
Abstract
Background
Long-term follow-up studies after endovascular treatment for intracranial aneurysm are still rare and inconclusive. Parenchymal infarctions related to aneurysms have mostly been studied in patients with subarachnoidal hemorrhage (SAH) but infarction rates in patients with endovascularly treated unruptured aneurysms have been little studied.
Purpose
To determine the frequency of permanent parenchymal lesions as detected in magnetic resonance imaging (MRI) in patients treated with endovascular coiling and to assess aneurysm-related infarctions after the initial treatment period.
Material and Methods
A total of 64 patients (32 with primarily ruptured aneurysms) with 69 embolized aneurysms were examined neurologically and by MRI and magnetic resonance angiography (MRA) more than 9 years after the initial endovascular treatment.
Results
A total of 14 out of 32 (44%) SAH patients and 11 (34%) patients with unruptured aneurysms had parenchymal lesions in MRI. Infarctions were detected in 10 (31%) SAH patients and the majority (9/10, 90%) of them were aneurysm-related. All aneurysm-related infarctions were detected at the acute hospitalization stage. A total of six (55%) out of 11 infarctions in patients with unruptured aneurysms were aneurysm-related and two of them appeared after the treatment period. Patients with infarction had poorer clinical outcome than patients with no ischemic lesions in MRI.
Conclusion
Nineteen percent of patients with unruptured and 41% with ruptured aneurysms had aneurysm-related parenchymal lesions in MRI. Most of these were detected during acute treatment period. Aneurysm-related infarctions after treatment period are uncommon.
Morbidity after subarachnoid hemorrhage (SAH) is still high despite developed treatment methods, anesthesiological modalities, and intensive rehabilitation (1–7). Bleeding itself, vasospasm or treatment-related causes can cause cerebral lesions visible in computed tomography (CT) or magnetic resonance imaging (MRI). MRI is more sensitive for detecting parenchymal lesions than CT (8, 9). Infarction rate after aneurysmal SAH is as high as 79–89% in clipped patients (8, 10–12). Aneurysm treatment with endovascular coiling seems to be safer than clipping (10, 13) and fewer infarctions are seen in coiled patients (10, 12). Although lesions consistent with infarction seen in CT or MRI sometimes appear extensive, patients may in fact be asymptomatic (14, 15). The treatment of small unruptured aneurysms is much debated because the International Study of Unruptured Intracranial Aneurysms (ISUIA) showed that surgical morbidity and mortality from unruptured aneurysms was higher than risk of rupture for aneurysms less than 10 mm over a 7.5-year period (16). Morbidity related to endovascular coiling in unruptured aneurysms is between 1.7 and 8.6% (16–20) and lower than in patients receiving surgical treatment (16, 17, 21). The incidence of parental artery infarction after unruptured aneurysm coiling is not known. The aim of this study was to ascertain the frequency of permanent parenchymal lesions as detected in MRI in patients treated with endovascular coiling and to assess aneurysm-related infarctions after the initial treatment period.
Material and Methods
Patient population
A total of 185 patients with 200 aneurysms were treated between 1992 and 1999 with endovascular coiling in our hospital (Fig. 1). Twenty patients had one or more aneurysms clipped and were excluded from this study. A further 22 patients living outside our hospital catchment area were excluded because follow-up and possible re-treatment was not done in our hospital. Endovascular procedures were done in cases where the aneurysm seemed to be treatable in the estimation of the endovascular radiologist and neurosurgeon. Aneurysms were embolized with platinum Guglielmi detachable coils (GDC, Target Therapeutics, Fremont, CA, USA) and peri-interventional medication was 5000 IU unfractionated heparin intravenously before coiling in unruptured cases and 5000 IU unfractionated heparin intravenously after two coils in ruptured cases. Intravenous nimodipine was used routinely. The clinical status of patients with aneurysmal SAH was assessed at the time of onset and treatment according to the Hunt & Hess scale (H&H) (22). Glasgow Outcome Score (GOS) (23) was used to evaluate clinical status at the time of discharge and at follow-up visits.
