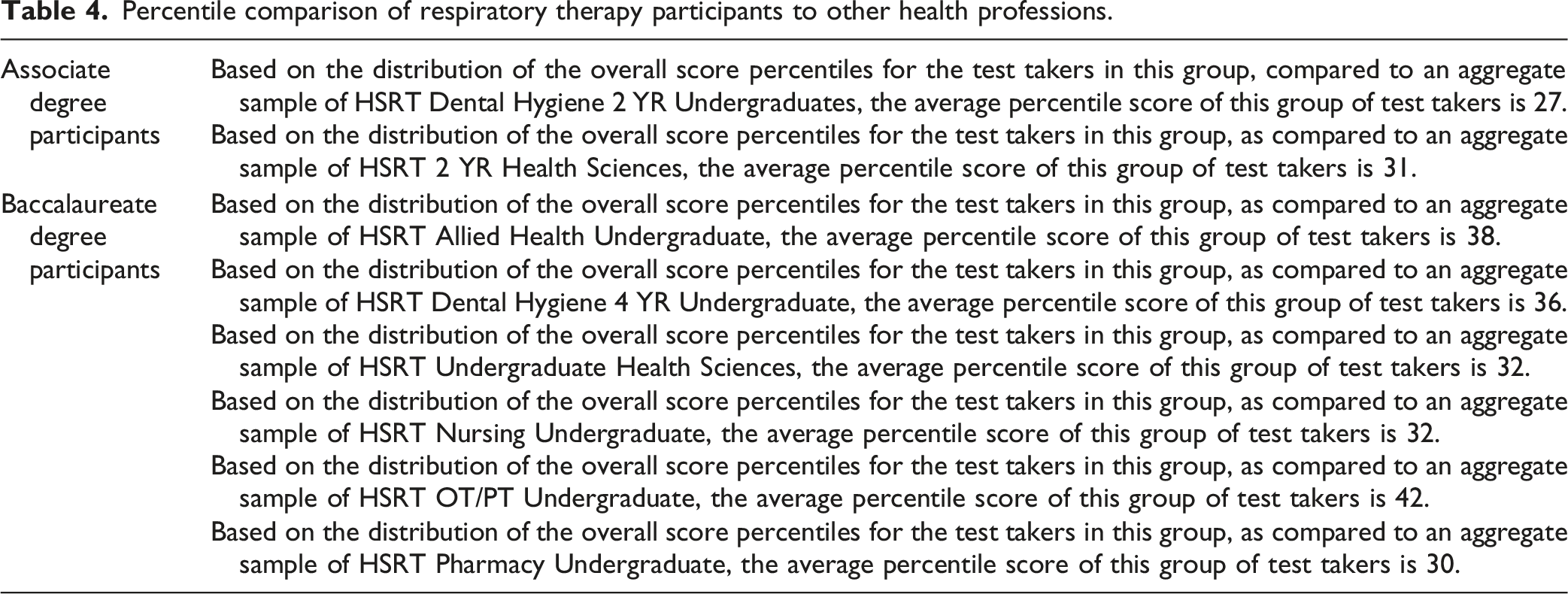
Our participants’ percentile rankings compared to other health profession participants provide additional context for interpreting the results. Associate degree RT participants scored at the 27th percentile compared to dental hygiene 2-year undergraduates and at the 31st percentile compared to other 2-year health sciences participants. Baccalaureate RT participants scored at the 38th percentile compared to allied health undergraduates, the 36th percentile compared to dental hygiene 4-year participants, and the 32nd percentile compared to nursing undergraduates.
These comparisons suggest that respiratory therapy participants’ critical-thinking abilities generally fall below the average of their peers in other health professions. This finding is concerning when considering the increasing complexity of respiratory therapy practice and the growing importance of independent clinical judgment in the field. Respiratory therapy educators may need to place greater emphasis on developing critical-thinking skills throughout the curriculum, regardless of program type. As Gutierrez et al. 29 emphasize, engaging students in evidence-based, protocol-guided clinical practice is not a cookbook approach but rather one that heightens the need for higher-order thinking skills, underscoring the importance of educational strategies that foster critical thinking through real-world, inquiry-centered learning experiences.
