
Abstract
Background
Nocturia is common but the clinical assessment of its severity and cause rarely involves any biochemical analysis. Investigating the cause of nocturia needs to be informed by the overall 24 h fluid and solute excretion patterns. The aim of this study was to establish a practical method of monitoring the renal excretion of water and solutes over a complete 24 h cycle.
Methods
The excretion patterns of sodium, volume and osmoles were assessed in 89 healthy control subjects over a 24 h period by sampling each voiding from the 24 h collection and then using the total urine creatinine as the denominator. A group of 21 patients under investigation for sleep-disordered breathing (SDB: a group of disorders known to increase the risk of nocturia) were also studied to determine comparative excretion patterns.
Results
Reference excretion patterns of sodium, volume and osmoles were described. Patients under investigation for SDB had overall a significant (P < 0.001) increase in urine sodium excretion at night (nocturnal natriuresis) matched by an increased osmotic excretion and accompanied by a significantly increased nocturnal urine volume (P < 0.001).
Conclusion
Breaking down a 24 h urine collection into voided aliquots provides practical information on the pattern of water and solute excretion. Such patterns may assist in identifying the underlying mechanism of significant nocturia in individual patients presenting with this symptom, and could be used as a method of monitoring treatment.
Introduction
Nocturia is defined as the number of voids recorded during a night's sleep; each void is preceded and followed by sleep. 1
Nocturia is common with 14.2% of the adult population reporting >2 voids/night, and the prevalence of the symptom increases with age with no gender differences. 2 The presentation and investigation of nocturia may involve one or more of many medical specialties including general practice, urology, endocrinology, gynaecology, neurology, cardiology and respiratory medicine.
Measurements performed by the clinical biochemistry laboratory inform the clinician on the classification of daytime polyuria; yet the involvement in the classification of nocturia is currently minimal. Detailed characteristics of nocturia require quantification of solute and water excretion using commonly defined and comparable scales to improve classification.
The two fundamental determinants of urinary frequency are bladder volume and urine production rate. The normal human adult bladder has a maximum capacity of between 600 and 800 mL but the subjective urge to micturate often begins when the contained volume is between 150 and 300 mL and increases in intensity as the contained volume approaches the maximum capacity. The normal urinary frequency ranges from four to eight voidings per 24 h, strongly tempered by social requirements, and the pattern of voiding generally excludes the sleeping period. A reduction in the bladder volume capacity will result in daytime frequency and will eventually progress to include nocturia: this presentation is the domain of urologists and this type of nocturia is best described as night-time frequency.
The normal adult urine volume ranges from 800 to 2800 mL per 24 h, again strongly tempered by social requirements but ultimately dependent on the precise demands of fluid balance. Therefore, excessive primary fluid intake for whatever reason will result in daytime polyuria and, if balance requires, nocturia. Nocturia, however, can occur without daytime polyuria and is then best described as nocturnal polyuria. Normal physiology reduces night-time fluid output proportionally to day-time. The normal adult osmotic excretion ranges from 700 to 1500 mmol/24 h contained within the urine volume and the excretion pattern also favours day-time excretion. 3 Thus, nocturnal polyuria may be due to excessive nocturnal water excretion, excessive nocturnal osmotic excretion or a combination of both.
The medical approach to the investigation of the presenting symptoms of nocturia will vary with specialty. The most basic approach is a subjective recall of the number of voiding episodes interrupting sleep, although this approach is widely recognized as inaccurate. A more systematic approach used in urology is to require the patient to formally complete a frequency/volume chart. No standard time period is universally applied to the frequency volume chart and can range between 24 h and seven consecutive days. In some protocols, the patient assesses or measures the volumes of fluid consumed and in all protocols the patient records the time and assesses the volume of urine passed. 4 However, no urine is usually retained, hence the composition of voided urine is unknown.
In this study certain aspects of the frequency volume chart are incorporated into a urine frequency/composition test. For this test the individual under investigation is requested to collect a 24 h urine but to retain an aliquot of every recorded and timed urine passed. Using the 24 h urine creatinine excretion as the denominator, the pattern of urine volume and solute excretion can be constructed over the 24 h period and comparatively expressed as a cumulative percentage of the total excretion. For the individual patient with nocturia, comparison with the normal excretion patterns can then be made to establish causation.
