
Abstract
Performance anxiety among musicians and music students has been widely addressed, but far less attention has been given to examining the rates and characteristics of broader mental distress in this population. This study examined depression and anxiety in music students at one university. A considerable number of students reported symptoms indicative of anxiety or depression. Even though prevalence rates were not markedly different than those described in the literature for other university students irrespective of major, the high rate of untreated anxiety and depression among the music students is concerning. Music educators can help prepare their junior high and high school–aged students for the stressors of university music study by helping them develop coping strategies, fostering awareness of anxiety and depression as common and treatable conditions, and promoting acceptability of seeking treatment when necessary.
Over the past decade or so, directors of university counseling centers have expressed growing concern that the number of students seeking treatment for mental health concerns may be rising and have similarly noted that student mental health problems are more severe compared with those reported by previous generations of students (Benton, Robertson, Tseng, Newton & Benton, 2003; Erdur-Baker, Aberson, Barrow, & Draper, 2006; Hunt & Eisenberg, 2010; Kitzrow, 2009; Soet & Sevig, 2006). It may be that more students with serious mental health problems are able to attend university than ever before because of both the opportunities assured through the Americans with Disabilities Act and the efficacy of the newer Selective Serotonin Reuptake Inhibitor (SSRI) drugs (Gallagher, Gill, & Sysko, 2000; Hunt & Eisenberg, 2010; Rudd, 2004; Sharkin, 2004). Alternately, it may be that the rate of problems is not actually higher, but more students are seeking treatment, likely due to a gradual lessening of stigma surrounding mental illness and in response to educational campaigns bringing attention to mental health issues as treatable complaints (Berger, 2002; Blanco et al., 2008; O’Connor, 2001; Sharkin, 2004). At any rate, university and college counseling centers are increasingly called on to provide treatment or referral for more students who have significant degrees of psychopathology rather than primarily focusing on career guidance and developmental problems as has historically been the case (Pledge, Lapan, Heppner, Kivlighan, & Roehlke, 1998).
College students face many developmental challenges that might complicate or precipitate mental distress, including living alone for the first time, long-distance relationships with significant others, learning time management and independent living skills, balancing demands of jobs and school, living up to parental expectations, peer pressure, sleep deprivation and fluctuation in sleep patterns, and concerns about gaining employment after graduation. They may also be struggling with financial challenges, coming to terms with sexual identity, and alcohol and/or drugs (Kadison & DiGeronimo, 2004; Robotham, 2008). Mental health disorders (depression, anxiety disorders, bipolar disorder, schizophrenia, substance use, eating disorders, and many others) typically first present themselves between the ages of 18 and 25 years, (Kessler, Berglund, et al., 2005).
Depression and anxiety, among various categories of mental disorders, have been the focus of many studies, given their suggested role in the development of suicidal ideation and suicide attempt in this population (Garlow et al., 2008; Kisch, Leino, & Silverman, 2005). The Centers for Disease Control and Prevention identifies suicide as a leading cause of death in 20- to 24-year-olds, behind accidents and homicides. More teens and young adults die by suicide than from all other illnesses combined. One in every 12 American college students makes a suicide plan (Kadison & DiGeronimo, 2004).
Prevalence of anxiety and depression among university students is high. Blanco et al. (2008) found that 12% of college students were suffering from an anxiety disorder and 11% from a mood disorder. Soet and Sevig (2006) found a 14.9% depression rate, and an anxiety rate of 5.9% among their university student participants whereas Kessler, Chiu, Demler, and Walters (2005) documented an anxiety disorder rate of 18.1% and a mood disorder (including depression) rate of 9.5%. Eisenberg, Gollust, Golberstein, and Hefner (2007) estimated the overall prevalence for any anxiety or mood disorder was 15.6% for undergraduates and 13% for graduate students.
Rates of unreported and untreated depression and anxiety tend to be very high in any university student population, ranging from 50% to more than 80% (Blanco et al., 2008; Hunt & Eisenberg, 2010; Eisenberg et al., 2007) with fewer than half of the students screening positive for major depression or anxiety disorders receiving mental health services. Although more students are seeking treatment for depression and anxiety than in previous years (Benton et al., 2003), it appears that most students suffering from depression and anxiety still do not seek treatment.
