
Abstract
We report the rare finding of a macro-alkaline phosphatase (macroALP) complex in a patient with a previously unexplained raised alkaline phosphatase activity. The clinical symptoms were persistent, daily diarrhoea for two months with blood in the stool. The patient was subsequently diagnosed with inflammatory bowel disease, specifically ulcerative colitis, following a rectal biopsy and colonoscopy. Two cases of macroALP associated with ulcerative colitis have been reported before, suggesting there could be an increased prevalence of macroALP in these patients.
Introduction
Tissue-specific alkaline phosphatase (ALP) isoenzymes are found in the bone, liver, kidney, intestine and placenta. Routine biochemical assays of serum ALP activity do not distinguish between the different ALP isoenzymes. However, specialized electrophoresis techniques can identify the ALP isoenzyme responsible for raised ALP activity (Figure 1).
The theoretical separation of ALP isoenzymes using the Sebia Hydragel 15 ISO PAL kit. Lectin is used to bind to any bone ALP present and prevent its co-migration with the liver and placental isoenzymes. ALP, alkaline phosphatase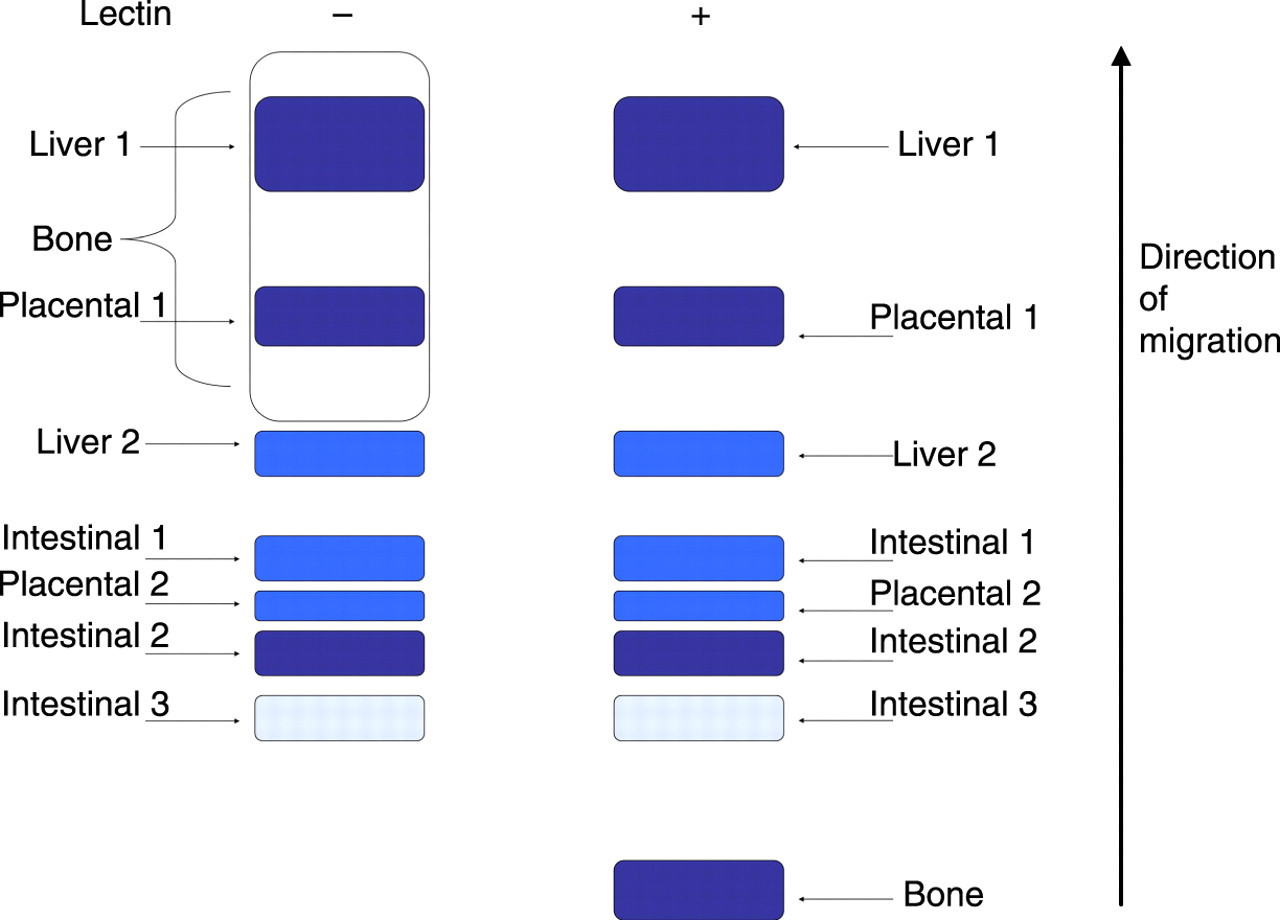
Raised serum ALP activity may be due to the liver ALP isoenzyme as a result of hepatic damage or cholestasis. Increased production of bone-specific ALP is a common reason for raised serum ALP activity, which can be caused by fracture and a number of pathologies affecting the bone, including Paget's disease, osteomalacia and bone metastasis. Serum ALP activity will also be raised in pregnancy due to the placental ALP isoform. Intestinal ALP is present in approximately 40% of normal subjects, with an increased prevalence in individuals with a B or O blood group and is more likely to be present after a meal with a high fat content. 1 Raised serum intestinal ALP activity is of uncertain clinical significance, but has been reported in patients with liver cirrhosis, diabetes, chronic kidney disease, and in bowel ischaemia and infarction. 2
Occasionally, increased plasma ALP activity will be due to an immunoglobulin-bound form of ALP (macroALP); the kidneys have a role in clearing ALP from the circulation 3 and so macroALP complexes have reduced clearance due to their high molecular weight compared with unbound ALP. Several such macroALP complexes have been reported, but they have no known clinical significance. 4–8 In general, the identification of macro-enzyme complexes is important to rule out pathological causes of raised serum enzyme activity and avoid unnecessary and potentially harmful diagnostic investigations.
