
Abstract
Background
The incidence and findings of tuberculous invasion of the peripheral bronchus have not been fully investigated with MDCT.
Purpose
To evaluate the prevalence and findings of MDCT abnormalities of small- and medium-sized bronchus (SMB) in active pulmonary tuberculosis (TB).
Material and Methods
Using multiplanar reformation, 35 consecutive MDCT scans (follow-up exams available in 14 patients with a mean interval of 8.1 months) were assessed for following abnormalities of SMB: bronchial impaction (BI), wall thickening, dilatation, peribronchial cuff of soft tissue, and bronchocavitary fistula. It was also assessed whether tree-in-buds (TIB) have a tendency to distribute in the territories of diseased SMB, and whether SMB abnormalities are present in patients with relatively mild disease.
Results
SMB abnormalities were observed in 23 (65.7%) patients with active TB. The most frequent finding was wall thickening (n = 18, 51.4%), followed by BI (n = 13, 37.1%; zigzag-shaped in four), dilatation (n = 11, 31.4%), amputated appearance of air column (n = 11, 31.4%), peribronchial cuff of soft tissue (n = 10, 28.6%), and bronchocavitary fistula (n =8, 22.9%). TIB (n = 29; absent in two patients with SMB) was mainly within (n = 14) or close to (n = 4) the territory of diseased SMB. Follow-up CT frequently showed improvement of wall thickening (11/12) and persistence of bronchial dilatation (11/13). SMB abnormality was present in all of six patients with mild disease.
Conclusion
MDCT shows that tuberculous invasion of the peripheral bronchus may be more frequent than previously thought, of which findings include wall thickening, BI, dilatation, amputated appearance of air column, peribronchial cuff of soft tissue and bronchocavitary fistula.
Bronchogenic spread of TB occurs from breakdown of a lobar infection or a pulmonary cavitary lesion or from rupture of an infected lymph node into the bronchus (1). The radiologic hallmark of the activity and bronchogenic spread of TB is the ‘tree-in-bud’ appearance, which represents filling of caseous material within the lumen of the terminal bronchioles and peripheral alveolar ducts (2, 3). Actually, however, bronchogenic spread is a process which not only involves the terminal bronchiole and peripheral alveolar duct but also ‘the entire course of a bronchus, including segmental, lobar and mainstem, which leads from a parenchymal lesion’ (4). In 1993 Im et al. reported that TB can invade the bronchus itself and produce CT abnormalities while undergoing bronchogenic spread, albeit without mentioning the level of the involved bronchus (2). Representative findings of this process include wall thickening, bronchial dilatation, and branching tubular opacity (bronchial impaction; BI) with a bulbous end, which is caused by the luminal impaction of caseous material (2). CT findings indicating tuberculous invasion of the central (from the trachea to the segmental) bronchus, or so-called endobronchial TB (EBTB), have been described in detail (5). However, CT findings of TB invading bronchi distal to the segmental bronchus (defined as the small- and medium-sized bronchus [SMB] here) have not been studied systematically after the 1993 article by Im et al. (2), and only BI has been sporadically described using several different terms such as intraluminal mass (6), pigmented polypoid obstructive endobronchial tuberculosis (7), and bronchocele (8). Only recently Cha et al. (9) have shed a new light on this subject by reporting on the CT-pathologic correlation of the medium-sized bronchus invasion by TB. However, the article by Cha et al. was a case series consisting of only eight cases demonstrating such findings, and therefore did not establish the frequency of these findings in patients with active pulmonary TB. On the other hand, before the article by Cha et al., there were reports delving into the incidence of BI in patients with TB; however, these studies were undertaken before the era of multidetector CT (MDCT), making it hard to lend credence to their reported incidence of 7.8 ∼ 17.2% (2, 10, 11). In other words, their findings are difficult to interpret due to limitations in the CT techniques used in those studies, especially the presence of interslice gaps and the inability to perform multiplanar reformation. Now that such technical limitations have been largely overcome with the recent advancement of MDCT, it became much easier to evaluate the true frequency of SMB abnormality with CT. Therefore, we decided to evaluate the incidence of SMB abnormalities using meticulous multiplanar reformation of MDCT in a consecutive group of patients diagnosed with active pulmonary TB.
The purposes of this study were to determine the true frequency of SMB abnormalities in patients with active pulmonary TB, and to discuss their diagnostic importance.