While our findings show comparable critical-thinking abilities between associate and baccalaureate degree participants, this should be viewed as evidence of the strong foundational education provided across all respiratory therapy programs rather than a challenge to academic progression. The push for degree advancement represents a forward-thinking vision for the RT profession that extends beyond critical-thinking development alone. CoARC entry-to-practice standards explicitly require graduates to demonstrate competency in interprofessional collaboration, effective communication with diverse patient populations, ethical decision-making, and professional responsibility (Standards 4.05–4.08). 30 While both AS and BS programs must meet these foundational accreditation requirements, baccalaureate and graduate education provide expanded opportunities to develop and refine these competencies through more advanced coursework, greater exposure to research and evidence-based practice, and broader clinical and professional experiences. The ability to function effectively within interprofessional teams, navigate complex ethical decisions, and communicate across diverse healthcare settings represents a growing expectation for respiratory therapy practitioners. Advanced academic preparation is well-positioned to reinforce and deepen these competencies. As the scope of respiratory care practice expands, these traits will only become more important for its practitioners. As the respiratory therapy profession continues to debate the merits of different educational pathways, there is a pressing need for empirical evidence regarding the relationship between degree type and critical-thinking outcomes.
Baccalaureate and graduate education provide numerous advantages essential for the evolution of respiratory therapy practice. Higher education cultivates broader knowledge of healthcare systems, research literacy, leadership preparation, and interprofessional collaboration skills. Furthering one’s education is increasingly crucial as the healthcare landscape becomes more complex and integrated. Four-year and graduate programs typically offer expanded coursework in research methods, healthcare management, advanced pathophysiology, and evidence-based practice that prepare respiratory therapists to function as autonomous healthcare professionals.
The nursing profession offers a compelling parallel, where research has demonstrated that increasing the proportion of BSN-prepared nurses improved patient outcomes, including decreased mortality rates and reduced length of stay.13,14 Similar benefits may emerge in respiratory therapy as more practitioners attain advanced degrees and apply this expanded knowledge base to patient care.
Academic progression is also vital for professional recognition and advancement. As Smith et al 17 emphasized, respiratory therapy must elevate both educational preparation and scope of practice to remain competitive with other healthcare professions. Advanced degrees position respiratory therapists to assume leadership roles, participate in research initiatives, develop specialized clinical expertise, and advocate effectively for the profession. Furthermore, degree advancement aligns with department directors’ preferences when hiring new graduate respiratory therapists to better meet the expanding roles and responsibilities of the profession. 31 The transition to baccalaureate and graduate education represents an investment in the profession’s future rather than a criticism of current educational models. Both degree pathways can develop competent clinicians with strong critical-thinking abilities, but advanced education provides additional dimensions of professional development that will be essential as respiratory therapy continues to evolve. Our study supports a thoughtful transition that builds upon the strengths of existing programs while expanding educational opportunities that will ultimately benefit patients and advance the profession.
Our findings have several implications for respiratory therapy education. First, the lack of difference between program types suggests that effective critical thinking instruction can occur in both 2-year and 4-year programs. Educators should focus on identifying and implementing best practices for developing critical-thinking skills regardless of program length or degree awarded.
Based on a qualitative study by Mishoe, 32 the best practices that educators should develop include incorporating teaching strategies that foster critical discourse, reflection, problem-solving, and decision-making skills among respiratory therapy students and practitioners. Specifically, educators should utilize problem-based learning, small-group discussions, and case-based approaches to help students develop a multidimensional understanding of critical thinking. 32 This requires moving beyond development of cognitive skills alone. Educational approaches should include the seven essential skills identified by Mishoe (prioritizing, anticipating, troubleshooting, communicating, negotiating, decision-making, and reflecting) as well as traits like openness to multiple perspectives and reflective capacity.
Educators should emphasize experiential learning in realistic clinical settings, encouraging students to continually examine their assumptions and recognize multiple perspectives. They should also help students learn to conduct informal action experiments, evaluate results, and adapt their approaches based on reflection-in-action, mirroring expert practice.
Fostering an environment of continual reflection on decisions and promoting effective communication and negotiation skills are critical. These practices will prepare students not just with knowledge but with the judgment, practical wisdom, and traits necessary for effective independent decision-making in complex, real-world situations. Overall, integrating these approaches into respiratory care education can build critical-thinking skills essential for safe, effective patient care.
