
Abstract
Objective:
The aim of the Australian WorkHealth Program - Arthritis was to develop and test an education program designed to minimise risk of arthritis and prevent or reduce absenteeism and presenteeism. The objective of the current study was to use a wide-ranging, multifaceted and interactive approach to engage with stakeholders in order to inform the content and delivery of the intervention.
Methods:
Methods used to inform program design included a concept mapping workshop, interviews, surveys, a steering committee and an industry advisory group. Engaging with a wide range of stakeholders in multiple ways early in program development allowed for the comparison and verification of data to obtain a better overall picture of the needs of participants. It also offered the opportunity to share ‘ownership’ of the program with stakeholders by generating a program that was tailored to their ethos and needs.
Results:
The stakeholder engagement process was instrumental in building commitment to the program and establishing an overarching model of action. Interview and survey data indicated that awareness of arthritis was low and musculoskeletal disorders more generally were of greater concern. It was agreed that programs should be relevant, evidence-based, involve senior management education, incorporate a business case, and involve tailored implementation and marketing strategies. The qualitative preparatory phase as well as all the engagement work was key to informing program design.
Conclusions:
The approach taken in this study has the potential to inform a wide range of workplace interventions. Engaging with a wide range of stakeholders in multiple ways from program inception allowed for the comparison and verification of information to permit the generation of a model of intervention that had the highest possible chance of success. It offered the opportunity to not only define program content and implementation processes, but to build genuine ‘ownership’ of the program.
Introduction
In an attempt to address work disability related to musculoskeletal disorders (MSDs), the Australian WorkHealth Program – Arthritis was commissioned by the Commonwealth Department of Health and Ageing as a project under the Better Arthritis and Osteoporosis Care (BAOC) initiative. The aim of the Australian WorkHealth Program – Arthritis was to develop and test an education program to minimise risk for disease onset and prevent or reduce osteoarthritis (OA)-related absenteeism and presenteeism (being unproductive at work).
Arthritis and related MSDs are Australia's leading causes of disability and chronic pain and a leading cause of work disability. OA is the most common form of arthritis, affecting 1.3 million Australians (6.5% of the population) and is one of the most costly medical conditions to industry, estimated to be second only to heart disease in working days lost through disability.1,2 Muchmore et al. 2 estimated that those with joint disorders had a 4% lower annual work output than those without these disorders, mostly due to absence from work. They also found arthritis to significantly increase the likelihood of workers’ compensation claims. Work disability can have serious consequences for individuals, for example a reduced quality of life, loss of social identity, and even indefinite or permanent exclusion from work.3,4
It is anticipated that the number of people with disability due to arthritis will nearly double by 2020, with half of this increase occurring among those in their highest earning years (45–65 years old). 5 This represents a major public health problem in western industrialized countries, with a recent report estimating productivity costs in Australia to be over $4.1 billion in 2007. 3
There are independent and multiple risk factors for arthritis, other MSDs and related disability.6,7 Modifiable risk factors for OA include injury, obesity, occupational factors, sports participation, joint malalignment, muscle weakness, nutritional factors and hormonal influences.8,9 Industry sectors associated with increased risk of arthritis include construction, transport, and agriculture.10,11 In general, it appears that high psychological demands, low decision authority and low social and management support are most strongly linked to MSD-related work disability.12–15
As MSD-related work disability is a multifactorial problem with no single solution, interventions must take into account physical, psychological, social, clinical, occupational and organizational factors, e.g. repetitive movements, obesity, smoking and job strain.16,17 They also need to be evidence-based, effective, practical, whole of system (with a focus on policy, people and practices), appropriate for a wide range of settings, and endorsed by a wide range of stakeholders.18,19
The press for evidence-based health interventions has led to increased debate about the nature of this evidence 19 and how utilization of this evidence might be enhanced. 20 The term ‘knowledge exchange’, or ‘information exchange’ incorporates the idea of knowledge as a dynamic set of understandings shaped both by researchers and by stakeholders whose decision-making is informed by research. 21 This understanding highlights the importance of engaging key decision makers from the initial stages of program development, an approach which has been shown to increase uptake and application of research information. 18 It is argued that a dynamic and participatory approach is required to generate the knowledge, will, enthusiasm and, critically, commitment to program success. Stakeholders need to see tangible changes in the program that directly result from their participation in the program development.22–28
Using a framework in which organisations are conceptualised operationally as communities, we attempted to negotiate with industry and government sectors to develop a shared strategic direction for the Australian WorkHealth Program – Arthritis. We used a combination of methods to inform program design, planning and evaluation in an effort to apply the strengths of an evidence-based approach to the program while considering issues of context, policy, implementation and sustain-ability. This paper reports on the findings of that process.