MacroALP has been reported in two patients with ulcerative colitis, although it is not known if this is a coincidental finding or linked to the condition, and the specific ALP isoenzyme in the complexes was not identified. 9,10 Ulcerative colitis is a type of inflammatory bowel disease (IBD) which affects the colon and rectum. 11 The main pathophysiological processes in ulcerative colitis are inflammation of the mucosa and ulceration of the lumen of the intestine. The most common symptom of the disease is diarrhoea with the passing of blood in the stool, which is also common in other diseases, such as bowel cancer. The severity of the condition depends on the amount of inflammation present, and complications can include steatohepatitis, anaemia and blood loss due to haemorrhage. The prognosis for patients with ulcerative colitis has improved greatly in recent years due to developments in medical and surgical procedures, but 25–30% of sufferers will ultimately require a colectomy.
Case report
A 41-year-old male patient presented to his local general practitioner (GP) reporting a change in bowel habit over two months to a pattern of persistent and frequent diarrhoea. On examination, the patient's abdomen was soft and tender and his stools were visibly blood-stained and contained mucus. The patient had no significant past medical history, was a non-smoker and occasional drinker of alcohol.
A full blood count and a number of biochemical investigations were performed on the patient, including liver and renal function tests, as well as assessment of his calcium homeostasis. The only abnormality found was a raised serum ALP activity of 267 U/L (reference range: 42–128 U/L) when measured by a spectrophotometric para-nitrophenyl phosphate assay on an Abbott Architect analyser (Abbott Laboratories, Abbott Park, IL, USA). The ALP activity was still elevated when a repeat measurement was carried out one month later (231 U/L). The patient's GP subsequently contacted our laboratory and asked us to investigate the cause of his raised ALP activity.