Stressors Encountered By University Music Students
In addition to the stressors faced by all university students, music students face a number of challenges that may affect their mental health and well-being. Music is a highly competitive professional field, with many applicants auditioning for a limited number of positions. This competitiveness can be quite pervasive throughout the musician’s career, from the audition process to gain admission to elite precollege programs, university, or conservatory of choice, to competing for a limited number of professional positions. Dews and Williams (1989) pointed out that music demands a high level of perfection from those who hope to be successful at it, perhaps more than any other artistic discipline. Music performance requires a high level of constant discipline and exposure to criticism, both from self and others, throughout the career, and Dews and Williams concluded that this preoccupation with perfection might be mentally disruptive to the music student. More recently, Hunt and Eisenberg (2010) noted that perfectionism may play a role in how much stress students perceive as a result of their college studies. This observation has obvious implications, considering the high level of performance expectations that go along with pursuing music degrees. Perfectionism has long been vilified as a major source of psychological distress giving rise to maladaptive behaviors. Additionally, perfectionism has been linked to physical complaints. Jabush and Altenmüller (2004) found that musicians suffering from focal dystonias (e.g., involuntary, disruptive spasm that occurs in an isolated part of the anatomy and is evoked only by playing the instrument) had higher rates of perfectionism and specific forms of anxiety in comparison with healthy musicians. However, it is important to note that perfectionism can, in fact, play an adaptive role in psychological adjustment (Rice, Leever, Chrisopher, & Porter, 2006). In other words, a desire to strive for perfection, kept in proper balance, can actually motivate musicians toward the highest levels of performance.
Musicians must also cope with the heightened arousal that surrounds performance. Performance anxiety, a state anxiety condition, has been the focus of many studies and is beyond the purview of this article. State anxiety is experienced for relatively short periods of time by most if not all individuals in response to specific stressors. Abnormally high amounts of state anxiety can be disruptive and pathological, as occurs in music performance anxiety. In contrast to short-term state anxiety, trait anxiety may be defined as a predisposition to maintain longer term anxiety in anticipation of events, or to perceive higher levels of stress from situations, relationships, and events. It is worth noting that several studies (Kenny, Davis, & Oates, 2004; Lehrer, Goldman, & Strommen, 1990; Osborne & Kenny, 2008) have documented that many individuals who suffer from performance anxiety (state anxiety) also have trait anxiety. Kenny et al. (2004) postulated that perhaps an environment of constant evaluation heightened trait anxiety. Hyun, Quinn, and Madon (2006) found that there was a positive correlation between competition between students in an academic program and self-reported needs for mental health care. It has also been suggested that musical giftedness and higher trait anxiety might be related in some unknown way (Kenny et al., 2004).
Stressors related to music study are not only experienced by performance majors. Music education students also face distinct stressors related to their field of study. Conway, Eros, Pellegrino, and West (2010) identified struggles among instrumental music education majors with time management and a fear that individual performance development must be sacrificed in favor of academic coursework as major concerns. Music education students were frustrated that their accomplishments were not as visible or as readily acknowledged as those of performance majors. Bernhard (2005) suggested that there is a need to equip university music education students with interpersonal and intrapersonal communication skills to equip them as professional music educators. Intrapersonal strategies suggested included time management and organization, strategies for studying, and healthy habits with regard to sleep, diet, and exercise. Learning to effectively relate to peers, family, and figures of authority were suggested as interpersonal skills to cultivate.
Several studies have suggested that a high degree of internalization and identification with discipline of study may contribute to emotional problems in music students (Dews & Williams, 1989; Spahn, Strukely, & Lehmann, 2004). In a study comparing students majoring in music, premedical studies, psychology, and physical education in Germany, music students were least able to detach themselves from their course of study. Notable characteristics distinguishing music students were their high ambitions, strong commitment to their course of study, and identification with their chosen discipline from the very beginning of their university study. Musicians personally identify with their work and are not always able to separate themselves from it, which in turn may lead to a narrowing of other interests in life (Spahn et al., 2004). However, in contrast, Chesky and Hipple (1997) found lower rates of emotional and alcohol problems in university music students in comparison with students in other disciplines. Music majors reported significantly fewer social and emotional problems than their nonmusician peers.