Material and Methods
Patients
The study was approved by the Institutional Review Board, which granted waiver of informed consent. During the study period (March through June 2009), there were a total 139 patients newly diagnosed as active pulmonary TB by means of sputum and/or BAL culture in our institution. Chest radiographs (postero-anterior and lateral) were obtained in all of those patients. Decision to perform MDCT (n = 35; 22 men, 13 women, mean age 49 years) was made in the following situations: non-specific radiographic findings, suspicion of other infections, and suspicion of malignancy. All of those 35 patients were included for a retrospective image analysis. Follow-up CT was done in 14 patients (duration of follow-up ranging from 4–13 months, mean 8.1 months) to decide whether CT findings suggestive of disease activity (TIB, cavity, etc.) were still present.
CT
MDCT scans were obtained with Somatom Definition AS (Siemens Medical Imaging, Forchheim, Germany) with and without intravenous administration of contrast medium (100 cc at 2 ∼ 2.5cc/sec) in 28 and seven patients, respectively. Scanning parameters included a 130 mA tube current, 120 kV tube voltage, 128×0.6 mm collimation, 0.75 mm section thickness, 0.7 reconstruction interval and 1.2 pitch.
Image analysis
Image analysis was performed with a 3D workstation (Aquarius Net, Tera Recon, San Mateo, CA, USA). Primary image analysis was performed based on axial images, in order to ascertain the presence, location, and the distribution of the lesions. In addition to