
Abstract
Background
Anastomotic leaks are uncommon complications following aortic surgery. To avoid the morbidity associated with a second surgical procedure, minimally invasive techniques have become increasingly popular.
Purpose
To evaluate the feasibility and safety of thrombin in interventional treatment of postoperative pseudoaneurysms.
Material and Methods
CT-guided percutaneous injection was chosen in four cases. Endovascular access using an occlusion balloon catheter placed in the orifice of the pseudoaneurysm was utilized in one case.
Results
The average volume of all pseudoaneurysms was 178 ± 190 mL with a volume of the patent lumen of 25 ± 28 mL. All aneurysms thrombosed after injection of 600 ± 237 IU of thrombin. During the follow-up period of an average of 10 months all pseudoaneurysms remained occluded.
Conclusion
Our series demonstrates the feasibility of thrombin in the treatment of aortic anastomotic pseudoaneurysms. In combination with occlusion balloon catheters, even wide-necked pseudoaneurysms may be treated successfully. However, further investigations are warranted.
Unlike the well-known, long-term developments after open abdominal aortic aneurysm (AAA) repair such as graft dilatation and aneurysms proximal and distal to the graft (1, 2), early postoperative pseudoaneurysms are relatively uncommon (3). In order to avoid the morbidity associated with a second surgical procedure, minimally invasive techniques have become increasingly popular. Recently, thrombin has been successfully used for the treatment of postcatheterization extremity pseudoaneurysms and pseudoaneurysms of the torso, respectively (4–6). We report our experiences in application of thrombin for the treatment of postoperative, peri-anastomotic, aortic pseudoaneurysms following open aortic surgery via percutaneous and endovascular approaches.
Material and Methods
Between December 2006 and December 2008 five patients (m:f = 3:2; mean age 65.4 years; range 51–74 years) following open aortic surgery were treated with an injection of thrombin (Tissucol Duo [500 IU Thrombin/mL]), Baxter International Inc., Deerfield, IL, USA). Individual written informed consent was obtained. Each procedure was an attempt to treat in concordance with the regulations of the local Institutional Review Board.
Enlargement of the pseudoaneurysms was demonstrated by repeated helical CT 8.4±1.6 days following implantation of an aortic prosthetic graft without patch plastic. Decision for treatment was made in conjunction with the vascular surgeon, following exclusion of ongoing infection by serum chemistry. Patient demographic data and pseudoaneurysm parameters are shown in Table 1. Measurements of size and volume of the aneurysms were performed using standard software on the basis of contrast-enhanced helical CT (Emotion 6, Siemens Medical Solutions, Erlangen, Germany).
Patient demographic data and pseudoaneurysm parameters
Slow thrombin injection (500 IU/min) was performed percutaneously through a 19.5 gauge needle (Uni-dwell; Angiomed, Karlsruhe, Germany) using CT guidance in four patients in whom CT demonstrated a small (<2 mm) necked pseudoaneurysm (Fig. 1). In one pseudoaneurysm with a neck measuring 11 mm, thrombin injection was performed via an endovascular approach utilizing an 8 French sheath (Super Arrow-Flex [F-8, 45 cm], Arrow International Inc, Reading, PA, USA) and an occlusion balloon catheter (occlusion balloon catheter 11.5, Boston Scientific, Cork, Ireland) inflated within the orifice of the pseudoaneurysm (Fig. 2). A microcatheter (Fast tracker F2.8, Boston Scientific, Cork, Ireland) was placed coaxially in the dome of the aneurysm and thrombin was slowly injected. Progress of the treatment was controlled either by repeated contrast enhanced CT angiography (Collimation: 6*2 mm; Pitch: 1.5; 60 mL Iomeprol [Imeron 300; Nycomed, Konstanz,Germany]; 3 mL/sec), or via the introducer sheath in case of endoluminal access. Control angiography was performed after injection of 150–250 UI thrombin.