Spahn, Richter, and Zschocke (2002) found that 12% of university music students experienced playing-related psychological problems, and approximately half of their participants reported that all the problems they experienced had psychological components. Yet 79% of the participants who reported psychological problems had not sought professional help. Even though music students are significantly more likely to believe they can take actions to positively influence their health in comparison with both medical students and a normed population sample (Spahn, Burger, Hildebrandt, & Seidenglanz, 2005), they are apparently no more likely, and perhaps even less likely, to seek professional help for problems of a psychological nature than nonmusicians.
As discussed, rates of depression and anxiety are quite high among all university students. However, given the additional stressors of university music training, it seems reasonable to investigate whether university music students might report even higher rates of anxiety and/or depression than other university students. The purpose of this study is thus to determine whether prevalence and treatment rates of depression and anxiety among music students at a single institution are comparable with, or higher than, rates documented by other studies in other university student populations.
Method
Participants
Participants (n = 287) consisted of music majors and minors at a large state institution in the Midwestern United States with a total student enrollment of approximately 24,000. The School of Music has approximately 250 undergraduates and 150 graduate students, is fully accredited by the National Association of Schools of Music, and has three wind ensembles, an orchestra, a large marching band, two jazz bands, four large choral ensembles, an opera program, and numerous smaller ensembles and chamber music groups. Participants consented to participate in the study in accordance with institutional review procedures. The mean age of participants was 21.19 years, with a mode of 18 years. Gender representation was almost equal, with 53.5% males and 46.5% females. The majority (62.9%) were instrumentalists, and 37.1% were vocalists. Many (40.4%) were in their first year of university study post–high school; 18.4% were in their second year, 14.5% in their third year, 6.4% in their fourth year, 6.4 % in their fifth year, 6.0% in their sixth year, and 7.8% in their seventh year or beyond. Most of the participants (91.6%) had never taken any class on the topic of musician health.
Most of the participants (93.8%) were pursuing a music degree (undergraduate degrees, Master of Music degrees, and doctoral degrees), 5.8% were music minors, and less than 1% was undeclared. Data from music minors and unspecified degree students is reported along with that of the music majors because of the relatively small number of these students and similarity of stressors. Music minors at the institution face many of the same stressors and health risk exposures as those pursuing music majors during the first and second years of study, including the necessity of being accepted into private lessons by audition and participation in ensembles and performances. It is also presumed that both the undergraduate music minors and majors have experienced similar formative experiences (i.e., participation in high school–level ensembles, performances, private instruction in instrument/voice, etc.) during their precollege music education.
Procedure
This study analyzed data from one area of a lengthy questionnaire developed to examine health states and behaviors as well as participants’ perceptions regarding the impact of these behaviors. Multiple revisions, informed by the input from a typical 20-year-old music student, were undertaken to eliminate redundancy and enhance comprehension on the part of participants. The questionnaire was then outsourced to a separate department of the institution—Surveys, Statistics, and Psychometrics—for further editing, formatting, and printing to enhance reliability. Since this study was limited to the prevalence of anxiety and depression, only data from the questionnaire subset dealing with mental health states were examined.
Participants were asked about several mental health conditions, including depression, anxiety, bipolar disorder, obsessive–compulsive disorder, and phobia. Since the overall treated and untreated prevalence of bipolar disorder, obsessive–compulsive disorder, and specific phobias was negligible, this study further restricted itself to those items related to depression, anxiety, and generalized anxiety disorder (GAD, which is a specific type of anxiety disorder characterized by at least 6 months of excessive anxiety and worry about a variety of events and situations). Participants were asked to select (yes/no) whether they had ever received medical or psychological treatment for the condition (lifetime-to-date prevalence), and if they had, whether treatment for each condition had included medication.