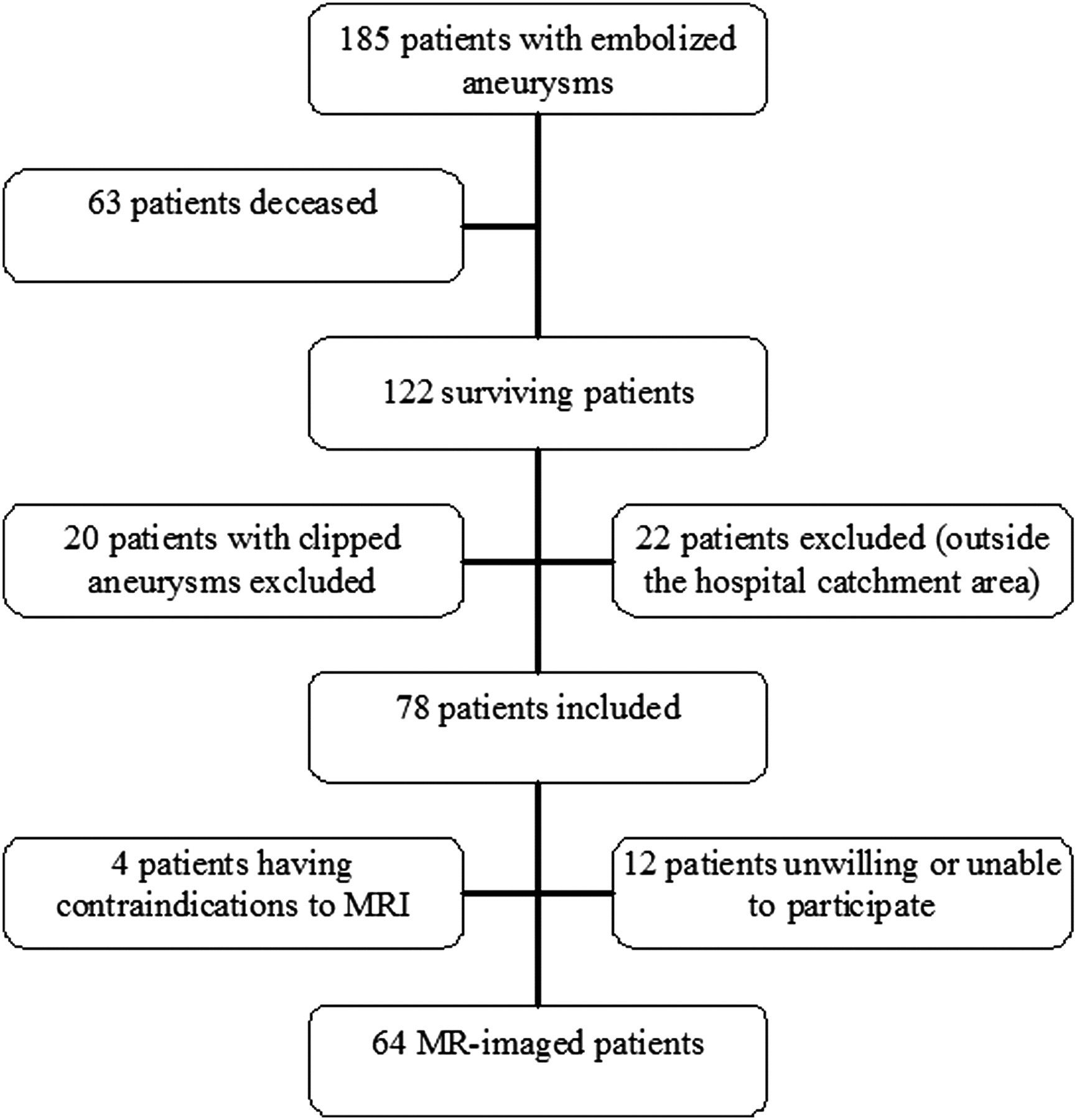
Flowchart summarizing the included and excluded patients
A total of 63 patients were deceased at the time of follow-up and 34 (54%) of them died due to aneurysmal disease (Table 1). Sixteen patients were lost from MRI follow-up either due to refusal to participate in follow-up studies or to having contraindications to magnetic field studies. Sixty-four patients harbouring 72 aneurysms were studied for more than 9 years after the initial coiling procedure (Table 2). Mean follow-up time was 11 years (range 9–16 years, median 10). Sixty-nine aneurysms were coiled and three were left untreated due to small size. Thromboembolic events occurred in seven coiling procedures (10%) and coil migration in one (1%) case. Neurological deterioration was detected in 15 procedures (22%) and infarction verified by CT was seen in 11 cases (16%). Three patients suffered re-bleeding in hospital before treatment and aneurysmal rupture occurred in two cases during coiling (3%). One patient (1%) re-bled 13 days after incompletely coiled aneurysm procedure. Re-treatment was provided for 23 aneurysms (33%) from one month to six years after the initial treatment (mean 15 months).
