
Abstract
Background
Measurement of serum natriuretic peptides is recommended in patients with suspected heart failure. Assays for N-terminal pro-B-type natriuretic peptide (NT-proBNP) are available on several platforms and can be measured in serum or heparinized plasma. Siemens Healthcare Diagnostics do not recommend the use of serum for the Immulite NT-proBNP assay. Serum offers some practical advantages over plasma. We investigated the suitability of serum for use with the Immulite and Dimension Vista LOCI methods.
Methods
Paired serum and heparinized plasma samples were drawn from patients in the Cardiology Department over a 48-h period. Samples spanning the NT-proBNP concentration range 50–60,000 ng/L were analysed using the Siemens Immulite 2500 and Dimension Vista LOCI methods.
Results
There was no significant difference between serum NT-proBNP concentrations on either platform (P = 0.0665). Plasma NT-proBNP measured using the Immulite were moderately higher than on Vista (P < 0.0001). There was a small but statistically significant difference between plasma and serum NT-proBNP measured using the Immulite (P = 0.0002) with plasma values higher than serum. A similar comparison between plasma and serum NT-proBNP measured using the Vista showed no difference (P = 0.3662).
Conclusions
We have demonstrated the suitability of serum for use on the Immulite 2500. Bland–Altman comparative analysis indicated minimal bias between both serum methods near the clinical cut-off level below which heart failure is considered unlikely (400 ng/L) up to the highest concentration tested (60,000 ng/L).
Introduction
Measurement of serum natriuretic peptides is recommended in patients with suspected heart failure. 1 Human B-type natriuretic peptide (BNP) is produced by cardiac myocytes in response to increased ventricular wall tension and volume expansion. It is released as the 108-amino acid precursor pro-BNP. Pro-BNP undergoes proteolytic cleavage to release a 32-amino acid physiologically active hormone, BNP, and the inactive N-terminal 76-amino acid peptide, NT-proBNP. 2 NT-proBNP has several practical advantages over BNP as a biochemical marker, demonstrating a longer half-life, increased in vitro stability, reduced intra-individual variation and higher circulating concentration. 3–5
Several commercial assays are available for NT-proBNP. All assays use the synthetic human NT-proBNP1–76 calibration standard, explaining the small (<20%) difference in values generated by the different assays. Siemens Healthcare Diagnostics market methods on both the Immulite and Dimension Vista platforms. The Immulite assay uses a sheep polyclonal capture antibody directed against the N-terminal 1–21 sequence and a sheep polyclonal detection antibody against the central 39–50 sequence of NT-proBNP. The Dimension Vista LOCI assay utilizes monoclonal capture and detection antibodies directed against the N-terminus (residues 22–28) and central regions (residues 42–46), respectively. 6
On several analytical platforms, NT-proBNP can be measured in either serum or heparinized plasma; both produce similar results. There is little practical advantage in using one sample type over another. Siemens Healthcare Diagnostics do not consider serum as being suitable for use with the Immulite assay. 7 Serum offers a practical advantage over plasma, as a single blood sample would be required for NT-proBNP analysis and routine biochemistry tests. Natriuretic peptide measurement in suspected heart failure has great promise in the primary health-care arena. In some primary health-care settings, where the majority of requests for NT-proBNP originate, it can be difficult to source alternative types of sample tubes for chemistry analysis and serum is the sample of choice for most investigations. Therefore, we investigated the suitability of serum as the sample type on two different analytical platforms: the Immulite and the Dimension Vista.
Methods
Paired serum and heparinized plasma samples for NT-proBNP analysis were drawn from patients (n = 52) in the Cardiology Department, Aberdeen Royal Infirmary, over a 48-h period. Approximately 3–5 mL blood was drawn per patient into a serum separator tube (BD Vacutainer SST II Advance gel tube) and a plasma separator tube (BD Vacutainer LH PST II gel tube) (Becton Dickinson, Franklin Lakes, NJ, USA). Both sample types were analysed for NT-proBNP (median time from venepuncture = approximately 6 h) using the Siemens Immulite 2500 and Dimension Vista LOCI methods (Siemens Healthcare Diagnostics, Tarrytown, NY, USA). Samples spanning the NT-proBNP concentration range 50–60,000 ng/L were included for the comparison study. This included samples near the NT-proBNP clinical cut-off of 400 ng/L. An NT-proBNP concentration below this value in any patient of any age makes the diagnosis of heart failure unlikely. 1 This cut-off is universal across all methods for NT-proBNP due to <15% total imprecision between all assays at concentrations around the cut-off level. 8 All data were processed using Graphpad Prism 5 (GraphPad Software, La Jolla, CA, USA). All data followed a Gaussian distribution following log transformation and Shapiro–Wilk normality testing. Transformed data were analysed by paired Student's t-test. Untransformed data were analysed using Deming linear regression and Bland–Altman comparison.