Participants were then asked to select symptoms they experienced from lists in separate inventories and indicate impact of symptoms on daily relationships and functioning. This was done to screen for presence of conditions for which treatment had not been sought by participants. Symptom inventories were based directly on criteria and symptoms listed in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 1994), the current reference standard used by mental health practitioners in the United States. Separate inventories listing symptoms of depression, panic/anxiety, and GAD were used. Depression symptoms listed for adults were combined with those listed for adolescents because of the ages of participants in this study. All symptoms discussed throughout the relevant section of the DSM-IV were listed, with one exception: psychomotor agitation or slowing down was omitted during vetting of the questionnaire by an age-typical music student, who expressed concerns that this symptom might not be meaningful or could be misinterpreted by participants. DSM-IV criteria were occasionally “exploded” to capture various aspects of a symptom and recombined during data analysis. For example, with regard to depression, the DSM-IV lists sleep disturbances as a symptom. The symptom inventory on the research questionnaire included difficulty falling asleep, difficulty staying asleep, and sleeping much more than usual. Responses for these three items were later combined into a single item—sleep disturbances—and considered as a single symptom. This was done to ensure that the participants considered various ways sleep disturbance might manifest, while avoiding artificially inflating the number of symptoms experienced for each condition during data analysis. For panic/anxiety and depression symptoms, the reporting time frame was restricted to the past year, and for GAD symptoms, participants were asked whether there had ever been a period of time of 6 months or greater when they experienced the symptom listed on most days, consistent with DSM-IV criteria. Since how a person is affected by symptoms is a critical consideration in diagnosis of mental health conditions, participants also indicated how much distress each symptom reported caused—none, mild, moderate, or severe, using wording derived directly from the DSM-IV. Finally, participants were asked to rate their perception of how their overall mental health affected their musical practice and/or performance on a Likert-type scale from negative 5 to positive 5, with −5 = very negatively, 0 = not affected, and +5 = very positively.
The university where the survey was conducted maintains a convocation hour in its weekly academic schedule, during which all students taking a private lesson for credit meet to participate in lectures, workshops, or performances. All participants completed the research questionnaire during the same convocation hour, in the same physical location, during the fourth week of the academic term. Since participants were asked to report health states and symptoms over a minimum period of 12 months, timing of data collection was not deemed to be crucial, and date of questionnaire administration was chosen according to availability.
To prevent potential measurement error or bias, all surveys were completed via anonymous instrument at the same place and same time. Research participants are generally more likely to respond to questions of a sensitive nature given repeated assurance of anonymity (Aday, 1996). No names were collected on the questionnaires and students were assured that all raw data would be entered by an independent source to maintain anonymity. Data were analyzed to determine simple frequencies for all items, and interactions between items (e.g., number of reported symptoms by impact of symptoms) were then examined using a Microsoft Excel spreadsheet.
Results
Anxiety
Participants were asked to select anxiety symptoms experienced over the previous year and were also asked to indicate whether each symptom caused “a mild, moderate or severe amount of distress or interfered with school, work, or relationships”. Over the entire research sample, 11.6% (33/285) indicated that they had experienced no symptoms over the previous year. Of those who reported symptoms, 52.8% (133/252) reported one to four symptoms that interfered with function to Mild degree whereas 14.7% (37/252) selected five or more symptoms that interfered to a Moderate/Severe degree. It should be noted that it was possible for participants to select numerous symptoms of varying severity. For example, while one individual may not have selected any symptoms, another individual may have reported more than five Mild anxiety symptoms and also one to four Moderate/Severe symptoms. Experiencing five or more symptoms is a DSM-IV criterion for anxiety, with severity or impact of symptoms on functioning representing another important criterion. Table 1 summarizes number of symptoms and their impact on functioning in those who had and had not sought treatment for anxiety. Numbers of symptoms according to severity totaled more than numbers of participants in treatment categories because of possibility for reporting multiple symptoms of different severities.
Symptoms and Impact Among Participants Treated and Not Treated for Anxiety (12-Month Rate).

Note. Percentages of total research sample, rounded to nearest tenth. Numbers of symptoms according to severity total more than numbers in treatment categories because of reporting of multiple symptoms of different severities.
Only 9.8% (n = 28) of participants had ever previously sought treatment for anxiety conditions (lifetime-to-date) prior to study participation, with 18 taking medication as part of their treatment. There were 257 no responses with regard to previous lifetime-to-date anxiety treatment, and two nonresponses. With regard to anxiety symptoms experienced in the previous year, two thirds of those who had previously received treatment for anxiety had experienced symptoms, with 11 participants reporting zero to four symptoms and 15 reporting five or more symptoms with moderate to severe impact on functioning. Of the 257 participants who indicated that they had never been treated for anxiety, 12.5% (32/257) indicated that they had experienced five or more symptoms of anxiety in the previous 12 months that negatively affected their functioning or relationships, addressing both symptom and severity criteria of the DSM-IV. This suggests an overall 12-month rate of anxiety disorders of various kinds of 16.49%, with 11.23% of participants suffering anxiety symptoms but not seeking treatment.