Cause of death of the 63 deceased patients
Population characteristics
ICA = internal carotid artery; MCA = middle cerebral artery; ACoA = anterior communicating artery; ACoP = posterior communicating artery; ACA = anterior cerebral artery; COPD = chronic obstructive pulmonary disease; SAH = subarachnoidal hemorrhage; GOS = Glasgow Outcome Scale
Data collection
All hospital records were studied retrospectively and all CT scans, MR images and angiograms performed from 1992 to 2008 were analyzed. Preoperative CTs were done for 32 SAH patients and 15 patients with unruptured aneurysms. Preoperative MRIs were done for two SAH patients and 21 patients with unruptured aneurysms. Postoperative CTs during the acute stage of the disease were done for 17 SAH patients and seven patients with unruptured aneurysms. Postoperative MRIs were done for four SAH patients during the initial treatment period. Surviving patients included were contacted by letter offering an MRI examination. A total of 64 patients were studied with MRI between the years 2007 and 2008 and patients were interviewed and examined neurologically by the author. The study was approved by the Hospital Ethics Committee and all patients gave their informed consent to the study.
Imaging protocol
The follow-up MR imaging was performed with 1.5 T unit (GE Signa HD, Milwaukee, WI, USA) with 1-channel head-coil. The MRA was supplemented with cross-sectional imaging including fluid attenuated inversion recovery (FLAIR) and T2* weighted sequences mainly to detect ischemic parenchyma, the size of the CSF spaces and signs of persistent blood degradation deposits. The imaging parameters for the non-contrast 3D time-of-flight angiography were: TR 30, TE 2.5, FOV 22 × 16.5 cm, slice thickness 1.0 mm/interpolated to 0.5 mm, matrix 320 × 224. Magnetization transfer contrast and flow compensation were included. The imaging parameters for the FLAIR were: TR 9001 ms, TE 125 ms, TI 2250 ms, FOV 22 cm, slice thickness 5/1 mm, matrix 224 × 256, NEX 1 and for T2* weighted images: TR 460 ms, TE 20 ms, flipangle 20°, FOV 22 cm, slice thickness 5/1 mm, matrix 160 × 256 (interpolated to 512), NEX 2. Areas of increased signal intensity of vascular territories in T2* weighted images were considered as infarctions. Small high signal foci on T2* weighted images were considered as leukoaraiosis.
Imaging assessment
The diagnostic, procedural and follow-up images were reviewed independently by a neuroradiologist, a neurointerventionalist and a neurosurgeon. Thereafter, the results were reviewed and a consensus statement for each study was issued. MRI and MRA studies done prior to this study were analyzed and compared with the present study results. Primary CT images were re-evaluated to assess Fisher grades, existence and grade of ventricular enlargement and possible parenchymal lesions. Parenchymal lesions were considered aneurysm-related if they appeared during acute hospitalization, aneurysmal ICH was seen in primary CT or detected in parental artery territory after treatment period. Infarctions in MRI were divided into parental and non-parental artery territory infarctions.
Statistical analysis
Statistical analysis was performed using NCSS statistical software (NCSS, Kaysville, UT, USA). Categorical variables were compared using Fisher's exact two-tailed test. Continuous variables between groups were compared using the Mann-Whitney U-test. The level of significance was set at p < 0.05.
Results
MRI findings at long-term follow-up
Parenchymal lesions
Ten years after embolization, 18 (56%) SAH patients and 21 (66%) patients with unruptured aneurysms showed normal brain MRI. Parenchymal lesions on FLAIR images of different cause (infarctions or previous ICH) were seen in 14 (44%) SAH patients (Fig. 2) and 11 (34%) patients with unruptured aneurysms (Fig. 3).