Materials and methods
Study populations
A control group of 89 adult individuals (43 males, 46 females, average age [±SD] 45.7±14.5 y) were identified in good health and without any known condition predisposing to nocturia or polyuria. No night shift workers were included and all controls had standard sleep patterns, i.e. awake during the day and sleep at night.
A patient group of 21 adults (16 males, 5 females, average age 55.4±7.7 y) under investigation for sleep-disordered breathing (SDB) by a standard sleep study attending the Gwent Sleep Centre were selected. Patients under investigation for SDB were recruited because of the known increased incidence of nocturia in this group of conditions 5,6 and were studied prior to the institution of any treatment regimen. Symptomatic nocturia was not assessed in the SDB group prior to study.
Procedure
Each participant was issued with urine frequency/composition test kit, which consisted of 20 × 30 mL plain screw-top plastic containers (Polycon tubes for aliquots), one disposable 1 L plastic jug, 2 × 2.5 L screw-top polypropylene bulk urine containers (24 h urine, no preservative), a detailed patient instruction sheet and a urine collection record chart (see Appendix with online article, found at
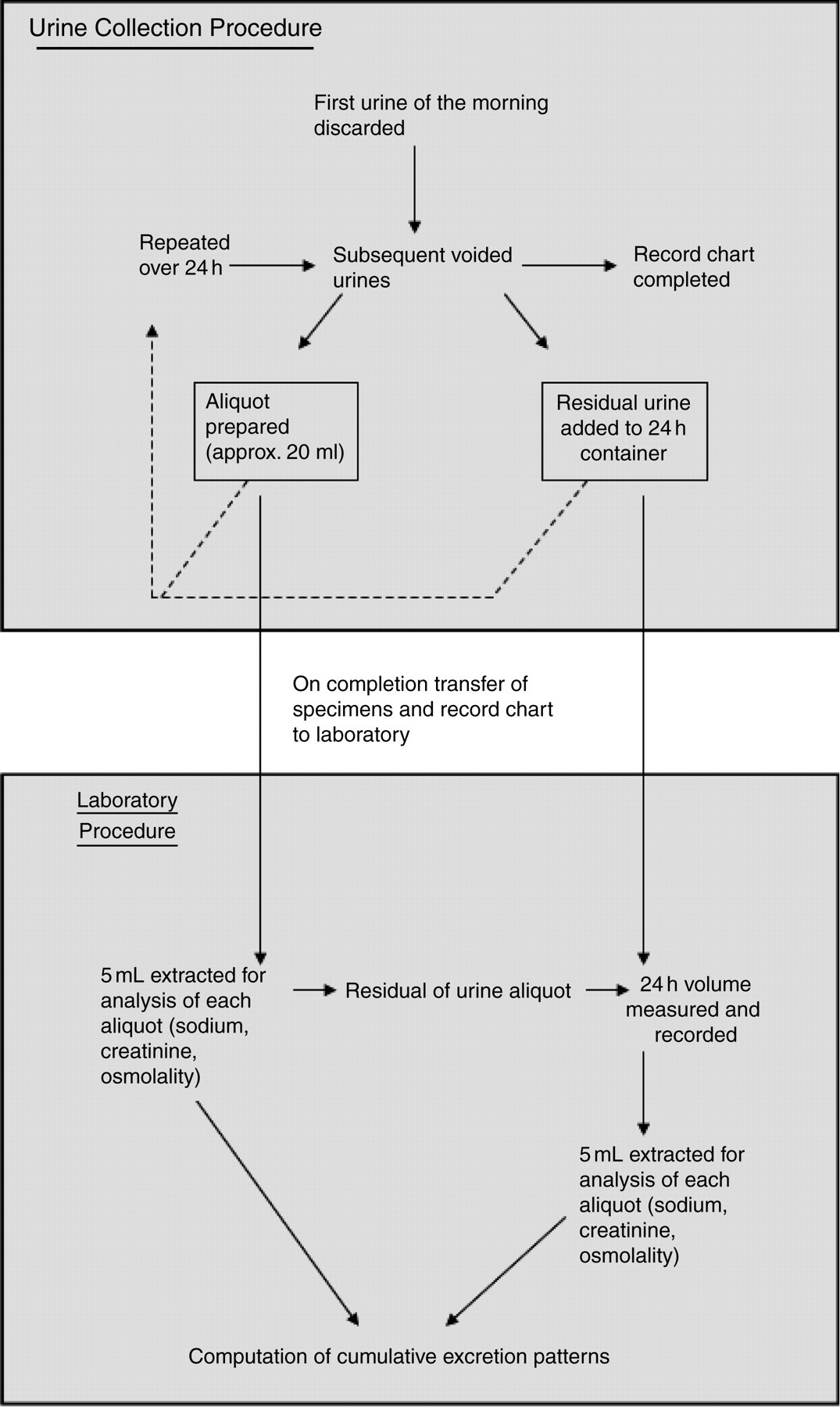
Flow diagram of the urine frequency/composition test procedures
All urine collections were made on an outpatient basis and the procedure commenced on arising day 1 when the first urine was discarded (time 0). Cumulative excretion commenced at this point. Each subsequent urine passed was collected and, after an aliquot had been saved, the remaining urine was added to the bulk container. All subsequent urines were collected in the same way, including all night-time voids, and the test was concluded on arising day 2 when the final urine was collected at the same time as the first discarded urine the previous day (time 24 h). The participant also completed the urine collection record chart identifying the precise times of voiding, indicating that an aliquot had been prepared and saved together with identifying the time of retiring to bed and the time of arising. Participants also recorded their height, weight and any prescribed medication.
