
Abstract
Ascending pharyngeal-vertebral anastomosis has been identified by angiography of the carotid artery in several cases. We present a case of ascending pharyngeal-vertebral anastomosis that was found incidentally in computed tomography angiography of the ascending pharyngeal artery. Images revealed that the anastomosis formed through the hypoglossal branch of the neuromeningeal trunk. The anastomosis seemed to be associated with hypoplasia of the right vertebral artery. Interventional radiologists should be aware of this dangerous anastomotic route of the APA to the VA. Discovery of hypoplasia of the major intracranial arteries before intra-arterial chemotherapy or embolization in head and neck area may avoid subsequent complications.
Among the branches of the external carotid artery (ECA), the ascending pharyngeal artery (APA) plays a major role in extracranial-intracranial anastomosis, since an ascending pharyngeal-internal carotid anastomosis can occur via the inferior tympanic branch, meningeal branch, jugular branch, and carotid branch (1, 2). Such anastomoses have been identified by angiography of the carotid artery (3-5). Several reports have also shown that the APA can form an anastomosis with the vertebral artery (VA) via the musculospinal branch or hypoglossal branch, also through use of angiography of the carotid artery (6, 7). Here, we present a case of APA-VA anastomosis that was found on computed tomography angiography (CTA) of the APA, and we discuss the relationship between this anastomosis and VA hypoplasia.
Case report
A 57-year-old man was admitted to our hospital with intermittent epistaxis. One year earlier, he had received radiotherapy with systematic chemotherapy for a right maxillary tumor, followed by a total maxillectomy with microsurgical anastomosis between the right superficial temporal artery and a vascularized flap used as a reconstructed deep inferior epigastric artery (DIEA).
Magnetic resonance imaging showed a recurrent maxillary tumor in the right nasal cavity, and transarterial chemoembolization was planned for control of the epistaxis. An interventional procedure was performed via a transfemoral route. The reconstructed DIEA, a right maxillary artery, and a right ophthalmic artery arising from the internal carotid artery (ICA) were identified as feeding arteries. To search for another feeding artery, we also performed selective injection of the right APA. Digital subtraction angiography (DSA) images did not reveal tumor staining, but showed incidental visualization of the right VA (Fig. 1). On CTA of the APA, the vessel entered the hypoglossal canal and connected with the right VA (Fig. 2). These findings were compatible with APA-VA anastomosis via the hypoglossal branch of the neuromeningeal trunk.
Anteroposterior (a) and lateral (b) views of an ascending pharyngeal arteriogram showing the V4 portion of the right vertebral artery (arrow). The hypoglossal branch (open arrow), neuromeningeal trunk (arrow head), muscu-lospinal branch (double arrow heads), and the inferior tympanic branch (open arrow head) are well visualized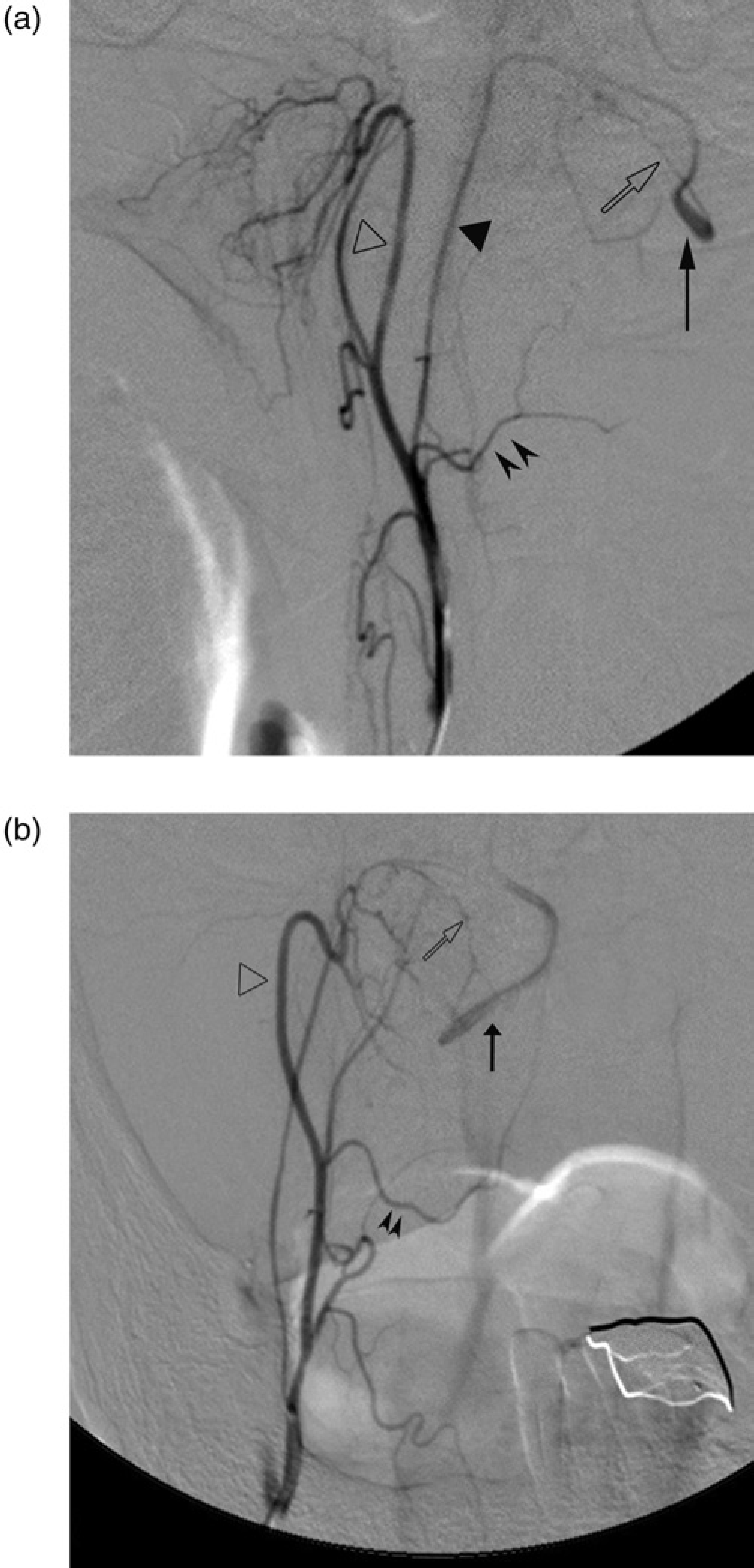
Computed tomography angiography of the ascending pharyngeal artery (APA) showing (a) a branch of the APA passing through the hypoglossal canal (arrow heads) and (b) a branch of the APA connecting to the right vertebral artery (arrow)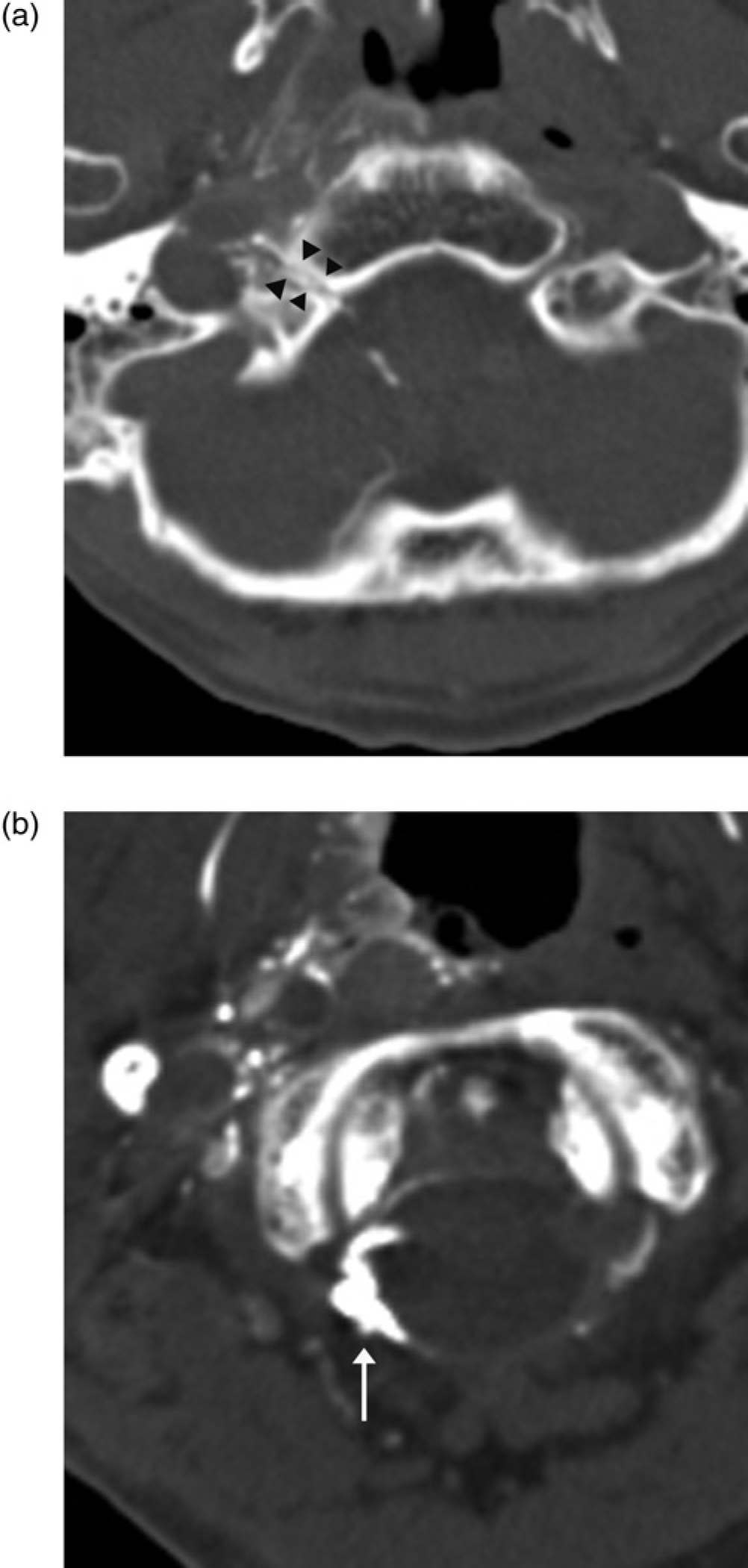
Transarterial chemotherapy was performed through the reconstructed DIEA, internal maxillary artery, and ICA. Embolization of the reconstructed DIEA and internal maxillary artery was also performed using Gelfoam® particles.
The epistaxis diminished and the patient was discharged. We retrospectively reviewed a CT angiogram obtained by preoperative intravenous contrast-enhanced CT, which showed hypoplasia of the right VA.
Discussion
The APA usually arises from the proximal portion of the ECA and divides into two major trunks: anteriorly, the pharyngeal trunk, which mainly supplies pharyngeal tissue; and posteriorly, the neuromeningeal trunk, which supplies the dura and lower cranial nerves of the skull base (6, 8). The two main divisions of the neuromeningeal trunk are the jugular and hypoglossal branches. The former enters the cranial cavity through the jugular foramen, supplying the ninth, 10th, and 11th nerves (7). The latter extends to the meninges of the posterior fossa and the vasa nervorum of the 12th cranial nerve. The hypoglossal branch has a medially descending branch that anastomoses with the VA at the third cervical space, forming an extradural arcade dorsal to the body of the dens of C-2; this constitutes the arterial arcade of the odontoid process (7-10). Since the routes of these two branches are closely aligned, the jugular branch can mimic the hypoglossal branch. Consequently, identification of the hypoglossal branch is sometimes difficult on DSA images (10).