Methods
Approaches used to inform program development included steering committee consultations, a 47-person concept mapping workshop, one-on-one interviews, a written survey, and an industry advisory group. 29 The study was approved by the University of Melbourne Human Research Ethics Committee.
Steering committee consultations
The first phase of stakeholder engagement involved the formation of a Steering Committee comprising 15 members including a professor of general practice (who was nominated as the chairperson of the committee), a consultant ergonomist, an occupational physician working in industry, a representative of the Arthritis Foundation, two consumers, a union representative, an educational change consultant, an Australian Safety and Compensation Council representative and a representative of the Department of Education, Employment and Workplace Relations. The Chief Investigators of the project, who included a businessman, a rheumatologist, a health program evaluator, a health services researcher and a physiotherapist, were also members of the Steering Committee. Project members were actively engaged in these meetings as well. Six face-to-face meetings were held between August 2007 and February 2009. At each meeting, members were asked to participate in decisions about program content and implementation, particularly in problematic areas. Notes were taken at all meetings, and minutes circulated, with ongoing contact where specific concerns were canvassed.
Concept mapping workshop
The second phase of stakeholder engagement and consultation involved a structured concept mapping workshop with 47 key informants from across Australia. 29 The concept mapping process generated program principles, service delivery modes and constituent elements of the education program de novo, bringing these ideas together as a broadly conceptualized theory of action. As planned, this concept map became the overarching organizer for all planning, implementation and evaluation work.
Consultation interviews and follow-up surveys
Representatives of a number of organizations were contacted and asked to participate in consultation interviews. The purpose of the interviews was to identify how these key people described employee health issues, current health and wellbeing programs and potential for improvement. Representatives of larger organizations with more experience in work health programs and industries with workforces identified as having increased risk of MSDs were approached directly, with the aim of category sampling sufficient for thematic saturation rather than comprehensive or exhaustive sampling. 30 An attempt was made to obtain diverse responses to ensure the data were sufficiently robust to cater for diversity.
A total of 46 Victorian-based organizations were approached with a request for an interview. Of these, one declined due to work commitments, 24 did not respond to either e-mail or telephone requests and three companies who agreed were in the same industry category and so only one was interviewed. In all, interviews with 28 individuals from 19 organizations were carried out (see Table 1). Interviewees were those that had Occupational Health and Safety (OHS) or Human Resources as a key part of their role. A responsive approach was used, enabling the interviewees to talk freely and informally about their health and wellbeing activities, although some specific questions were used to guide the conversation and ensure effective use of the time available. Questions were asked about the following areas:
The level of awareness of and impact of arthritis on the workforce; Current workplace health and wellbeing activities; Enablers of successful implementation and outcomes; Barriers to successful implementation and outcomes; Desirable changes in workplace education and support.
Characteristics of organisations participating in survey

Not interviewed in the consultation interview phase
The consultation interviews were analysed for major themes and from this, a follow-up questionnaire was developed based on the themes from the interviews and sent to the interviewees. Respondents were asked to verify the existing data and add in any missing information. All but two of the respondents completed the follow-up questionnaire.
Findings from consultation interviews and follow-up surveys
Level of awareness of and impact of arthritis on the workforce
The workforce demographics were varied across and within organizations. Fifteen interviewees worked for companies with multiple sites. All organizations reported either an ageing workforce overall or in particular sectors. Only two organizations nominated arthritis as a specific health concern and these were both manufacturing companies. In this sample, representatives of organizations with a predominantly white collar workforce did not view arthritis as an issue while representatives of organizations with a large proportion of manual workers were more likely to view it as a problem. Most respondents viewed arthritis as a disease of ageing. However, 15 organizations nominated MSDs (predominantly back pain) as a key concern. Other key concerns included fatigue, stress and mental health.
All organisations collected data on worker's compensation claims and absenteeism rates and most collected data on lost-time injury rates and staff turnover. However, there was little or no data relating to the impact of arthritis on the workforce, unless this was mentioned in documentation relating to a WorkCover (agency charged with prevention and compensation of occupational accidents and diseases) claim.
Current workplace health and wellbeing activities
All organizations surveyed had some health-related policies and practices. The most common of these related to mandated OHS and included occupational safety, manual handling, injury prevention and first aid. Only nine organizations had a specific health and well-being policy.