Analysis
Urine analysis was by standard laboratory methods: sodium by Chemiflex® Integrated Chip Technology™ (Abbott Laboratories, Maidenhead, Berkshire) and creatinine by a rate-based Jaffe method – both analysed on the Abbott ci8200. Osmolality was measured by freezing point depression – Advanced Instruments Model 3300 (Advanced Instruments, Norwood, MA, USA).
Twenty-four hour urine volume was measured by tare weight (Ohaus Portable Advanced, Ohaus Europe GmbH, Nänikon, Switzerland).
Calculation of urine voided volume and solute excretion rates
The basis of the calculation is the relative constancy of the urine creatinine excretion rate. 7,8 The 24 h urine creatinine excretion provides the denominator and the time intervals between each voiding allow the creatinine excretion rate to be calculated. The creatinine concentration of each aliquot ascribed to the specific time interval then allows the predicted urine volume to be calculated for each voiding. Subsequently, the excretion rate and absolute magnitude of voided solute can then be calculated and expressed as a cumulative percentage of the total.
Interpolation of the cumulative percentage excretion patterns for each healthy subject and the division of the 24 h timescale into 10 equal parts permitted the estimation of deciles of cumulative excretion for each measured parameter; the 10th decile indicating the completion of collection (100% of cumulative excretion). Using this methodology, reference intervals for cumulative excretion throughout the 24 h period were constructed.
Calculated indices definitions
The following three indices of nocturia, as defined, were calculated for each participant: 9
Nocturnal voids: the number of voids recorded at night, each void preceded and followed by sleep.
Nocturia index: the volume of urine excreted during the nocturnal period divided by the maximum voided volume of the whole day.
Nocturnal polyuria index (%NP): the volume of urine excreted during the nocturnal period divided by the total urine volume excreted over 24 h, expressed as a percentage.
In addition to the above indices is added a fourth:
Nocturnal natriuresis (%NN): specifically identifies the proportion of sodium excreted during the sleep period: the sodium excreted at night compared with the total 24 h sodium excretion, expressed as a percentage.
Reproducibility
Ten of the control subjects agreed to repeat the urine collection on a separate occasion and the paired indices of nocturia were compared.
Statistics
Data were analysed using Microsoft Excel 2007 (Microsoft Ltd, Wokingham, Berks, UK) and Unistat® version 5.6 (Unistat Ltd, Maida Vale, London, UK). Data from the healthy subjects were tested for normality using descriptive statistics (mean, median, standard deviation [SD]) and the one sample Kolmogorov–Smirnov test (KS); skewness and kurtosis and visually using box and whisker plots. Any outliers were identified and eliminated if a result was >3 × interquartile range (IQR).
Differences between group means were tested parametrically by the t-test or non-parametrically, if necessary, using the Mann-Whitney U test. The critical level of significance was set at 0.05. Results are expressed as mean±SD or median (IQR).
Ethical approval
This study was reviewed and approved by the Gwent Research Ethics Committee. All controls and patients were fully informed of the study procedure and provided written informed consent.