However, the quantitative study by Goodfellow 33 adds an important caveat: some critical-thinking behaviors (e.g., particularly prioritizing, troubleshooting, and communicating) may be difficult to teach in formal professional training programs because they involve tacit knowledge and practical skills that are manifested at the patient’s side rather than through textbooks or formulas. The study emphasizes that informal learning on the job and experience through one’s work are essential to developing these critical-thinking behaviors. 33
The implications for practice are that educators should develop innovative pre-service teaching approaches and enterprising learning experiences on the job that prepare novice practitioners for informal on-the-job learning. Specifically, educators should focus on identifying what experience teaching techniques are possible. 33 This includes strategies that simulate or accelerate the development of tacit, practical knowledge that typically comes from clinical experience. 33 Well-structured clinical rotations and internships represent critical opportunities to provide students with authentic workplace experiences where they can develop practical wisdom and situated judgment under mentorship. They embody the kind of experience teaching techniques Goodfellow recommends. 33
Furthermore, educators should place more emphasis on the importance of experience, expertise, and reflection in professional practice to facilitate critical thinking. 33 Since Goodfellow found that years of experience correlate with higher self-assessment in troubleshooting, decision-making, and anticipating, educational strategies should incorporate robust clinical rotation programs and extended internship experiences that leverage experiential learning when targeting novice practitioners. These experiences help students develop practical knowledge, time management skills, and mental rehearsing abilities that expert therapists possess. Such capabilities are best acquired through hands-on patient care rather than classroom instruction alone. Second, the lower performance in specific domains such as interpretation, evaluation, deduction, and numeracy highlights areas where RT curricula may need enhancement. Problem-based learning, case studies, simulation, mind mapping, and explicit critical-thinking instruction have all shown promise for developing these skills in healthcare education.34–37 Third, the ethnic differences observed suggest a need for culturally responsive teaching approaches and additional support for participants from diverse backgrounds. Inclusive educational practices that address potential barriers to critical-thinking development are essential for ensuring all participants can achieve their full potential.
Several limitations should be considered when interpreting these results. First, the use of the HSRT-N alone, without the originally planned clinical simulation assessments, provides a partial picture of participants’ abilities. The COVID-19 pandemic necessitated this methodological change, but future research should incorporate performance-based measures of clinical decision-making to complement standardized critical-thinking assessments. Beyond the methodology change associated with COVID-19, the pandemic may have also affected the participants’ actual education and training in their programs. The widespread shift to remote and hybrid instructional formats substantially altered the curriculum delivery and face-to-face learning environment. This shift may have affected the students’ learning and comprehension of respiratory therapy content in multiple ways. We do not know the full impact these education changes may have had on the development of critical-thinking skills of respiratory therapy students and specifically the participants of this study. Additionally, the convenience sampling approach may limit generalizability, as participating programs and participants may differ systematically from those who did not participate. Another limitation is the potential influence of program-specific factors not controlled by this study, such as curriculum design, teaching methodologies, and clinical education models. These variables could affect critical-thinking development independent of degree type.
Future research should address these limitations and explore additional questions raised by our findings. Longitudinal studies tracking critical-thinking development from program entry to several years post-graduation would provide valuable insights into how these skills evolve over time. Mixed-methods research incorporating both quantitative assessments and qualitative exploration of decision-making processes would offer a more comprehensive understanding of critical thinking in respiratory therapy practice. Studies examining the relationship between critical-thinking abilities and actual clinical performance would help determine the practical significance of the differences observed. Additionally, intervention studies testing specific educational strategies for enhancing critical thinking in respiratory therapy participants could inform evidence-based educational practices.
The Aiken et al 13 study offers a compelling methodological example for respiratory therapy research. By systematically linking nurse education levels to measurable patient outcomes across hundreds of hospitals, the authors generated evidence that directly informed workforce policy. A similar outcomes-based research agenda is needed in respiratory therapy, one that connects RT educational preparation to concrete clinical metrics such as ventilator-associated events, weaning success rates, and hospital length of stay. Encouraging practicing respiratory therapists to engage with and apply current research evidence to patient-care decisions will be essential to building this evidence base. This not only supports academic progression, but supports advancing the profession’s standing, scope of practice, and recognition within an increasingly complex and competitive healthcare environment.
Conclusion
This study provides evidence that critical-thinking abilities, as measured by the HSRT-N, do not differ significantly between associate and baccalaureate degree respiratory therapy participants about the time of graduation. Our findings suggest that the case for academic progression in respiratory therapy may need to be justified on grounds other than critical-thinking enhancement alone. The observed differences based on ethnicity highlight the importance of addressing educational equity in respiratory therapy programs. As the profession continues to evolve in a complex healthcare environment, ensuring that all respiratory therapists develop strong critical-thinking skills remains essential, regardless of degree pathway.
Footnotes
Acknowledgements
We want to thank Julie Perretta for writing the clinical simulations we planned to use with the study.
Author contributions
Christopher Russian was involved in the study idea, IRB submission, subject recruitment, data collection, and manuscript development.
Jonathan Waugh was involved in the study idea, subject recruitment, data collection, and manuscript development.
Gregg Marshall was involved in the study idea, IRB submission, subject recruitment, and manuscript development.
Crystal Dunlevy was involved in the study idea, subject recruitment, and manuscript development.
Charles Gutierrez was involved in the subject recruitment, data collection, and manuscript development.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the AARC Vision Grant.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.