The organizations adopted a variety of approaches to their initiatives, with three utilising external services only to provide pre-packaged programs, three using only internally-designed and developed programs and 11 organizations using a combination of the two. The most commonly used services were counsellors, ergonomists, psychologists, consultants/coaches, occupational physicians and nurses, general practitioners and dieticians. Most of the larger companies subscribed to an outsourced Employee Assistance Program with a mental health/counselling focus. The most common program delivery methods included online information provision, one-off education sessions on specific health topics, leaflets, posters, DVDs, interactive workshops, team games or challenges and health expositions or “roadshows”. Employee health screening was a relatively common intervention with 10 organizations conducting executive health checks and seven conducting health risk assessments. Task analysis by ergonomists was carried out by 10 organizations.
The majority of health promotion activities focused on risk reduction with an emphasis on weight loss, physical activity, alcohol/drug education and stress management. The most commonly addressed disease topics were cardiovascular disease, diabetes and mental health. Only three organisations specifically provided information on arthritis. All respondents understood, endorsed and tried to implement the notion of joint employer/employee responsibility in health, with an emphasis on self management.
Many programs involved the use of incentives provided by the organization, such as sports store vouchers and gym memberships. Competitions such as 10,000 steps (www.10000steps.org.au) were common and the competitive nature of the program was seen as an incentive to participation. One organization proved a notable exception to this. They had a strong belief that asking employees to pay for services related to health and well-being activities such as influenza vaccination increased participation.
Enablers of successful implementation and outcomes
When interview participants and survey respondents were asked about the factors most likely to lead to successful implementation and outcomes of health education programs, the most important enablers of employee participation were given as management support, evidence of need, relevance to organization and strong business case (See Figure 1).
Ten most important features of a successful workplace health promotion program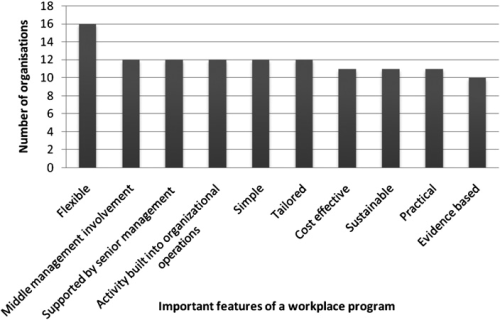
The larger organizations reported that they did not need specific data that evidenced a business case in order to introduce health education initiatives whereas smaller organization were more likely to report the need for this. There was a general acceptance of the links between health and productivity. A number of representatives stated that their health promotion activities were part of the ‘employee value proposition’ or corporate image and played a role in making the organisation more likely to attract new and retain existing staff. In companies with a largely blue collar workforce, a primary motivation for health education was to reduce absenteeism, lost time injury rates, workers compensation claims and insurance premiums.
Flexibility emerged as an important theme. In particular, the need to accommodate the differing needs of staff members was identified, most commonly where there was a geographically diverse workforce or one with very different job functions, such as a large urban central office and rural manufacturing operations. Respondents whose organizations had existing programs mentioned the need for new programs to integrate and partner with existing programs and providers.
Tailoring, defined in this situation as the need for a program to be built into and augment current organisational structures and operations, was also seen as important with 12 respondents nominating this as a key feature. Nine respondents mentioned the need for programs specifically designed for their industry. Twelve respondents nominated senior and middle management support as a feature critical to success. Ten respondents nominated the education of senior management as a vital first stage critical to success of a program. The use of internal marketing to promote health and wellbeing initiatives was highlighted by eight respondents (mostly larger organizations), with several developing their own corporate branding for programs.
Barriers to successful implementation and outcomes
Fourteen interviewees nominated insufficient time during work hours as the major barrier to individual participation in health and wellbeing initiatives. Other commonly cited barriers included organizational time constraints, remote worksites, financial issues and lack of resources.
Industry Advisory Group (IAG) consultations
The aim of the IAG was to incorporate industry expertise to ensure the ongoing success of the program in multiple ways. This is an essential part of a knowledge translation framework that incorporates the reciprocity involved in developing evidence-informed interventions. Eleven representatives were invited to become members of the IAG (see Table 1). Individuals were invited to join the IAG if they had considerable experience in managing health and wellbeing programs or were members of organizations seen as important in influencing industry practices. The majority of these individuals were recruited from the consultation interview phase of the project. All accepted the invitation to join. Three other members joined the IAG, two of whom were representatives of industry organizations and one (a representative of a mining company) who was invited to join after the interviews were completed. Three dynamic 3-hour long IAG meetings were held between March and July 2008.