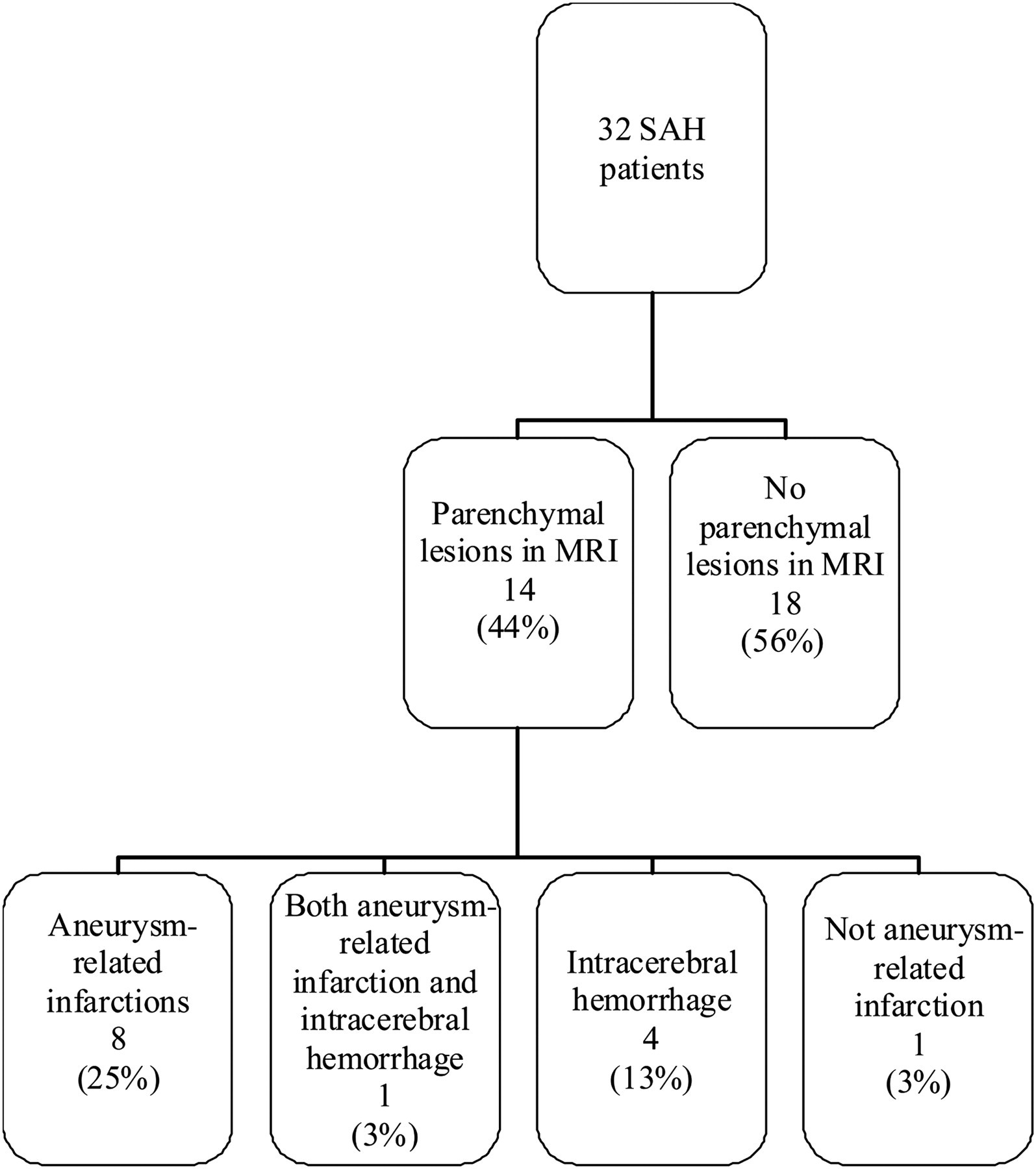
Flowchart summarizing parenchymal lesions in SAH group

Flowchart summarizing parenchymal lesions in patients with unruptured aneurysms
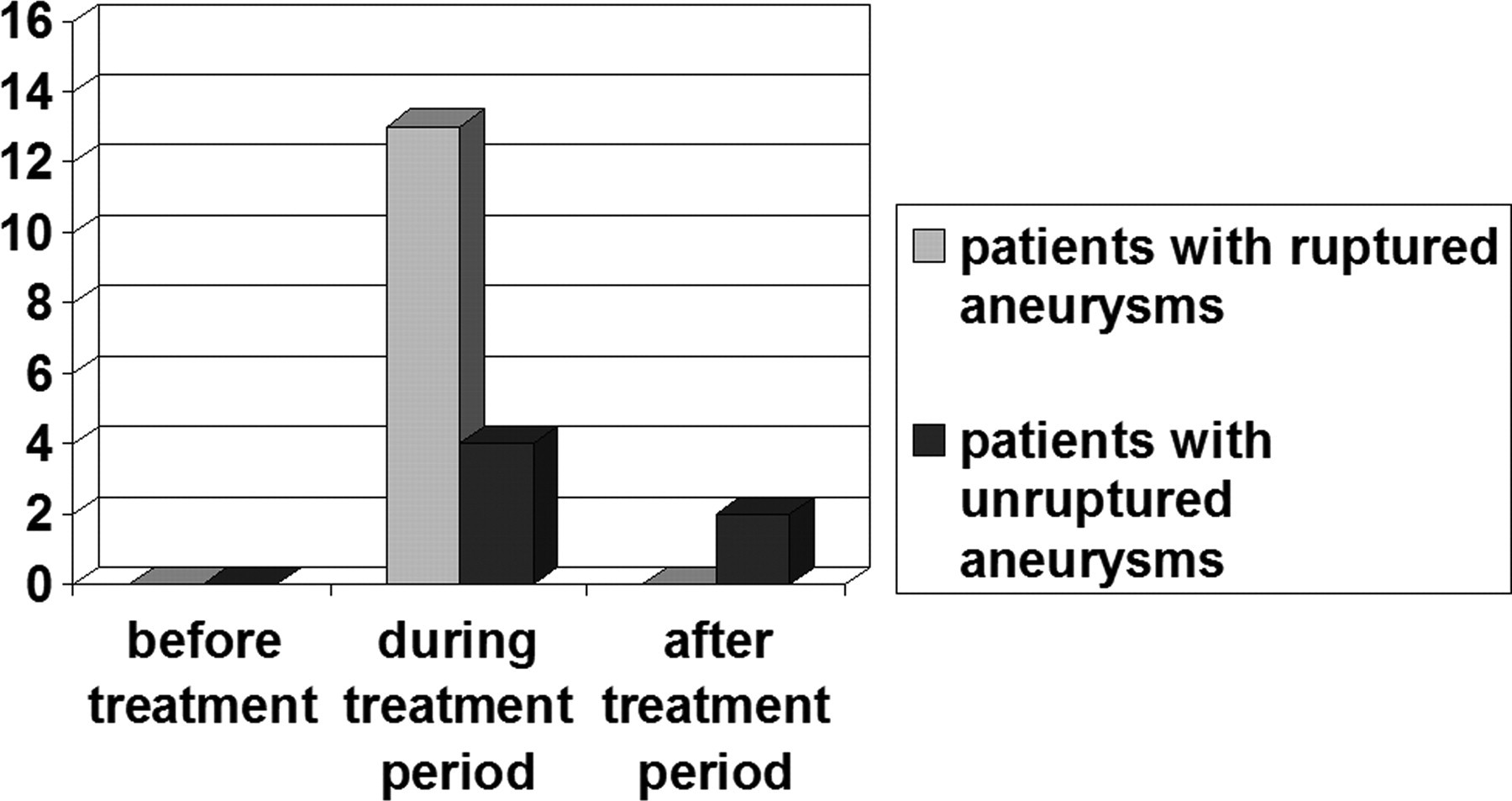
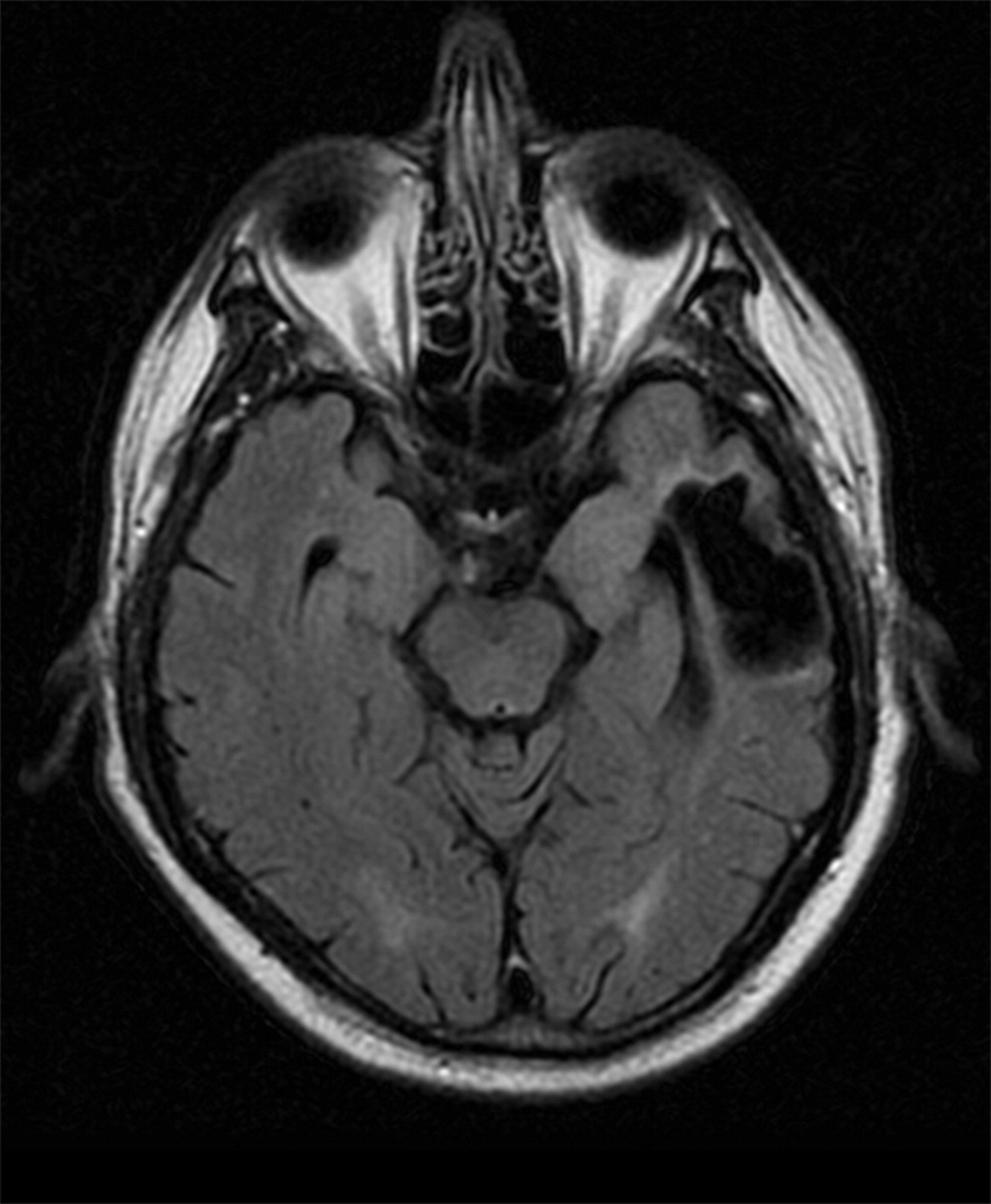
Infarctions in the parental artery territory
Lesions on FLAIR images indicating infarction in the vascular territory of the aneurysm were seen in six (19%) SAH patients and six (19%) patients with unruptured aneurysms (Fig. 4). All but two of these lesions were detected during the treatment period (Fig. 5). Infarctions were detected in patients who had either thromboembolic complications or clinical or angiographic vasospasm and infarctions in CT images. Two patients had infarctions in parental artery territory that were not detected during acute hospitalization. One of these patients had a small infarction in middle cerebral artery aneurysm territory without any clinical defects after coil migration in primary treatment procedure. The other patient had two infarctions at separate locations which occurred 10 years after primary stenting and coiling and 3 years after re-embolization of a giant ICA aneurysm.
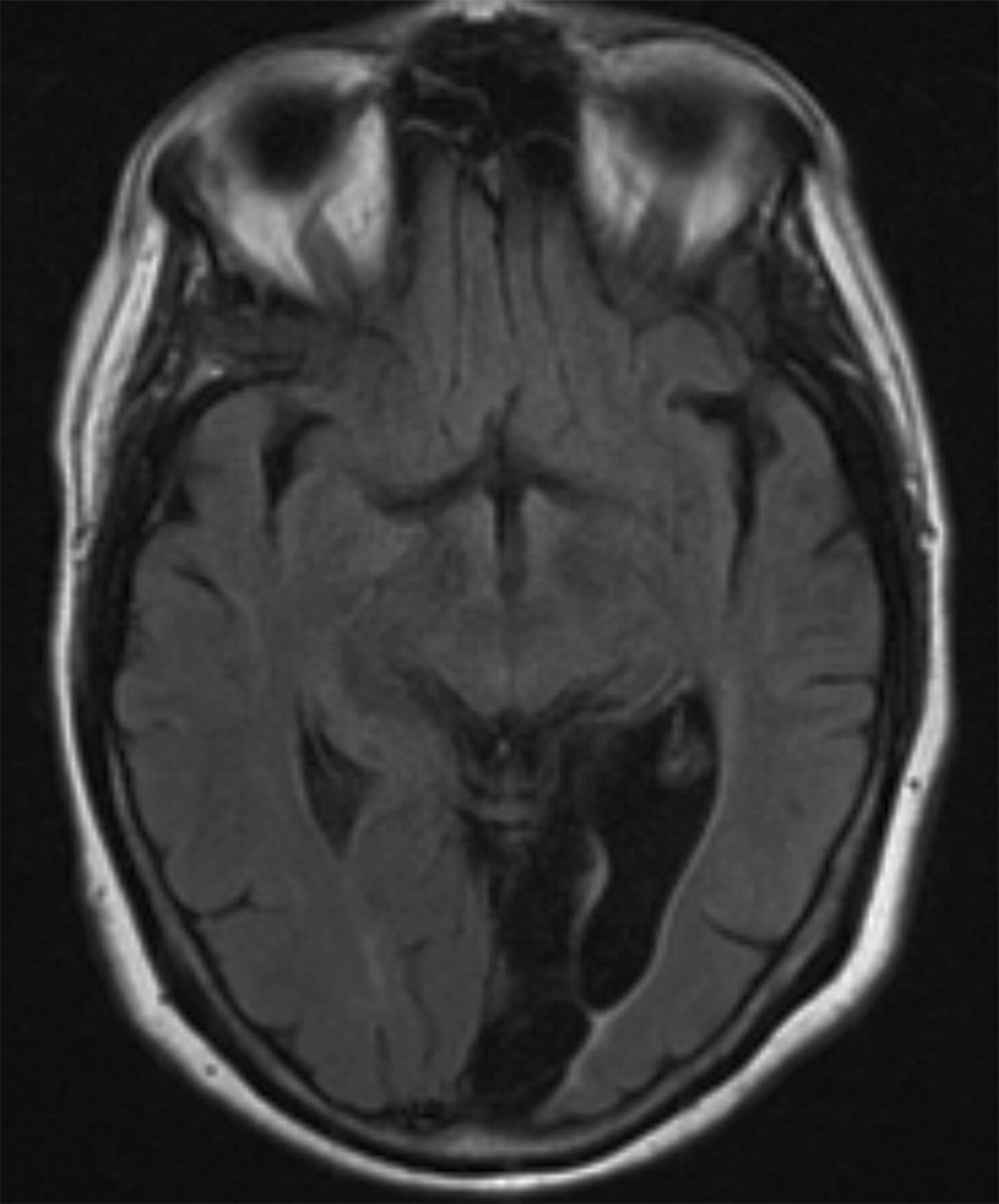