Results
Table 1 shows the physical characteristics, 24 h excretions, nocturia indices and sleep periods for the control and SDB groups. The SDB group is older than the control group, having higher body mass index and tending towards higher 24 h excretion of sodium, volume and osmolality, but none of the absolute excretion quantities reach statistical significance. Within the SDB group, nocturia indices all demonstrate significant nocturia and nocturnal natriuresis (P<0.001), although the actual total sleep duration as recorded was not significantly different between the control and SDB groups, nor were there significant differences between the times of retiring to sleep or arising the following morning. The SDB group had an oxygen desaturation index (ODI: ≥4% decrease in oxyhaemoglobin saturation) 10 ranging from 2 to 129/h (median 19, IQR 51).
Characteristics of the control and sleep-disordered breathing (SDB) groups
Ni, nocturia index; %NP, nocturnal polyuria index; %NN, nocturnal natriuresis; BMI, body mass index.
Data are expressed as mean±standard deviation or median (interquartile range)
Figures 2a, b and c show, respectively, the box and whisker plots for the nine decile ranges of the cumulative excretion in the control group of sodium volume and osmoles. No results for any of the deciles exceeded 3 × IQR. The one sample KS for normal distribution was used to test the null hypothesis that the decile excretion patterns are normally distributed and the range of P values for each excretion pattern were: sodium (0.07–0.93), volume (0.13–0.98) and osmoles (0.12–0.96). Skewness and kurtosis were also not significant for any parameter.
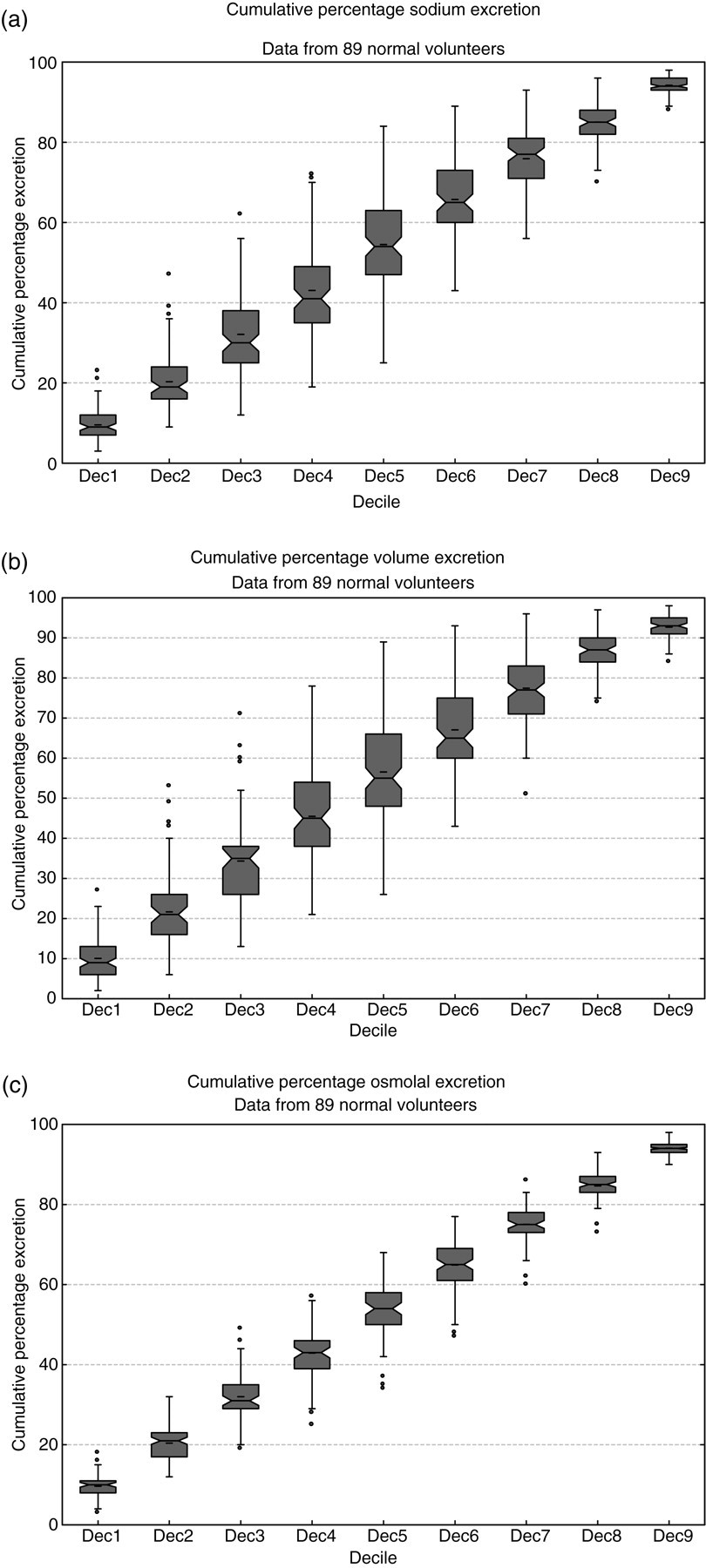
Control group cumulative excretion patterns showing box and whisker plots for each decile of (a) sodium, (b) volume and (c) osmoles
The 95% confidence limits for each excretion pattern of the control group are shown in Figures 3a, b and c for sodium, volume and osmoles, respectively. Also shown for comparison are the individual cumulative excretion patterns of the SDB patient group. There is considerable heterogeneity within the SDB patient group, and in comparison with the normal controls there is an overall shift towards nocturnal excretion of volume, sodium and hence osmoles.