At the first meeting, the project was introduced to the group and the purpose of the group explained. This was followed by a discussion using Nominal Group Technique 31 of the key benefits of a whole-system health program in the workplace. Each participant was asked to nominate an answer in turn, with responses refined during this process to eliminate duplicates and multiple concept answers. These were recorded on a whiteboard, ranked individually and then the group as a whole numbered the benefits in order of priority. The second IAG meeting involved a report on project progress and feedback on needs assessment procedures and questionnaires as well as a discussion on overcoming barriers to implementation. The third meeting involved a discussion of the program content and delivery approaches. Notes were taken at all meetings, and minutes were circulated.
Findings from IAG meetings
Discussion confirmed a low level of awareness of arthritis as a specific health issue and a general agreement of the need for a broad health and wellbeing program rather than one focused on a specific health issue. Overall, the top priority of work health programs was assigned to the need to recruit new and retain existing employees, followed by factors relating to improved productivity, including:
Decreased turnover; Decreased staff absenteeism; Decreased staff presenteeism; Decreased indirect costs associated with staffing; Decreased return-to-work costs; Decrease in injuries; Decrease in severity of musculoskeletal problems; Delay of onset of musculoskeletal problems.
Increase in ongoing employee engagement (e.g. as measured through climate surveys) was also given priority as were improvements in employee quality of life. The need for increased monitoring and management of efforts in workplace health was also mentioned as a priority. The most important enablers of participation were given as management support, evidence of need, relevance to organization and strong business case. The IAG meetings were characterised by open, lively discussion of views, including differences of opinion. A particular feature of the meetings was the readiness to offer opinions and critically appraise the content and direction of the project taken by the project team when IAG members did not consider that it met their needs.
Discussion
We used a novel combination of methods to inform the generation of the content and delivery approaches of a workplace intervention designed to minimise the development and impact of arthritis, a complex chronic condition. The wide-ranging, multifaceted approach ensured negotiation with diverse stakeholders and detailed the way forward for the intervention. It is argued that this approach has the potential to inform a range of workplace interventions as engaging with a wide range of stakeholders in multiple ways from the inception of program development allowed for the comparison and verification of information obtained to generate a well-informed picture of the needs across industry participants. It also offered the opportunity to define program content and implementation processes, and to build genuine ownership. 23
Synthesis of the findings revealed that participating organisations saw the health and wellbeing of their employees as important, principally due to the need to attract and retain employees and maintain or improve productivity. However, awareness of arthritis as a specific issue was low, although MSDs more broadly were seen as more of a concern, particularly in organizations with a high proportion of manual workers.
Participants nominated a number of features critical to success of programs, including business case, tailoring, flexibility, senior management involvement, effective marketing, joint employer/employee responsibility and expert validation. The main barriers were considered to be organizational and individual time constraints and lack of resources. Relevant, needs-focussed interventions, senior management education, development of a good business case, effective, evidence-based initiatives, tailored implementation and marketing were seen as effective ways of overcoming barriers.
Industry interviewees were all strongly committed to their work, saw a need for health and wellbeing programs, cared about the wellbeing of their employees and were keen to pass on their experience. Each interview provided a different perspective on workplace health and wellbeing and provided useful insight into the issues faced in particular industry settings. While there were individual differences, the overall views of the Steering Committee, workshop participants, interviewees and IAG broadly matched, allowing us to be reasonably confident of the conclusions drawn and the directions the program should take.
This research sought to explore ways of working productively and efficiently with stakeholders in the development of a complex intervention. Such programs are multifaceted and operate within already complex systems, presenting challenges in development and evaluation. 32 It is only relatively recently that there has been an acknowledgement that complex interventions require greater attention to early phase piloting and development work, integration of process and outcome evaluation and tailoring of interventions to specific contexts.18,33,34 It is argued that the methodology described here offers a way to engage a wide range of stakeholders as equal partners, rather than as docile research subjects or grateful and passive recipients of research findings. Each method described here offered unique insights as well as the opportunity to reinforce or challenge findings from elsewhere.