Results
There was no significant difference between log serum NT-proBNP concentrations measured on either platform by paired t-test (P = 0.0665). Deming regression analysis on untransformed data showed a slight positive bias of Immulite values compared with Vista; regression equation: Immulite = 1.056 Vista + 66.64 (95% confidence interval [CI] for slope = 1.040–1.072 and intercept = −119.3 to 252.6). Bland–Altman analysis of non-transformed data comparing serum NT-proBNP over the concentration range 0–4000 ng/L is shown in Figure 1a. Mean bias was calculated at 3.67% ± 14.1 with Immulite NT-proBNP concentrations higher than in Vista. There was no evidence of misclassification of patients with heart failure based on NT-proBNP measurement using one platform over the other.
Bland–Altman plots for comparison between N-terminal pro-B-type natriuretic peptide (NT-proBNP) measured using the Dimension Vista LOCI and Immulite 2500 methods. Mean NT-proBNP concentrations for (a) paired serum (SST) and (b) paired plasma (PST) measured on both platforms are plotted on the x-axis and the differences (Immulite–Vista) are plotted on the y-axis. Solid and dashed lines represent mean ± 2 standard deviations respectively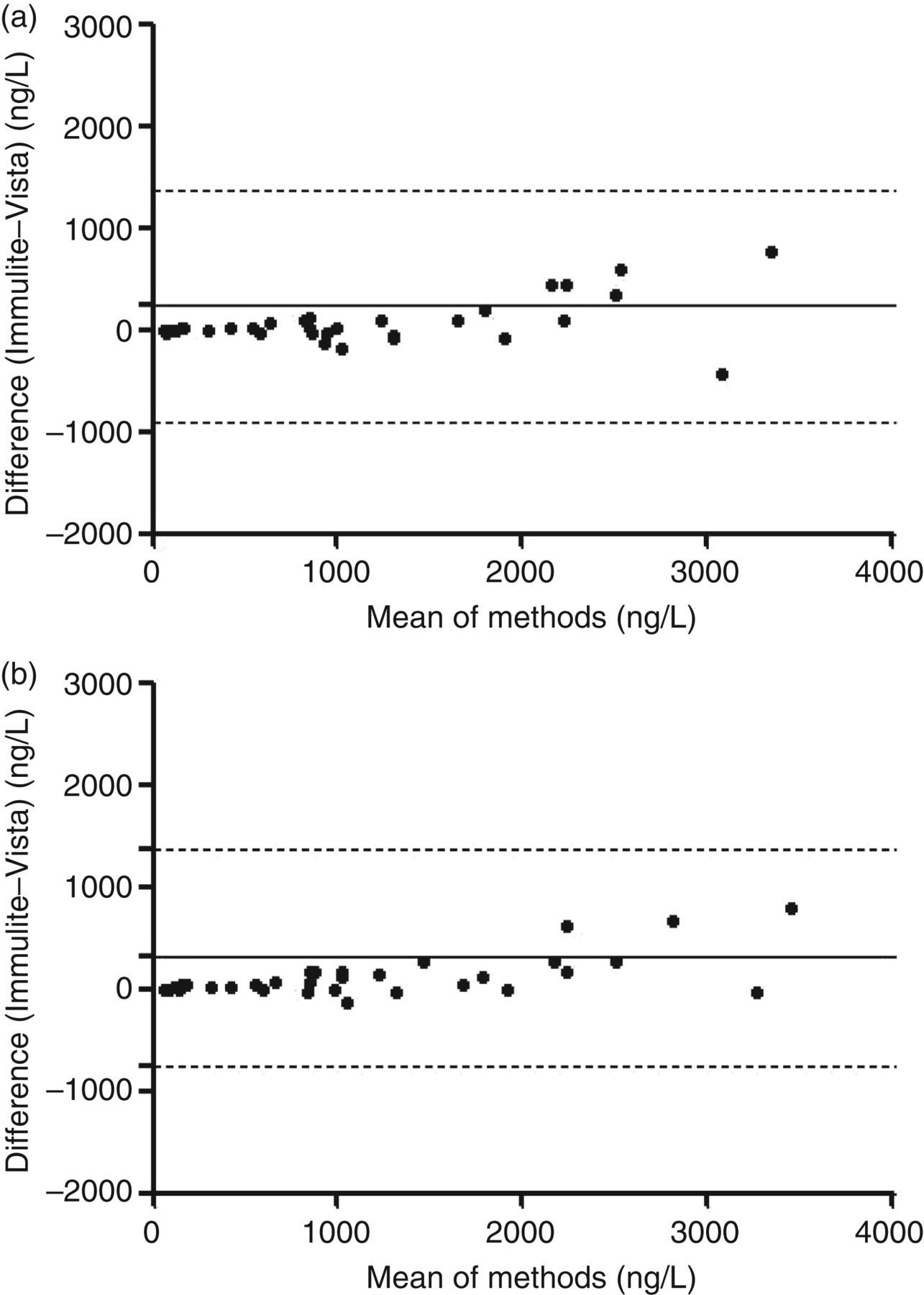
Plasma NT-proBNP samples measured using the Vista were statistically different from those measured on the Immulite (P < 0.0001). Bland–Altman analysis of non-transformed data comparing plasma NT-proBNP concentrations over the range 0–4000 ng/L is shown in Figure 1b. In a similar trend to that observed in serum, mean bias was calculated at 8.9% ± 12.0 with Immulite NT-proBNP concentrations higher than Vista (Deming regression equation: Immulite = 1.015 Vista + 231.0 [95% CI for slope = 0.9906 to 1.040 and intercept = −62.78 to 542.8]).