the images reformatted on the three orthogonal (axial, coronal and sagittal) planes, oblique planes were obtained in various directions such as along the long axes of the abnormal SMBs. Typically, it took three to five minutes for the radiologists to perform the multiplanar reformation.
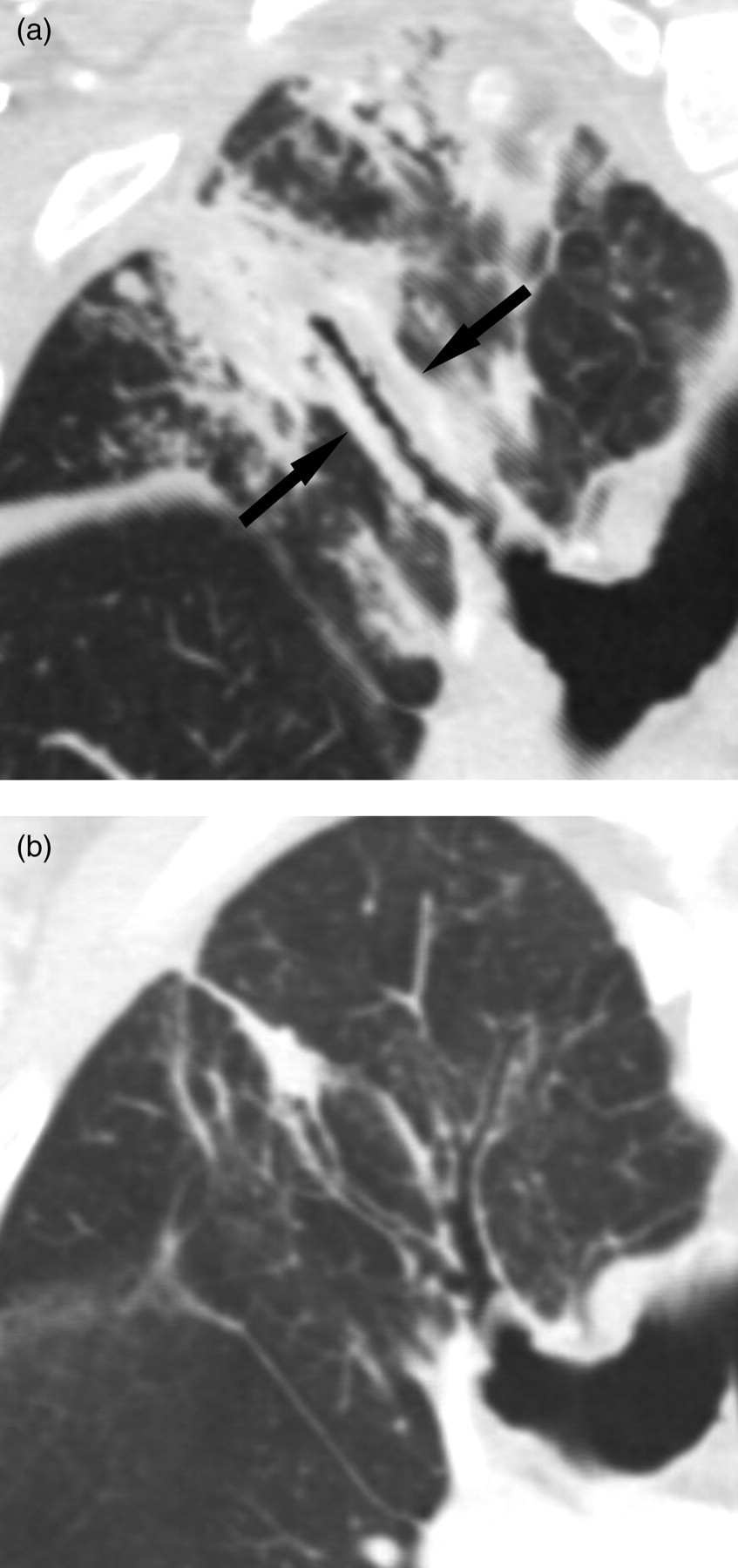
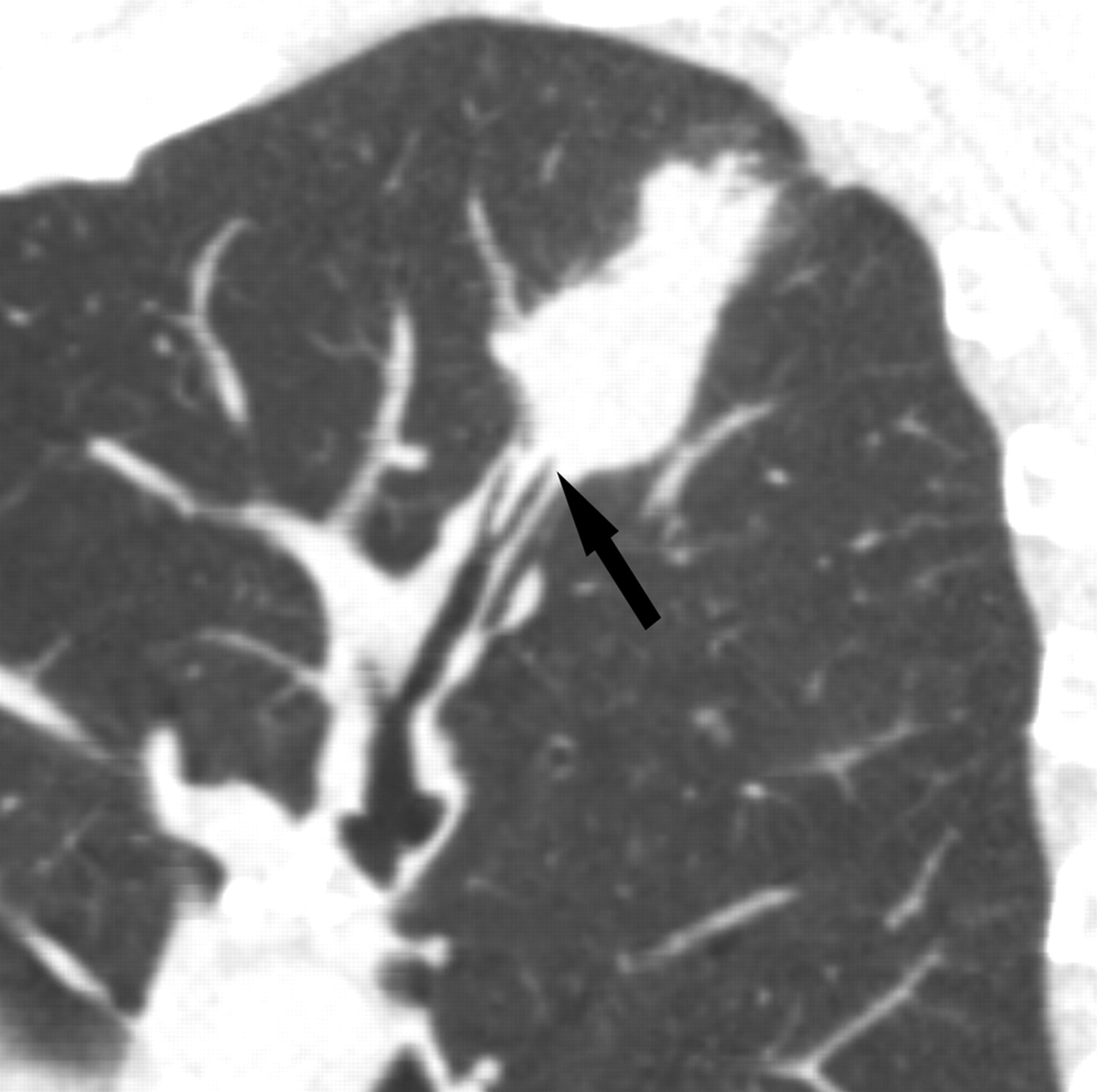
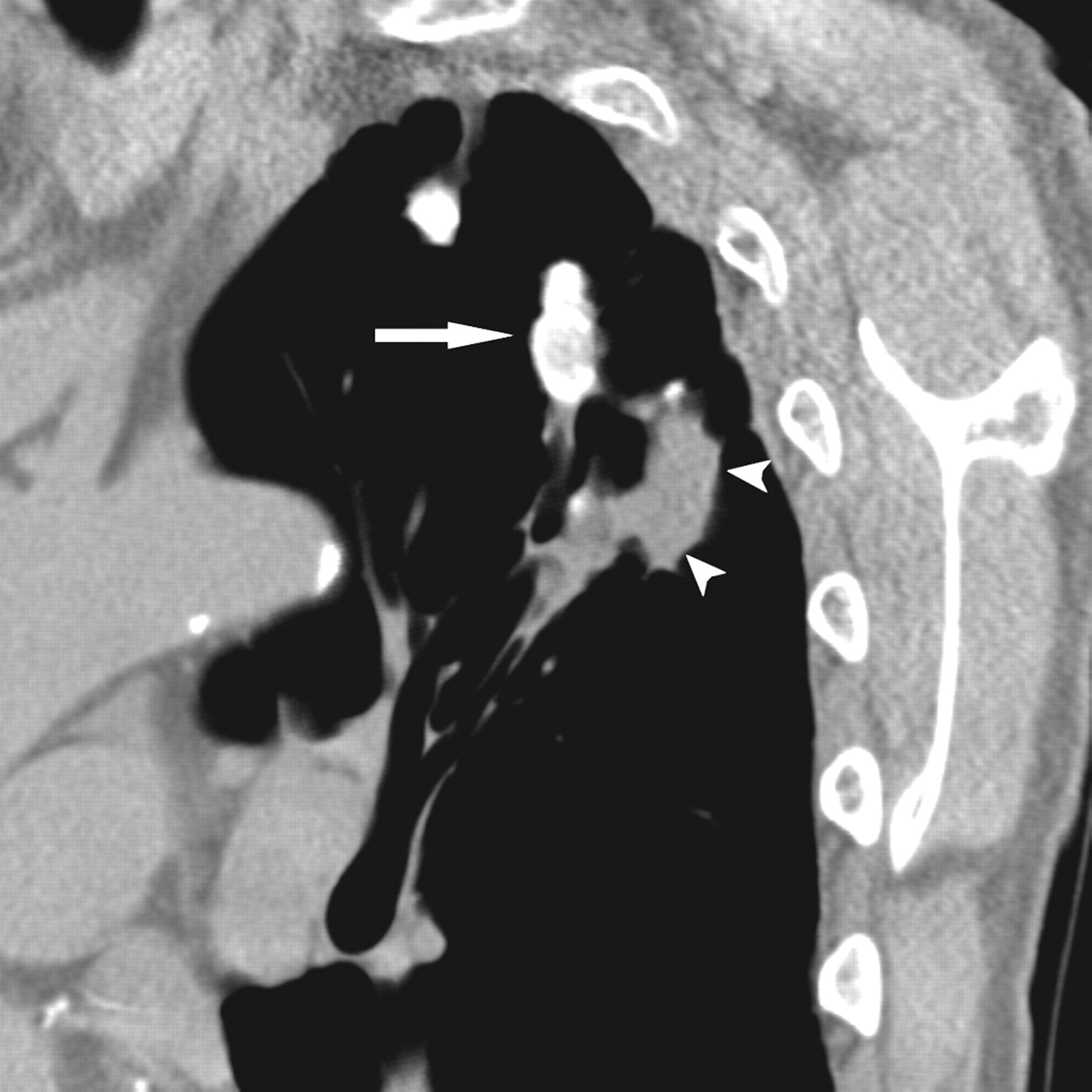
CT images, read by the consensus of two staff radiologists with 8 and 15 years of experience in chest CT, were assessed for the presence of following SMB abnormalities: BI (bronchial impaction or soft-tissue filling of the lumen; Figs. 1 and 2), wall thickening, bronchial dilatation, peribronchial cuff of soft tissue (Fig. 3) and bronchocavitary fistula (Fig. 4).