A separate inventory was included to estimate the rate of GAD. In keeping with DSM-IV criteria, the distinguishing factor for this specific anxiety disorder on the research instrument was whether generalized anxiety symptoms selected were experienced on most days for a period of 6 months or greater at any point lifetime-to-date (unlike inventories for depression and other anxiety symptoms, which specified a 12-month time frame). Of 157 participants who selected GAD symptoms, 39 reported five or more symptoms persisting 6 months or greater (one of the DSM-IV criteria for GAD). A total of 57 participants selected GAD symptoms on the inventory and indicated that symptoms negatively affected their functioning, and 43 of that number had not sought treatment. Sixteen (16) of these untreated participants reported experiencing five or more symptoms that negatively affected their function for a period of 6 months or greater, satisfying all criteria of DSM-IV for GAD. Of the 28 (9.8% of total sample) who indicated seeking treatment for anxiety of any type (lifetime-to-date), half had been negatively affected by symptoms listed on the GAD inventory for a period of 6 months or greater. Considering number of symptoms and negative impact on function, the number of treated and nontreated participants meeting all DSM-IV diagnostic criteria for GAD may be as high as 8.4%.
Depression
Of the 285 respondents to items regarding depression, 37 (12.98%) reported having received treatment for depression at some point previously (lifetime-to-date). Of those who had received treatment, 13 (4.6%) reported experiencing five or more symptoms during the previous year that affected quality of life to a Moderate/Severe degree, with an additional 9 (3.2%) reporting one to four symptoms with milder impact. Most participants (249/287) had never been treated for depression. However, 144 of those untreated had experienced one to four symptoms of depression during the previous 12 months that had mildly interfered with their function. More notably, 21 (7.4%) of the untreated participants experienced five or more symptoms that negatively affected function to a Moderate/Severe degree over the previous year, meeting the DSM-IV symptom and impact criteria for depression. The 12-month rate for treated and untreated participants meeting all DSM-IV criteria for depression was 11.9% (34/285). Fourteen participants (4.9% of total sample) reported previous suicide attempts (lifetime-to-date). Responding to the Likert-type scale question regarding perception of mental health, nearly one quarter of study participants reported being negatively affected by their mental health state: 23.2% reported musical practice and performance negatively affected by mental health; 20.6% reported that the impact was neutral; and 56.2% reported positive impact of mental health on their music making.
Discussion
In this sample of university music students, rates of anxiety and depression are roughly equivalent to, or even perhaps slightly below those documented in other studies in general university student populations. The lengthy questionnaire used for this study was developed to support a number of separate research studies examining health states and behaviors of music students while only requiring a single data collection and contained items in several sections pertinent only to musicians. For this reason, the questionnaire was not distributed to students in other fields of study, and thus direct comparison of these music students with a peer group of nonmusic students is not possible. However, it is reasonable to consider how percentage rate compares with rates of anxiety and depression documented in other studies. Additionally, the same university participated the previous fall in the National College Health Assessment–II (NCHA) conducted by the American College Health Association, which sampled all students, irrespective of academic major. Findings from the NCHA study documented a 12-month treatment rate of 10.4% for depression and a 12-month treatment rate of 10.3% for anxiety. Those seeking treatment for both depression and anxiety represented 5.9%. Additionally, 13.9% indicated that they had felt too depressed to function, and 18.8% indicated they felt overwhelming anxiety. The 12-month anxiety treatment rate documented by the NCHA in 2008 for all students, irrespective of academic major, was within a percentage point of than the lifetime-to-date treatment rate documented by this study in 2009 among the music students at the same institution. Similarly, the lifetime-to-date treatment rate of 12.98% for depression documented in this study is quite comparable with the 12-month rate documented in the NCHA study (American College Health Association, 2009).