Contrast enhanced helical CT. Following thoraco-abdominal aortic surgery, a giant pseudoaneurysm with a small perfused lumen was present; (a) additionally, a large hematoma was seen behind the left kidney; (b) using a percutaneous access, 300 IU thrombin were injected slowly, leading to a complete occlusion of the pseudoaneurysm
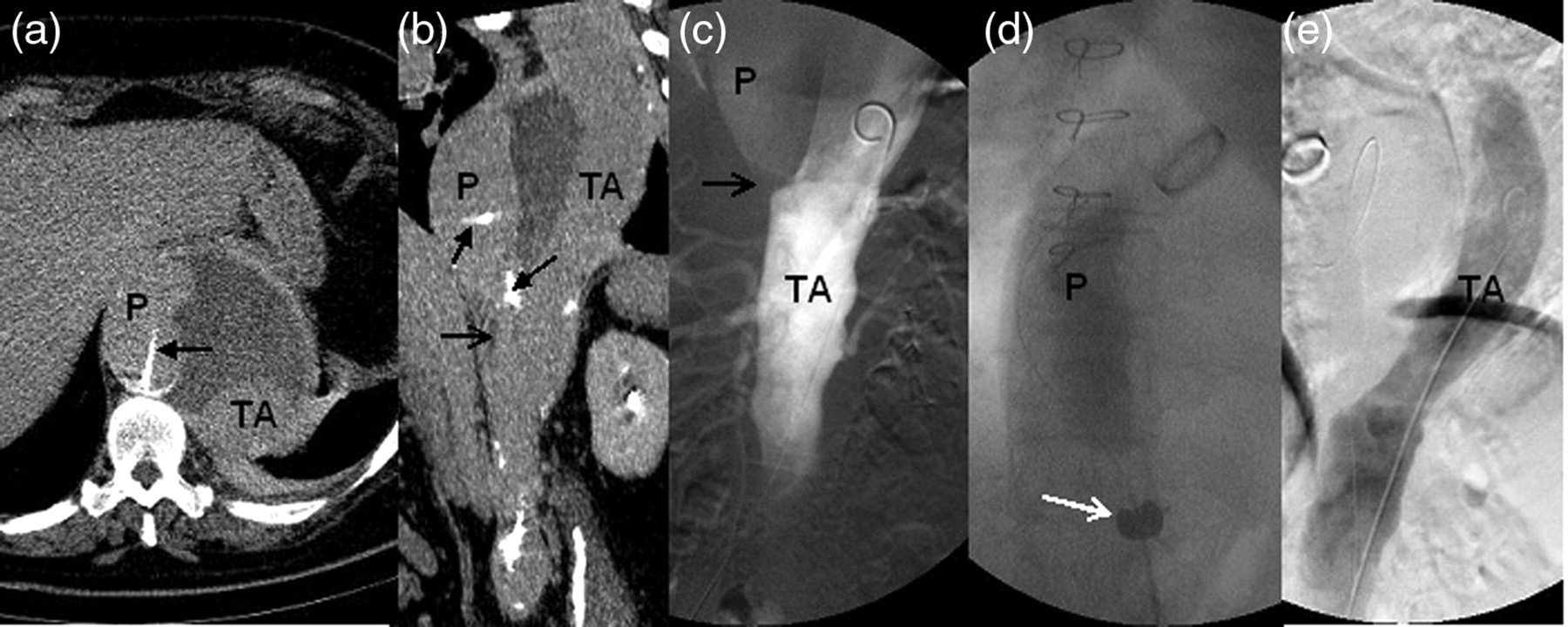
(a, b) Contrast enhanced helical CT and (c, d) digital subtraction angiography (DSA) demonstrating a large pseudoaneurysm (P) of the thoraco-abdominal aorta (TA), characterized by a wide neck of 11 mm in diameter (open arrow); a microcatheter (closed arrows) was placed coaxially through an occlusion balloon catheter (white arrow) in the dome of the pseudoaneurysm; (e) following slow injection of 500 IU thrombin, complete occlusion was observed on DSA
Follow-up examinations were performed by CT angiography (Collimation: 6*2 mm; Pitch: 1.5; 120 mL Iomeprol; 3 mL/sec) at day 1 and week 1. Further follow-up at months 3, 9 and 15 using either MR angiography or CT angiography was performed on an outpatient basis. Evaluation included aortic patency as well as persistent occlusion of the pseudoaneurysms.
Results
All pseudoaneurysms were of single shape and adjacent to an abdominal vascular anastomosis. The mean volume of all pseudoaneurysms was 178 ± 190 mL (range 16–486 mL), with a mean patent lumen of 25 ± 28 mL (range 2–79 mL). The diameter of the pseudoaneurysms was 4.0 ± 2.5 cm (range 0.9–11.2 cm), the diameter of the neck was 2 mm or less in four cases. In case 5 the diameter of the neck was 11 mm as measured on helical CT (Table 1).