It was also evident from Figure 1 that there was increasing bias in both serum and plasma towards higher Immulite values with increasing NT-proBNP concentration. In serum, Immulite values were greater at NT-proBNP concentration > 2000 ng/L (mean bias = 8.31% ± 9.98%) compared with NT-proBNP < 2000 ng/L (mean bias = 1.92% ± 11.0%). However, this trend was also seen in plasma with Immulite values higher at concentrations > 2000 ng/L (11.49% ± 15.53) than at concentrations < 2000 ng/L (mean bias; 6.66% ± 10.21%).
Serum and plasma NT-proBNP concentrations were directly compared on each analytical platform. There was a small but statistically significant difference between plasma and serum NT-proBNP measured on the Immulite (P = 0.0002). Bland–Altman analysis (Figure 2a) across the NT-proBNP concentration range 0–4000 ng/L showed higher plasma values to those in serum (calculated mean bias 7.3% ± 9.1; Deming regression equation: plasma = 1.026 serum + 22.89; 95% CI for slope = 0.9902 to 1.061 and intercept = −29.79 to 73.57). A similar comparison between plasma and serum NT-proBNP measured using the Vista (Figure 2b) showed no statistically significant difference between the two sample types (P = 0.3662). The median plasma NT-proBNP concentration was slightly higher than that of serum with Vista (calculated mean bias 0.17% ± 2.5; Deming regression equation: plasma = 1.010 serum–4.822; 95% CI for slope = 0.9924 to 1.027 and intercept = −30.86 to 21.22).
Bland–Altman plots for comparison of N-terminal pro-B-type natriuretic peptide (NT-proBNP) in serum and plasma using the Immulite 2500 and Dimension Vista platforms. Mean NT-proBNP concentrations for (a) Immulite 2500 and (b) Dimension Vista are plotted on the x-axis and the differences (plasma–serum) are plotted on the y-axis. Solid and dashed lines represent mean ± 2 standard deviations respectively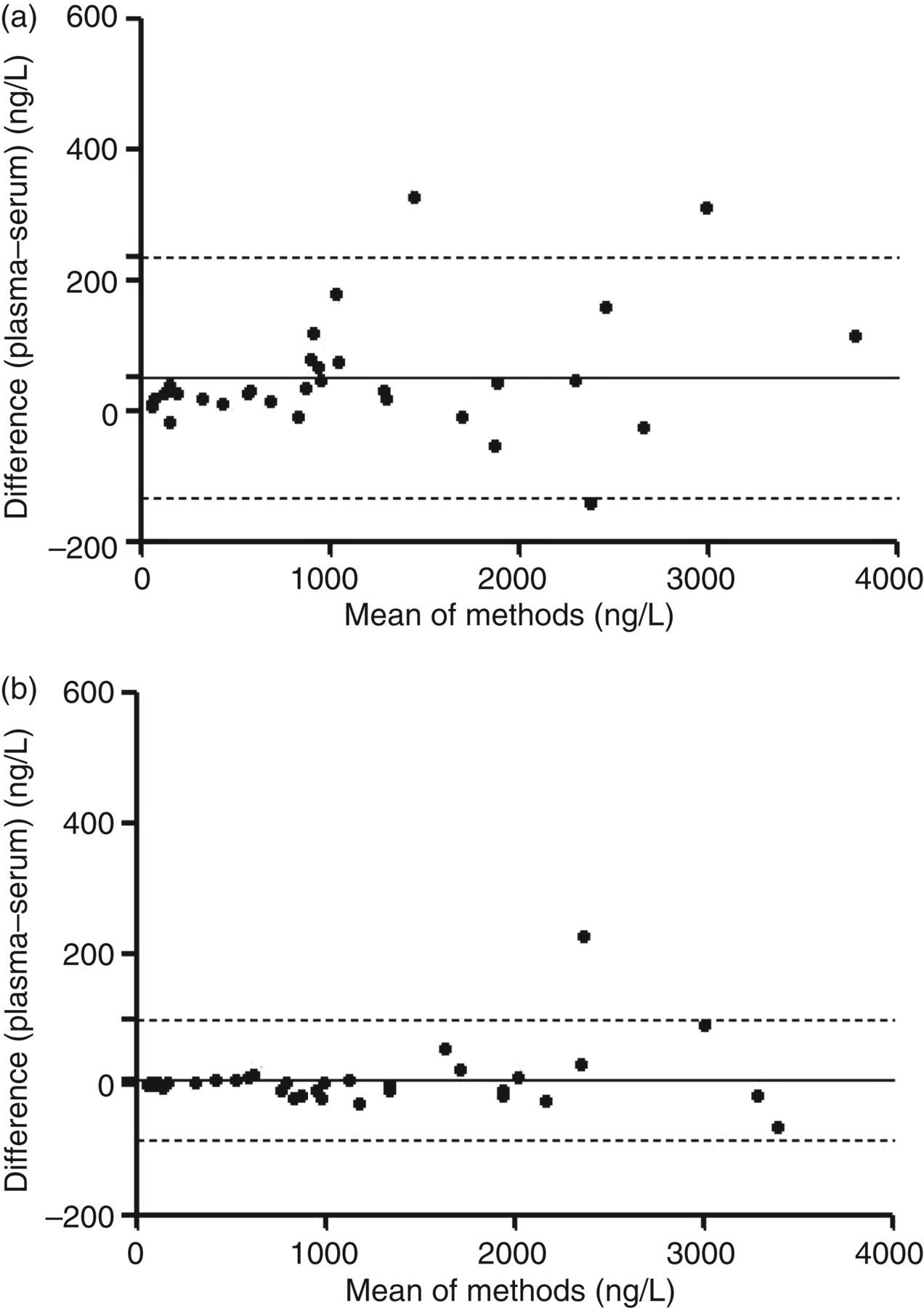