Fluid-attenuated inversion recovery image shows large infarction in the left posterior cerebral artery territory caused by thromboembolic complication in coiling procedure
Aneurysm-related infarction rates
Infarctions in other vascular territories
Brain infarctions in vascular territories other than that of the ruptured aneurysm were seen in four (13%) SAH patients and three (9%) of them were considered to be caused by vasospasm. Six (19%) patients with unruptured aneurysms had infarctions in non-parental artery territory. In four (13%) of these the infarctions were detected by CT before aneurysm treatment and in two patients years after the coiling. None of them were considered to be aneurysm-related.
Residual signs of hematoma and superficial siderosis
Signal intensity changes seen on FLAIR images due to previous ICH were detected in five (16%) SAH patients (Fig. 6). Signs of superficial siderosis were present in six (19%) SAH patients.
Fluid-attenuated inversion recovery image shows retractive lesion in the left temporal lobe caused by intraparenchymal haemorrhage from a ruptured medial cerebral artery aneurysm
Ventricular enlargement and leukoaraiosis
Five patients (8%) had ventricular enlargement. Leukoaraiosis was seen in 25 (39%) patients: in 16 (50%) patients with ruptured aneurysms and in nine (28%) patients with unruptured aneurysms.
Clinical outcome
Most patients were in good clinical condition after follow-up: 41 (64%) patients had a GOS score of 5 and 18 (28%) patients had a GOS score of 4. Only five patients (8%) were dependent (GOS score of 3). GOS tended to be lower in patients with unruptured aneurysms than in patients with ruptured aneurysms but the difference was not statistically significant (p > 0.08). Poor outcome in patients with unruptured aneurysms was related to aneurysm in one patient only who had brainstem compression caused by a large basilar aneurysm. In others the reason for poor outcome was not related to aneurysms. Patients with unruptured aneurysms had more depression but less hypertension than patients with previous SAH (Table 2). Other diseases and medication were comparable between patients with ruptured and unruptured aneurysms.
Patients with infarction had poorer clinical outcome than patients with no ischemic lesions in MRI (p < 0.05, Table 3). Five out of 14 (36%) SAH patients with radiological infarction were asymptomatic. Four patients (29%) had global deficits and five patients (36%) had focal deficits. Patients with unruptured aneurysms and parenchymal lesions in follow-up MRI were mostly (70%) asymptomatic. Only three out of 11 patients (30%) had focal deficits.
Correlation between infarction prevalence and clinical outcome
GOS = Glasgow Outcome Scale
Discussion
Our aim was to determine the frequency of permanent parenchymal lesions in patients treated with endovascular coiling and to assess aneurysm-related infarctions after the initial treatment period. Thirty-four percent of patients with unruptured aneurysms had infarctions in MRI and 19% were aneurysm-related. Patients with unruptured aneurysms had high incidence of parenchymal lesions not related to aneurysm because most aneurysms were found incidentally during cerebral imaging for some neurological symptoms other than SAH. Forty-four percent of SAH patients had parenchymal lesions in follow-up MRI and most of these were aneurysm-related. Aneurysm-related infarctions were detected in 25% of SAH patients and all were detected during acute treatment period. Only two patients with unruptured aneurysms had aneurysm-related infarctions after the treatment period.