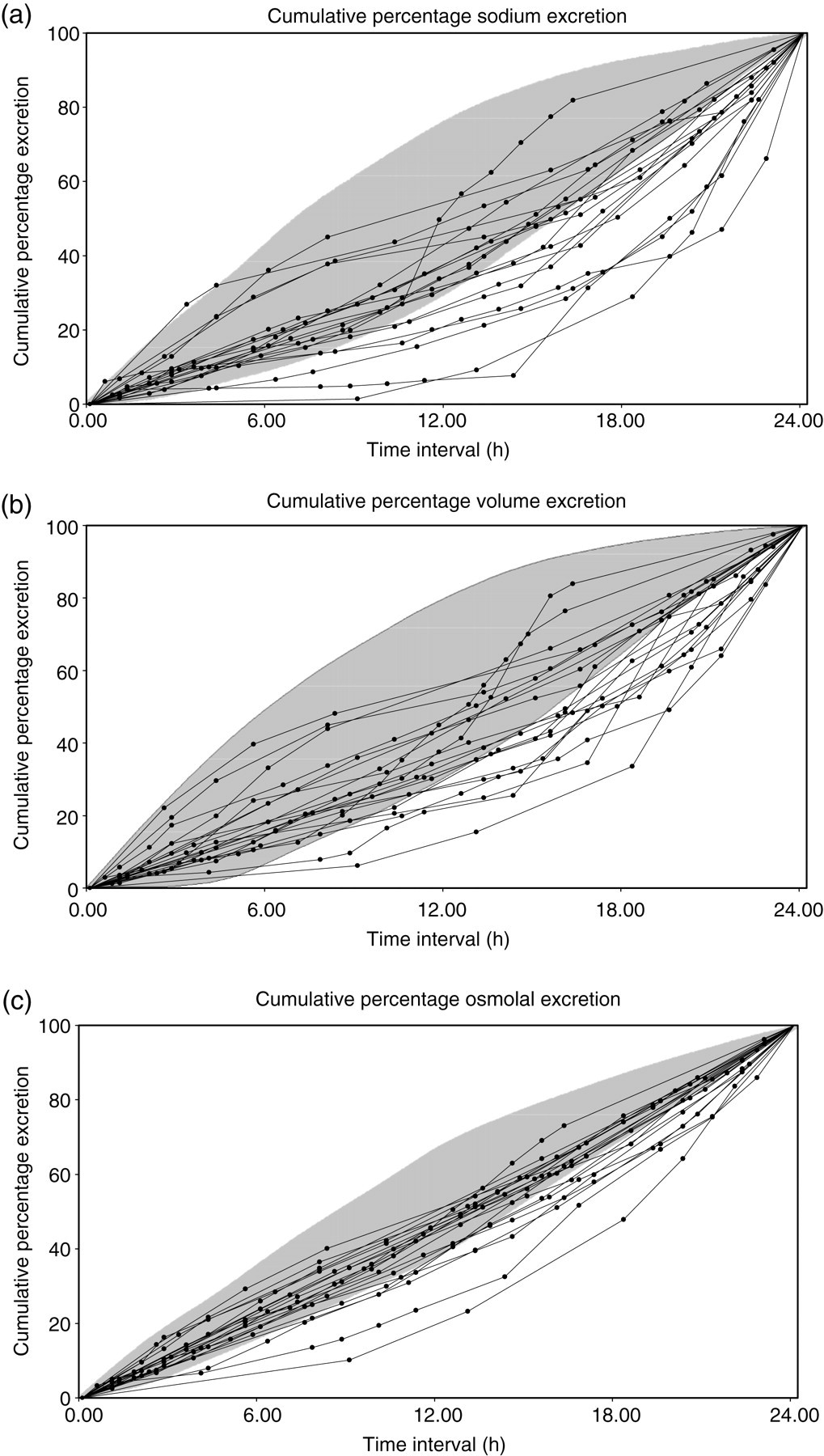
Control group 95% confidence limits excretion patterns (grey-shaded area). Also shown are the individual cumulative excretion patterns of the sleep-disordered breathing patient group: (a) sodium, (b) volume and (c) osmoles. Time interval measured from first morning urine
Table 2 shows the nocturia indices from two independent collections performed by the 10 control subjects. No significant differences were recorded in any parameter.