Discussion
This report demonstrates the suitability of serum as a sample matrix for use with the Immulite 2500 NT-proBNP method when compared with the validated serum method on the Dimension Vista. To the best of our knowledge, this observation has not been seen elsewhere. In a previous report by Al-Kindi et al., 9 the Immulite 2000 NT-proBNP method was compared with the Roche E170 method, with the Immulite being approximately 30% lower than the E170 at concentrations greater than 10,000 ng/L in serum. In agreement with these findings, Siemens Healthcare Diagnostics do not advocate the use of serum for use with the Immulite NT-proBNP assay. They have optimized the NT-proBNP assay on the Immulite for use with plasma only under the terms of the licensing agreement with Roche Diagnostics (Basel, Switzerland). In addition, Siemens Healthcare Diagnostics observed a non-parallel response between serum and heparinized plasma during the validation of the assay. In contrast, Deming regression analysis carried out on our data showed a linear relationship between the Immulite and Vista methods up to the highest NT-proBNP concentration tested (approximately 60,000 ng/L; data not shown). There was also little evidence of methodological bias at lower NT-proBNP concentrations near the optimal clinical cut-off level below which heart failure is considered unlikely (400 ng/L). Subsequently, there were no cases of potential misclassification around the clinical cut-off value of 400 ng/L based on analysis in plasma or serum on either platform.
We conclude from our study that serum is a suitable sample matrix for use compared with heparinized plasma on the Siemens Immulite 2500 NT-proBNP method. This is particularly relevant at NT-proBNP concentrations close to the diagnostic cut-off values.
DECLARATIONS