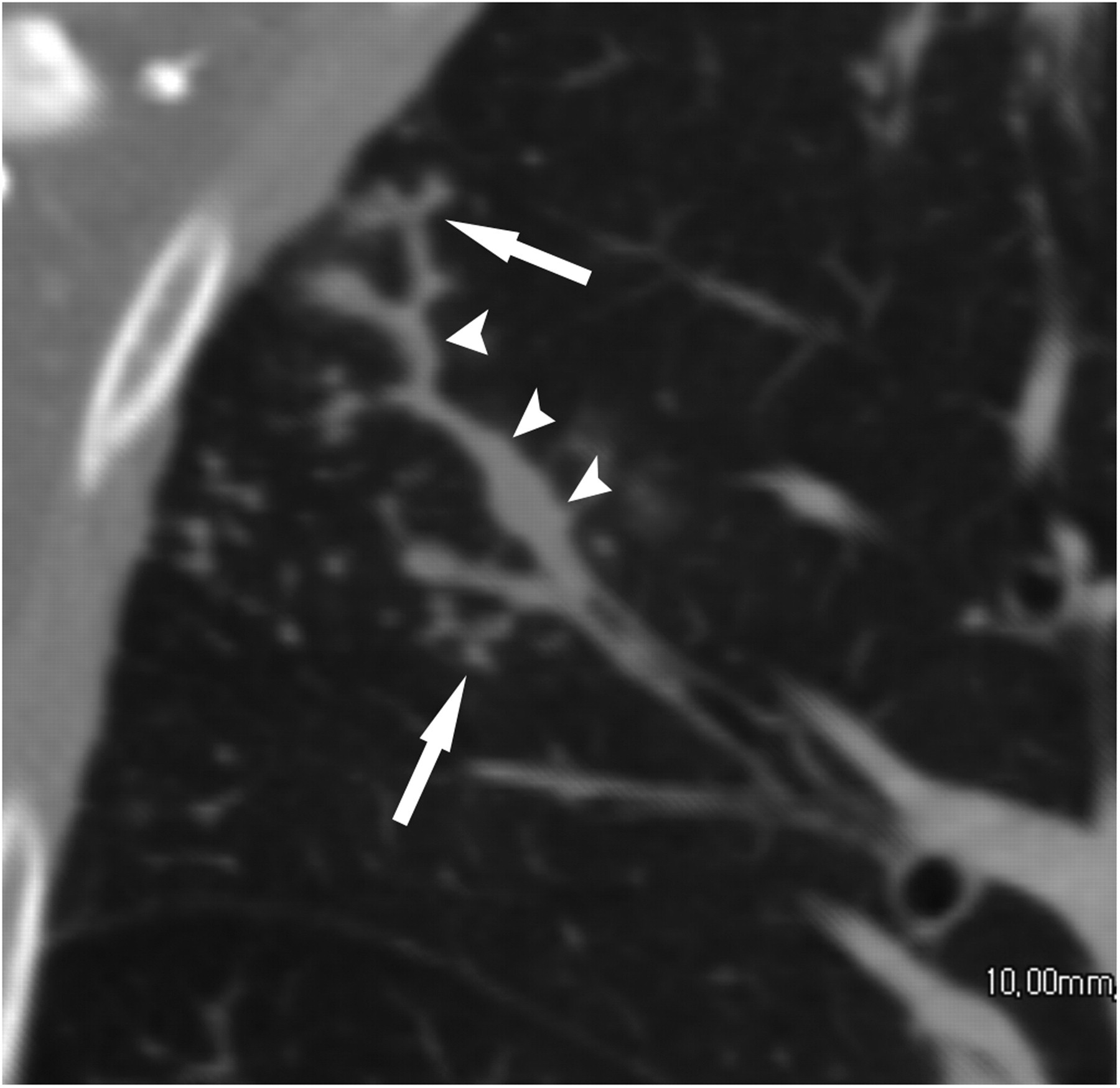
A 29-year-old woman with a zigzag impaction of the small- and medium-sized bronchus (SMB; arrowheads) and the bronchiole (arrows). Note the similarities between the two different entities: impaction of the bronchus and the bronchioles (tree-in-bud appearance)

(a, b) Two consecutive sagittal CT images of a 49-year-old woman with bronchial impaction (black arrows). The lumen of the distal airway is also impacted, producing a tree-in-bud appearance at the level of the bronchiole (white arrow)
A 40-year-old man with peribronchial cuffing of soft tissue (arrows). (a) Note bronchial dilatation at the baseline, with a distally amputated air column; (b) Follow-up CT shows improvement of peribronchial cuffing, wall thickening, distal consolidation and tree-in-bud appearances