In order to determine the isoform of ALP causing the raised activity, ALP isoenzyme electrophoresis was performed on the patient's serum sample using a Sebia Hydragel 15 ISO PAL kit (Sebia, Issy-les-Moulineaux, France). Following electrophoresis, the major band present was a slow migrating form of ALP (Figure 2, lanes 1 and 2), as well as a smaller band of bone ALP in the lane containing lectin (Figure 2, lane 2). Lectin is present to bind to bone ALP and thus separate it from the placental and liver ALP isoenzymes. There was also a very faint band with a migration pattern consistent with liver ALP (lane 2). The major band did not fit the migration pattern of any of the isoforms of ALP shown in the product manual (Figure 1).
Separation of the patient's serum sample using the Sebia Hydragel 15 ISO PAL kit. Lanes 1 and 2 contain the patient's serum sample; lanes 3 and 4 contain the supernatant produced following a PEG precipitation of the sample. PEG, polyethylene glycol precipitation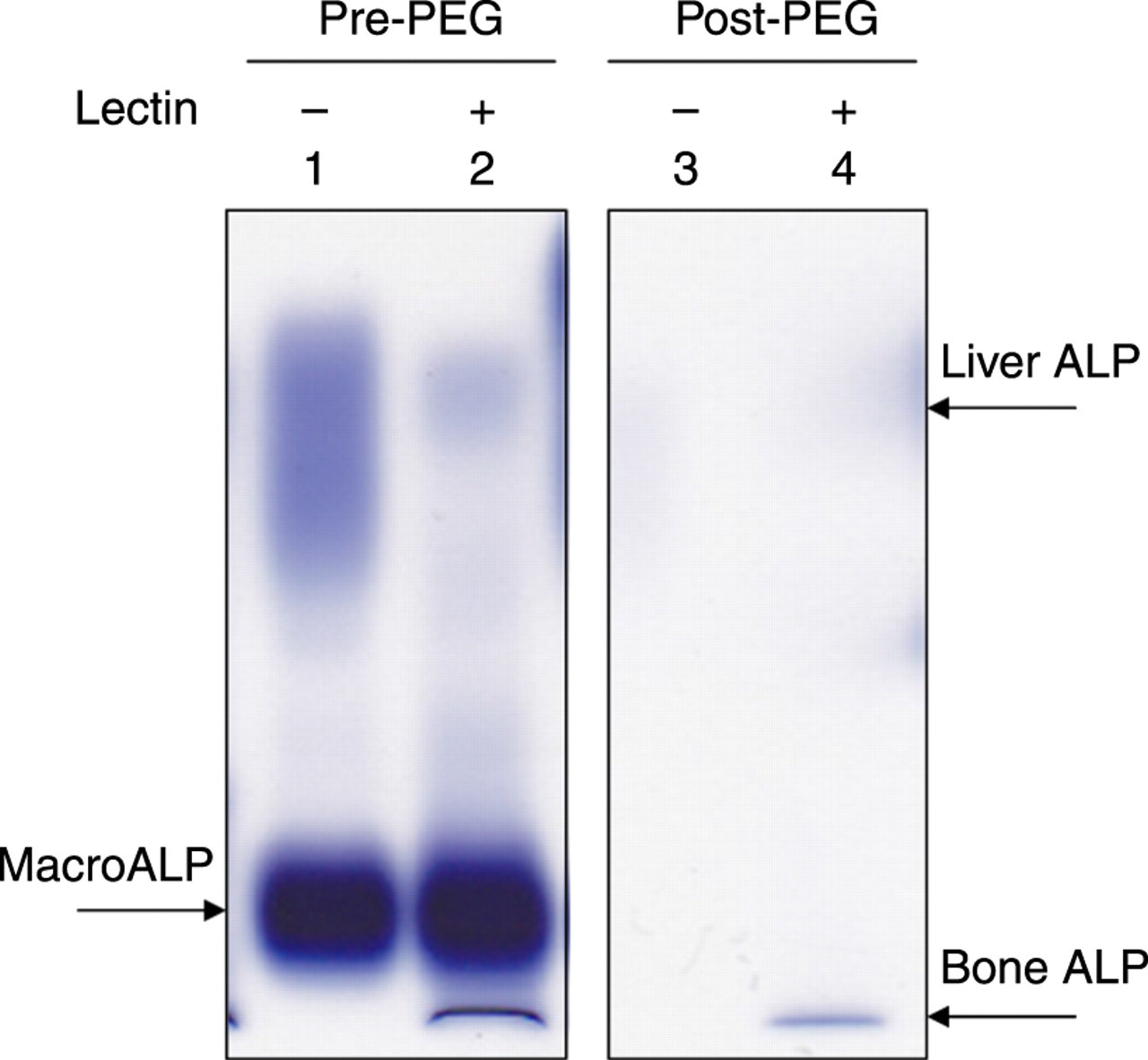
Following discussion with the manufacturer, it was suggested that the major band may be immunoglobulin-bound ALP (macroALP). In order to determine if this was the case, a polyethylene glycol precipitation (PEG) technique, which precipitates immune complexes, was carried out on the patient's serum sample. This technique has previously been shown to be effective for detecting macroenzymes. 12 The sample was mixed with an equal volume of PEG (molecular weight: 6487) solution (250 g/L). This mixture was then centrifuged for 10 min at 3000 rpm, following which the supernatant was decanted and its ALP activity measured using the Abbott Architect ALP assay.
The percentage of PEG-precipitable activity was 75.3%, which is consistent with the presence of macroALP. 12 Furthermore, the slow-migrating ALP was no longer visible following electrophoresis (Figure 2, lanes 3 and 4), suggesting the band was indeed macroALP. The bands of liver and bone ALP were decreased to some extent following the PEG precipitation (Figure 2, lane 4), indicating there was a slight overall decrease in ALP activity due to PEG. However, the major slow-migrating band was completely abrogated, strongly suggesting that macroALP was the cause of the patient's raised serum ALP activity.