Given the rigors of music training, including a tendency to strongly identify the self with the study of music, the need for continuously imposed self-discipline, long hours, and continuous competition with peers, it is encouraging that higher incidences of mental health psychopathologies among these music students were not observed. Even so, nearly one quarter of participants reported being negatively affected by their mental health. It is clear that many of these students did not seek treatment for these issues, as shown in Table 2. Untreated participants satisfying criteria for each condition studied outnumbered those who were treated. While a high rate of nontreatment was expected, the nontreatment rates observed in this study (Table 2) are notable when viewed alongside the nontreatment rates observed in the separate NCHA study conducted at the same institution the previous fall (Table 3). The low rate of treatment-seeking observed in the music students as compared with nonmusicians may echo the findings of Spahn et al. (2002), and points to a continuing need to promote awareness of indicators and potential impacts of depression and anxiety among music students and to increase cultural acceptability of seeking treatment for these conditions.
Music Students in This Study.
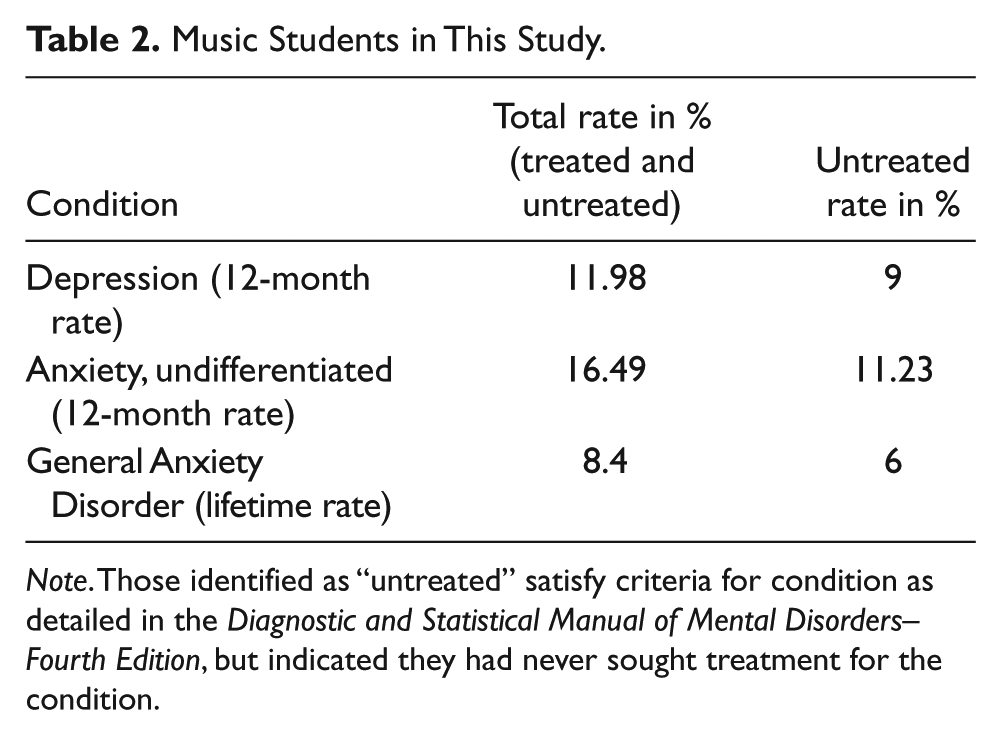
Note. Those identified as “untreated” satisfy criteria for condition as detailed in the Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition, but indicated they had never sought treatment for the condition.
All Students in National College Health Assessment Study, Previous Fall.