A 24-year-old woman with a bronchocavitary fistula. Re-formatted CT scan shows cavitary consolidation in the RUL and ectatic change of the subsegmental bronchus (arrow), which communicates with the cavity
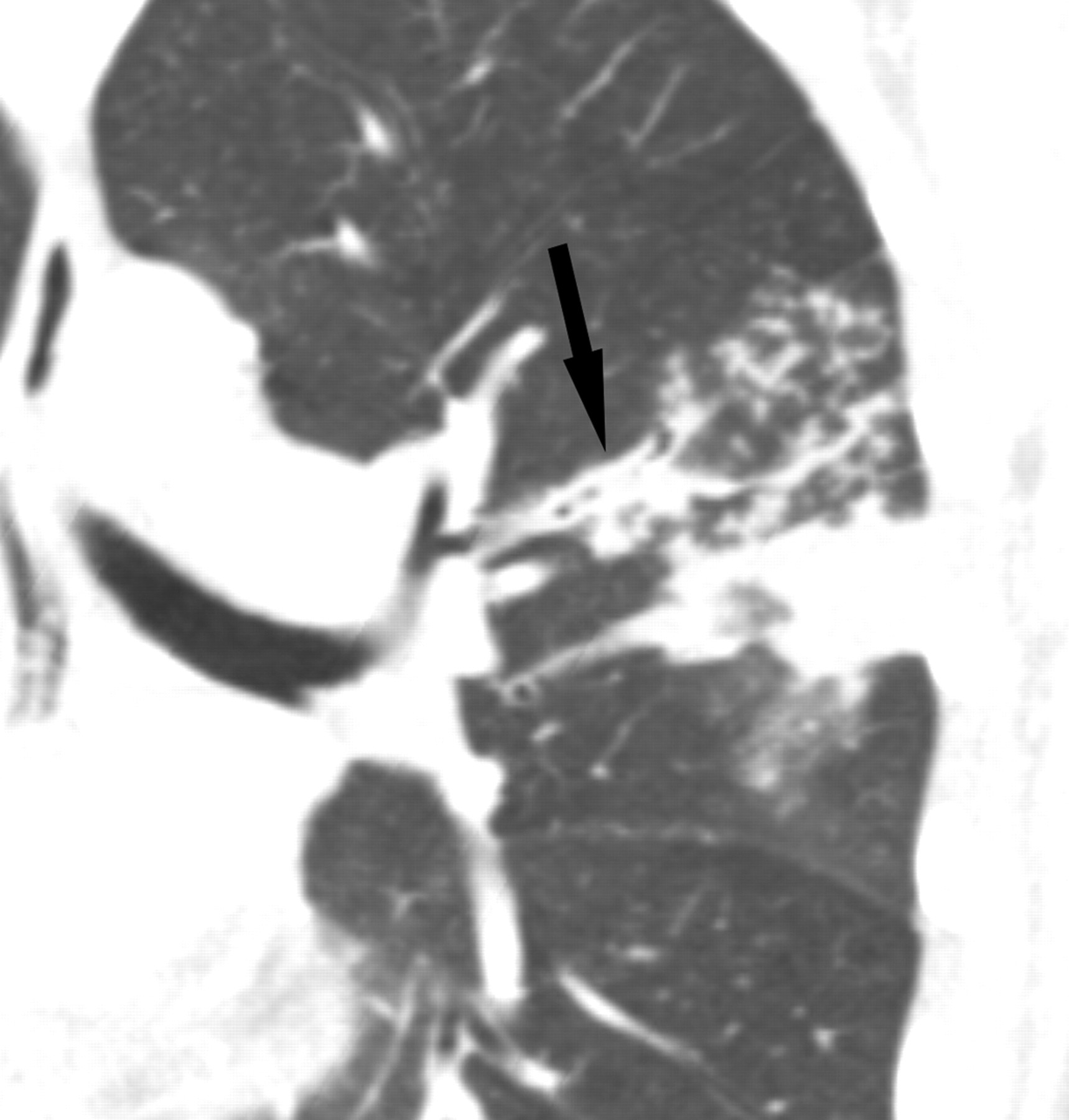
Bronchial wall thickening was defined as the luminal diameter less than 80% of the total bronchial diameter (12). Bronchial dilatation was defined as an increase in bronchial diameter (greater than that of the accompanying pulmonary artery) and a lack of normal bronchial tapering (13). It was also determined whether the air columns of SMB looked as if they were amputated without tapering (air-column amputation), ending abruptly at an area of BI, parenchymal consolidation or a cavity wall (Fig. 5).