This interactivity and flexibility is exemplified by the change in direction that arose as a result of the consultation interviews and IAG meetings. There was a low level of awareness of arthritis as a specific health issue. Only one (an occupational physician) had a clear understanding of the nature of the disease and only two mentioned arthritis as a specific health concern, although MSDs more broadly (predominantly back pain) were seen as more of a concern. The majority of the interviewees noted the need for a broad health and wellbeing program as they felt that focusing on one health problem (i.e., arthritis) would not be seen as cost-effective. Some participants thought that promoting a program using the term “arthritis” would discourage participation as those without diagnosed disease (particularly younger people) would not view it as a concern. There is strong evidence that any intervention which is not viewed as having a clear advantage in terms of effectiveness or cost-effectiveness, is unlikely to be adopted. 18 Therefore, as a result of the extensive consultation, it was decided to focus on musculoskeletal disorders more broadly and to base the program elements firmly on a model of musculoskeletal disability prevention and management that incorporates psychological and social factors as well as those relating to the medical facts of the disease. This ‘biopsychosocial’ approach appears particularly appropriate due to evidence that the factors affecting the onset and course of disease are so removed from the disability outcomes. 35 Variables that appear to be associated with arthritis pain and disability include: learned helplessness, depression and negative affect, stress, coping, self-efficacy and social support. 35 A program focusing on such elements has broad appeal and the potential to benefit those with a number of different health problems.
The desirable aspects of health education programs identified by participants (see above) are all reflected in the program logic model generated in the initial workshop. 29 There was considerable variation in how these elements were defined and viewed in different organisations and job roles. In larger organisations there was a general acceptance of the links between health and productivity, although it has been noted in other studies that while many employers understand that a healthy workforce is a more productive one 36 they may not be convinced that health promotion programs can affect their bottom line or may not know which program elements are more important or suitable for their workforce. 37 A number of representatives stated that their health promotion activities were part of the ‘employee value proposition’ or corporate image and played a role in enabling the organisation to attract new and retain existing staff. This finding is echoed by the list of benefits generated by the IAG who nominated attracting and retaining staff as the top key benefits of a work health program (see Figure 1). In companies with a largely blue collar workforce a primary motivation for health education was to reduce absenteeism, lost time injury rates, workers compensation claims and insurance premiums. This is also reflected in the priorities of the IAG. Initial consultation interviews highlighted the need for program content and implementation to be tailored to the needs of the organisations. In response to these findings, and in order to obtain a detailed knowledge of the organisation a set of needs assessment or “situational analysis” tools were developed. These were reviewed at the second IAG meeting and feedback from this meeting incorporated into the final questionnaires and interview protocols.
The most commonly cited barriers to participation were individual and organizational time constraints and lack of resources. However, it has been noted that different levels of management view barriers differently. Linnan et al. 38 questioned over 1,000 managers from 23 manufacturing worksites and found that senior managers (vs. line supervisors) were significantly less likely to believe space or cost were barriers and were less likely than middle managers or line supervisors to believe production conflicts were a barrier to offering health promotion programs. The interviewees and IAG members consulted here were a mix of middle and senior management with OHS or human resources responsibilities. It is possible that a similar consultation with line supervisors would provide alternate views. However, the discussion with the IAG enabled us to tap into their considerable experience in overcoming barriers. Relevant, needs-focussed interventions, senior management education, development of a good business case, effective, evidence-based initiatives, tailored implementation and marketing were seen as effective ways of overcoming barriers.
While every effort was made to incorporate a wide range of views during the consultation process, due to the enormous variation in industry categories, organisational structures and health-related practices it was not possible to capture the full picture. To obtain a more comprehensive view, it is suggested that further consultation be carried out with representatives of small and medium-sized organizations and with employees across different company levels, including line supervisors, lower level employees as well as senior management (Chief Financial Officers and Chief Executive Officers).
Adopting the responsive approach to the consultations allowed the conversation to be informally structured however, it was vital to be time efficient as interviewees were all busy and were unable to spare more than 30 minutes to one hour per interview. Given more time it would have been useful to explore some aspects further such as, the reasons why companies adopt different approaches and the impact of budgets on introducing new initiatives.
Conclusions
Engaging with a wide range of stakeholders in multiple ways from the initial stages of program development allowed for the comparison and verification of information obtained to ensure a comprehensive picture of the needs of industry participants. It also offered the opportunity to define program content and implementation processes, and to build ownership. Synthesis of findings revealed that organisations see the health and wellbeing of their employees as important, principally due to the need to attract and retain employees and maintain or improve productivity. However, awareness of arthritis as a specific issue was low although MSDs more broadly were seen as more of a concern, particularly in organizations with more manual workers. It is therefore proposed that programs aiming to prevent and manage arthritis should therefore adopt a broader MSD focus. They should be relevant, be needs-focussed, involve senior management education, incorporate a business case, be effective, incorporate evidence-based initiatives and involve tailored implementation and marketing strategies.
Footnotes
Acknowledgements
The authors would like to thank Angela Wood, Deanna Norris, the project Steering Committee members, including the chair, Professor Richard Reed and the members of the Industry Advisory Group.