In order to rule out coeliac disease as the cause of the patient's persistent diahorrea, IgA and IgG tissue translglutaminase (TTG) antibodies were measured in the patient's serum sample. A fluorometric enzyme-linked immunoassay on an ImmunoCap® 250 analyser (Phadia US Inc, Portage, MI, USA) was used, but neither IgA nor IgG TTG antibodies were detected, suggesting that the patient did not have coeliac disease.
Due to the severity of the patient's symptoms, he was referred to the gastroenterology department. A rectal examination was carried out which revealed the presence of blood-stained mucus; rigid sigmoidoscopy showed the patient's mucosa was red and very inflamed. A rectal biopsy was subsequently performed and histological analysis showed severe active chronic proctitis, which is consistent with ulcerative colitis. This preliminary diagnosis of ulcerative colitis was confirmed by colonoscopy. The patient was given a bowel-specific anti-inflammatory drug, mesalazine, to treat his ulcerative colitis; his symptoms have improved and his ALP activity had decreased slightly to 175 U/L when measured three months later.
Discussion
We have shown that the Sebia Hydragel 15 ISO PAL kit used in combination with PEG precipitation can be effectively used to identify cases of macroALP. The presence of macroALP is rare and thought to be benign. The discovery of macroALP was important in this case as it showed that the raised ALP was not due to malignancy. If immunoglobulin-bound ALP had not been identified as the cause of the raised ALP activity, a number of invasive and potentially harmful investigations may have been performed.
Since this is not the first report of macroALP in a patient with ulcerative colitis, the presence of macroALP may be more common in patients with the condition than in the general population. A potential study would be to screen a cohort of patients with ulcerative colitis for the presence of macroALP, to establish if there is an increased prevalence of the macroenzyme in patients with this type of IBD. If this is the case, monitoring ALP activity overtime in individual patients and determining if it correlates with disease progression would be the next point of interest.
DECLARATIONS