Oblique sagittal CT image of a 59-year-old man shows amputated appearance of the air column of a medium-sized bronchus (arrow), produced by a peribronchial consolidation interrupting the airway lumen
In each patient, it was assessed which lobe(s) were involved by one or more of the SMB abnormalities listed above.
The SMB abnormalities located distal to a thickened, obstructed or stenotic central airway (segmental bronchus or above) were considered as post obstructive pneumopathy and were excluded from analysis. Likewise, the SMB abnormalities within a destroyed portion of the lung were excluded since they might have been the results of a prior inflammation rather than that of the current tuberculous process.
When present, the distribution of tree-in-bud appearances (TIB) was assessed in relation to the location of SMB abnormalities: within the territory of abnormal SMB (Fig. 6), concentrated near the territory of abnormal SMB, or independent of the territory of abnormal SMB.
Coronal CT image of a 19-year-old woman shows distribution of tree-in-bud appearances distal to a thickened and impacted medium-sized bronchus (arrow)
To determine whether the abnormalities of SMB can exist in the patients with relatively mild involvement by TB, we arbitrarily defined ‘mild disease’ as follows: (a) less than three lobes are involved; (b) the parenchymal opacities are smaller than 3 cm; (c) no gross abnormalities in the central airway; (d) no effusion; and (e) no lymphadenopathy (LAP; short diameter greater than 1 cm).
Results
The abnormal MDCT findings of SMB have been summarized in Table 1.
Abnormal MDCT findings in small- and medium-sized bronchus in 35 patients with active pulmonary TB
SMB = small- and medium-sized bronchus
MDCT showed SMB abnormalities in 23 patients (65.7%); most commonly in the right upper lobe (n = 12, 34.3%), followed by the left upper (n = 10), right lower (n = 8), left lower (n = 6) and right middle lobes (n = 3). In four of the patients with BI, the bronchi were impacted in such a manner that one distal branch impacted and the other is saved, producing a zigzag appearance (Fig. 1). CT showed SMB abnormalities in two patients with no TIBs: in one of them, BI was the only SMB abnormality; in the other, there were BI and air column amputation. TIBs were noted within (n = 14) or close to (n = 4) the territory of the abnormal SMBs in the vast number of the other 21 patients.
Follow–up CT (n = 14) showed variable interval changes for SMB abnormalities.
However, wall thickening had a tendency to improvement, while bronchial dilatation was persistent in many patients. The details on the follow-up findings are described in Table 2.
Follow-up results of MDCT findings in small- and medium-sized bronchus in 14 patients with active pulmonary TB
SMB = small- and medium-sized bronchus
Six patients were classified to have a mild disease. Bronchial wall thickening was found in all six of them, while BI and amputation were each found in four.
Discussion
The results of the present study reveal that the active TB frequently invades the small- and medium-sized bronchi to produce MDCT abnormalities such as wall thickening, BI, peribronchial cuff of soft tissue, bronchial dilatation, and bronchocavitary fistula. The most common sites of the SMB abnormalities were the upper lobes (22 patients) and the superior segments of the lower lobes (14 patients), which are also the preferential areas of pulmonary lesions in active TB. These results demonstrate the fact that SMB, while functioning as a conduit for migration of TB bacilli, is at the same time invaded by the microorganism.