Several reports have described cases of APA-VA anastomosis, but few have discussed angiography findings. Although most of these reported anastomoses were detected by angiography of the carotid artery, whereas we revealed this anastomosis by CTA of the APA. Extra-intracranial anastomotic channels are usually not visible on routine catheter angiographies, but are seen under the following circumstances: (a) with increased intra-arterial pressure (e.g. during embolization procedures or super-selective injections; (b) in the presence of high-flow shunts, as a consequence of the ‘sump effect’; and (c) as collateral routes in cases with occlusions of the major intracranial arteries (11). In our case, the ascending pharyngeal-vertebral anastomosis was not visible on a right external carotid arteriogram, but was seen after selective injection into the APA. This indicates that increased intra-arterial pressure contributed to visualization of the anastomosis. In addition, hypoplasia of the right VA might have contributed to formation of the anastomosis as a collateral route. In fact, it is known that hypoplasia of the VA causes carotid artery-VA anastomosis, occipital artery-VA, persistent trigeminal artery-VA, and persistent primitive artery-VA (12-14). Whereas the lower cranial nerves are supplied from the vertebral arteries, the supply to their foraminal parts is mainly through the neuromeningeal trunk of the APA (7, 8, 11). Damage of the VA area in interventional procedures for the APA has not been reported, but there is a risk of such damage.
In conclusion, we have described a case of APA-VA anastomosis accompanied with hypoplasia of the VA. CTA of the APA showed that the anastomosis entered the hypoglossal canal and connected with the right VA. Interventional radiologists should be aware of this potential anastomotic route of the APA to the VA, especially under a condition of hypoplasia of the VA detected on preoperative images.
Footnotes
None