Because of the voluntary nature of the imaging study, we were only able to study 82% of included patients with follow-up MRI. Those we could not reach may be in poorer clinical condition and unable or unwilling to participate. It is thus likely that there is selection bias in our study and SAH patients may have a higher prevalence of parenchymal lesions than our 44%. Earlier reports have documented infarction rates of 57% (10, 11).
In follow-up images it is difficult to assess the cause of infarction and for this reason we classified lesions as parental artery territory or non-parental artery related. Taking into account only infarctions in parental artery territory, our figure of 19% compares favourably with earlier studies reporting parental artery territory infarction rates of 20% to 22% (10, 12). A total of 16% of patients had lesions caused by ICH, which is slightly lower than in the series of Koivisto and co-workers (12), who reported a rate of 25%. Lesions caused by ICH were detected in 22% in the series of Bendel (10). Unfortunately, in some studies patients with ICH were excluded. Incidence of infarctions not related to aneurysm territory in SAH patients was similar to that reported in earlier studies (10, 12).
To the best of our knowledge, there are no studies on infarctions long after embolized unruptured aneurysms. Patients with unruptured aneurysms had parental artery territory infarctions during the treatment period in 12% of cases, which compares favorably with earlier studies (20, 24). Late parental artery territory infarctions were uncommon although occlusion grade was incomplete in 36% of cases.
Small, high signal foci in the white matter are common incidental findings in T2-weighted images. As many as 79% of neurologically healthy people over 55 years have leukoaraiosis in MRI (25). In earlier reports, the frequency of leukoaraiosis in SAH patients was between 32–60% (8, 10, 11). In our study leukoaraiosis was present in 50% of SAH patients and 28% of patients with unruptured aneurysms. The clinical relevance of these small incidental findings remains unclear.
Clinical symptoms of ischemia were detected during the treatment period in all SAH patients who developed a parental artery territory infarction. Two out of six patients with unruptured aneurysms did not have any symptoms of ischemic episode during the treatment period and infarcts after the treatment period were related to coil migration, stenting procedure or giant aneurysm. Despite infarctions in unruptured patients, treatment of unruptured aneurysms did not cause permanent deterioration in outcome.
Bryan et al. reported that fewer than half of patients with cerebral lesion caused by SAH or its treatment have symptoms of stroke (26). We found higher symptom rates for SAH patients, of whom five out of 14 (36%) were asymptomatic. Four patients (29%) had global deficits and five patients (36%) had focal deficits. Patients with unruptured aneurysms were more often asymptomatic than SAH patients. Global deficits were not associated with unruptured aneurysms. Seventy per cent of patients with unruptured aneurysms were asymptomatic and 30% had focal deficits. Although SAH patients had more symptoms of cerebral infarctions, GOS was not lower than in the group with unruptured aneurysms. Actually, patients with unruptured aneurysms had poorer outcome but the difference was not statistically significant. The reason for this poorer outcome may be that depression was more common in the group with unruptured aneurysms. It is important to note that sample sizes in both groups were small and cannot be generalized in a straightforward manner to all aneurysm patients. Our outcome measure, GOS, may be too crude to measure outcome as reported in earlier studies (11, 27). In addition to primary analyses with GOS, we did some secondary analyses with the Extended Glasgow Outcome Scale (GOSE) (28). However the results were similar and patients with unruptured aneurysms had lower GOSE than SAH patients. In addition to small sample sizes there are other limitations in our study. Patient population is selected and infarction rates might thus be too low. MRIs in the acute hospitalization period were not done for every patient. Patients with ruptured and unruptured aneurysms had differences in population characteristics and cannot be compared in a straightforward manner.
This was a retrospective series and embolization technique has subsequently developed a lot. The aneurysms in our series were treated before the advent of newer techniques such as balloon-assisted remodeling or 3-dimensional GDC. These new techniques improve occlusion grades and probably also decreases complication rates.
In conclusion, 19% of patients with unruptured and 41% with ruptured aneurysms had aneurysm-related parenchymal lesions in MRI. Most of these were detected during acute treatment period. Aneurysm-related infarctions after treatment period are uncommon.
Footnotes
ACKNOWLEDGEMENT
This study was financially supported by EVO-funding of Pirkanmaa Hospital District and Maire Taponen Foundation