Nocturia indices from two independent collections of 10 controls
Ni, nocturia index; %NP, nocturnal polyuria index; %NN, nocturnal natriuresis
Data are expressed as mean±standard deviation or median (interquartile range)
Discussion
The systematic investigation of nocturia has been hampered for many years by the lack of accepted definitions, and the difficulties in obtaining accurate data particularly in the outpatient setting. Standard terminology now exists 1 and specified indices have been developed. 9 There remains, however, a reluctance to systematically investigate urine composition in this condition.
Over recent years in clinical biochemistry, every effort has been made to reduce the reliance on the 24 h collection. Such previous reliance has either been largely abandoned (estimated glomerular filtration rate versus creatinine clearance) or reduced to random or early morning collections relating the measured parameter to creatinine concentration (albumin, catecholamines, etc.). There is suspicion of the validity of biochemical parameters related to 24 h timed urine collections due to the difficulties of ensuring complete collection. 11 For any objective biochemical assessment of nocturia, however, it is necessary to compare water and solute excretion patterns between waking and sleeping periods over the whole 24 h period. It is important, therefore, to provide detailed instructions as to how the collection of samples for urine frequency/composition test is to be made, and the requirement for correct and honest completion of the diary. Nocturia can be seriously debilitating and patients often become obsessive when documenting their condition – thus the level of compliance in correct collection procedure is usually high.
The decision to use the 24 h creatinine excretion as a denominator of all other excretion rates (sodium, volume, osmoles) was taken following experience of observing data from traditional frequency volume charts – most patients are not skilled in precise volume measurements, and with nocturia this would require such measurements at several times during the night when sleep has been disturbed. Moreover, to establish composition using a complete collection of individual voids would require an unwieldy array of specimen containers.
There are undoubted errors in the derived excretion patterns regardless of collection errors. The use of creatinine measurements in the assessment of renal function has come under increasing scrutiny in recent years. In humans, creatinine in the serum is filtered by the glomerulus but significant tubular secretion also occurs mediated by an organic cation transporter (hOCT2). 12 Competition with other specific organic cations (e.g. cimetidine, dronedarone) can reduce tubular secretion of creatinine over the short term. In addition, the ingestion of meat and fish, and food products derived from these will, depending on the time eaten and thence metabolized, skew the excretion patterns based on creatinine outwith that time period. 13 Thus, if practicable, patients undergoing such an investigation should be advised to limit or abstain from meat and fish products during the collection period. These particular sources of error are common to any urinary parameter related to creatinine.
The excretion patterns of the control group confirm the physiological preference to limit nocturnal excretion of sodium, volume and osmoles at night (corresponding on average to the last 8 h or so of collection). The data from patients with SDB show a general shift of excretion from the waking to sleeping period – essentially a nocturnal natriuresis. This corresponds to haemodynamics of SDB that indicate a natriuresis induced by nocturnal elevation of plasma natriuretic peptides. 14 There is considerable intrathoracic negative pressure generated during obstructed apnoea events and negative pressure breathing is known to be a strong stimulant for natriuretic hormone release. 15 The magnitude of the symptom of nocturia will be dependent of the severity of the SDB and the prevailing sodium load for excretion – the latter accentuating the symptom if the daily sodium intake increases.
In conclusion, a practical reproducible method to monitor the renal excretion of sodium, volume and osmoles over a complete 24 h cycle is presented, and its application to the study of nocturia within a defined group of patients with SDB is made. The method may assist in identifying the underlying cause of nocturia in patients with this symptom and could then be applied further to objectively monitor treatment responses. Moreover, the principles of the method of study could be applied to any urinary constituent.
DECLARATIONS