All pseudoaneurysms thrombosed following slow injection of an average of 600 ± 237 IU thrombin (range 300–1000 IU), corresponding to 68 ± 49 IU/mL of the volume of the patent lumen (range 6–150 IU/mL). CT-guided procedures lasted for approximately 50 min. No more than four CT angiographies with reduced amount of contrast agent were necessary (average 195 mL). Endovascular embolization required 90 min with injection of 120 mL contrast agent. No thromboembolic complications were detected. Post serum chemistry demonstrated stable creatinine in all cases.
During the mean follow-up period of 10.2 ± 6.5 months (range 3–20 months), all treated pseudoaneurysms remained occluded without complication.
Discussion
A long-term study after open repair of AAA reported on aneurysmal dilatation due to progression of the disease as indication for reoperation in 13.8% (1). Early postoperative pseudoaneurysms, however, are rather unusual. The detection of such abnormalities is dependent on the development of new symptoms, on an incidental finding or on imaging performed for unrelated reasons. Therefore, the true incidence might be underestimated. Endoleaks represent a similar therapeutic challenge. They are defined as blood flow outside the graft but within the aneurysmal sack and are well-known complications following endovascular repair of AAA, with an incidence of 10–20% (7). In open AAA surgery endoleaks are uncommon entities, which were first described by Chan et al. in 2000 (8).
The gold standard in the definitive treatment of postoperative, para-aortic pseudoaneurysm is open surgery. Avoiding the morbidity associated with repeated laparotomy, minimally invasive techniques have become increasingly popular (9). In our cases, endovascular treatment using covered stents was inappropiate due to close visceral arteries. Besides other embolization techniques, such as coils or liquid embolic agents, thrombin has been shown to be a feasible and safe alternative in the treatment of puncture site pseudoaneurysms of the groin (4), and of endoleaks after endovascular repair of AAA (10, 11), respectively. Recently, thrombin has been successfully used for the treatment of pseudoaneurysms of the torso, either as the sole treatment or in combination with other embolization techniques (5, 12). Thrombin converts soluble fibrinogen into insoluble fibrin, and plays a vital role in the coagulation cascade leading to thrombus formation (13). Technical success rates in the treatment of puncture site pseudoaneurysms are up to 90% (14). Complication rates of less than 4% have been reported (15). Dasyam et al. described partial extension of thrombi into the arterial lumen after injection of thrombin into small pseudoaneurysms (16). These complications were asymptomatic and self-limiting. Thromboembolic events have been described by Sadiq et al., rather due to thrombin flowing into the local arterial system than to clot embolization (5, 17). Further complications include allergic reactions as well as infection. There is no evidence of systemic effect on the coagulation system (4).
Thrombin is a non-radiopaque coagulation protein, which starts a physiological process. Therefore, it is less important to observe the thrombin itself, but to control the therapeutic effect. In puncture site pseudoaneurysms in particular, ultrasound has proven to be the method of choice. Following recent abdominal surgery, however, ultrasound may be limited. As there was no reliable method for on-line visualization of thrombus formation, we decided to use CT angiography in case of percutaneous thrombin application (18). Krüger et al. proposed intra-arterial CT angiography using a F-5 pigtail catheter, to reduce the total volume of contrast media (19). In our experience, CT angiography with intravenous injection of 60 mL contrast media seems to be sufficient and less invasive.
Both percutaneous as well as catheter-based delivery of thrombin has been reported (5). Furthermore, various combinations of thrombin with additional embolization material have been used (9, 20). However, the amount of thrombin, which is necessary for successful occlusion of pseudoaneurysms remain unclear. Van den Berg et al. (21) suggested CT-guided injection of 500 IU, while Carmo et al. used two transcatheter injections of 5000 IU thrombin (6). In our experience, quite low amounts of thrombin may be sufficient. In case 5, no more than 6 IU thrombin per mL of the volume of the patent lumen was necessary. On average, we injected 68 IU thrombin per mL of the patent lumen. According to our learning curve, we assume 5–10 IU/mL of the patent lumen to be sufficient. Although all pseudoaneurysms in our series remained occluded, long-term complications such as reperfusion after initially successful treatment have been reported (22, 23).
In conclusion, our series demonstrates the feasibility and safety of thrombin injection in the minimal invasive treatment of postoperative, peri-anastomotic, aortic pseudoaneurysms after ongoing infection has been excluded. In combination with an occlusion balloon catheter, even pseudoaneurysms with a wider neck may be treated. Besides optimized visualization, slow application of thrombin seems to be the best option to prevent thrombembolic complications. However, further studies are needed to determine the amount and concentration of thrombin needed.