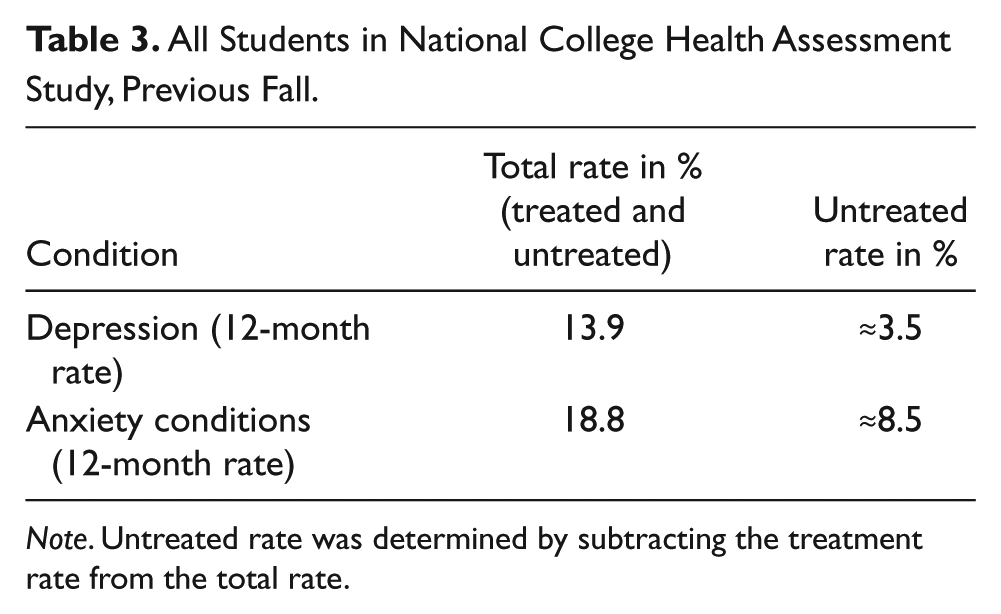
Note. Untreated rate was determined by subtracting the treatment rate from the total rate.
It would be illustrative to study whether or not mental disturbances, such as diagnosable anxiety and/or depression, directly lead to attrition within the field of music. Determining whether or not stressors and/or rates of anxiety and depression differ significantly as music students progress through different levels of their training might help university administrators and professors develop more efficacious interventions. It would also be quite instructive to examine various paradigms for teaching music students to cope with the mental/emotional demands of the profession and consider whether or not they result in behavioral changes or influence numbers of mental health disturbances among university music students.
Findings from this study should not be considered to represent actual rates of diagnosed depression or anxiety. Data were self-reported, and health history was not verifiable, and thus there exists a possibility for over- or underreporting. However, this is a concern that exists with any health screening inventory. This concern was addressed through providing comprehensive and specific lists of symptoms for participants to choose from and specifying the time frame for reported symptoms. Since the larger questionnaire containing the subset of data examined in this study was lengthy, there exists the potential for participant fatigue or inattentiveness. However, questions regarding mental health conditions and symptoms were located toward the beginning of the questionnaire. Participants were also given ample time to complete the questionnaire, and they received academic credit for the convocation during which the questionnaire was administered.
While the findings from this study are of direct interest to university music educators, these observations also have implications for the precollege music teacher. Given the high rate of nontreatment for these conditions, a logical first step would be for music educators to simply promote awareness of depression and anxiety as treatable conditions. Music educators are often highly influential in the lives of their junior high and high school students. Simply acknowledging these mental disorders with the same level of concern given to physical injuries affecting musical participation might encourage students to seek treatment when needed. It is important for music educators to be mindful of their limitations (they are usually not trained mental health care professionals) and to always respect student privacy and confidentiality. However, since music educators work closely in mentoring relationships with their students, they may well be the first to notice developing problems. Music educators can certainly make students aware of available support and counseling services and might also directly assist school counselors in endeavors such as administering screening inventories and offering programs to learn to cope with stressors. Fostering projects and interactions where students learn to identify musical, organizational, or social problems and develop productive solutions can help students learn to effectively cope with actual or potential challenges and develop their interpersonal and communication skills while addressing specific musical objectives. For example, a high school band director might form small groups to support practice. Students could identify the problems they encounter in their practice—such as scheduling difficulties, lack of motivation or focus, lack of musical progress, physical barriers, and so on—and address these challenges with help from their peers and guidance from the teacher. With regard to performance, providing procedural guidance for memorization (if applicable), tips for coping with the physiological and psychological stressors of performance, and numerous opportunities to participate in small-stakes performances are advisable to build success and self-efficacy. Music educators can also greatly assist students by providing them with simple time management skills and strategies, invaluable skills that are frequently neglected in students’ formal education.
There is a growing call to educate music students about occupational health and safety risks. Educating students about mental health issues and where to seek treatment is a vital part of advancing comprehensive health for musicians. By teaching music students to identify and specifically address challenges inherent in the discipline, and helping them identify their own unique triggers for mental distress, music educators can contribute to overall student success and well-being at all levels of musical training.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Arts & Humanities Enhancement Fund sponsored by the Office of Research and Economic Development, University of Nebraska–Lincoln.