Although wall thickening can be observed both in the central and peripheral bronchi, the other MDCT features reported in the present study are unique to the latter. Such a difference may be related to the small luminal diameter of SMB which allows retention of an endoluminal granuloma. Moreover, SMBs are surrounded by lung tissue, allowing the formation of a peribronchial cuff of soft tissue or bronchocavitary fistula.
The results of the current study suggest that BI (n = 13, 37.1%) is much more common than previously thought in patients with TB (2, 10, 11). It has been proven in an old (2) and a recent (9) study that BI represents endobronchial granuloma just as TIB does. However, when we searched the literature using various criteria, we found that little attention has been paid to the former as compared to the latter. We searched MEDLINE from January 1980 through July 2010 using two different strategies (tuberculosis[Title/Abstract]) AND ‘tree in bud’[text] AND (English;[lang]); tuberculosis[Title/Abstract]) AND ‘mucoid impaction’[text] AND (English;[lang])). The first search revealed 18 results (17 relevant titles), while the second search revealed only four results (three relevant titles). Such a difference may suggest that BI has not been accepted as widely as TIB as an important CT finding suggestive of bronchogenic spread. This may be partly explained by the difference in size between BI and TIB. Due to its small size (2), TIBs can be included within a CT slice either entirely or partially, which would reveal its branching linear shape. On the other hand, BIs are too large to be included within a single CT slice, and their branching linear shapes can hardly be appreciated on thin-section CT with wide interslice gaps. In addition to the technical limitation of the past, the lack of knowledge may have played a role in the under-recognition of BI: a recent study of TB fails to mention the presence of BI despite the use of MDCT technique (14).
Although much attention has been paid to TIB, the present study shows that the significance of BI is almost equivalent to that of TIB in terms of the imaging diagnosis of TB. Moreover, this study shows that the sole occurrence of BIs can indicate TB reactivation, without accompanying TIBs. Therefore, radiologists should familiarize themselves with BI or other SMB abnormalities for a correct imaging diagnosis of pulmonary TB.
Since TIB is analogous to the larger airway ‘finger-in-glove’ (15) and TB has known tendency to affect the airway (4), it is not surprising the CT abnormalities are similar in the larger and smaller airways. Indeed, the current study shows that BI and TIB are often seen together, with the vast number of TIB located in or close to the territory of the diseased SMB. TIB and BI can even be continuous with each other, as evidently shown in a small number of cases (Fig. 1). It requires further investigation, however, to determine whether the combination of these two findings increases the specificity of MDCT in the diagnosis of bronchogenic spread of TB compared to their occurrences separately.
Unlike TIB, many of BIs and other SMB abnormalities have been shown to be longstanding in this study, sometimes lasting for several months. The reason might be that the luminal surface of those bronchi may be exposed to TB bacilli for a prolonged period of time as the caseous material drains from the alveolar ducts (16).
It is possible that some BIs eventually calcify, considering the similarity between the BIs observed in this study and the calcific endobronchial cast often observed in the peripheral bronchi in our daily patients with inactive TB (Fig. 7). However, the clinical significance of BI or other SMB abnormalities remaining after the completion of anti-TB therapy is still uncertain.
A 59 year-old man with bronchial impaction by calcification. Re-formatted CT scan shows two branches of a peripheral bronchus impacted with calcified (arrow) and non-calcified (arrowheads) tissue, respectively
Of all SMB abnormalities shown by CT in this study, bronchial dilatation had the highest tendency to last without improvement. Long et al. (10) suggested that bronchial dilatation tended to develop late in the pulmonary TB, reporting that it was observed in three of 20 patients in the initial detection and in 10 patients after the completion of anti-TB chemotherapy. On the other hand, the prevalence of initial bronchial dilatation was as high as 48% in the study by Im et al. (2), which was almost comparable to that (58%) in the post-therapy CT. The results of the present study (31.4%) supports the results of the latter study, showing that bronchial dilatation often starts in the active phase of the disease.
The presence of peribronchial cuff of soft tissue suggests that tuberculous inflammation is not confined to the lumen of SMB, but rather extends to the surrounding lung tissue. However, the peribronchial distribution of such soft tissue was often striking, implying perilymphatic spread of the disease along the bronchovascular bundle.
In the study on NTM lung infection by Kim et al. (17), bronchocavitary fistula, or feeding bronchus sign, was a very frequent CT finding (75%). The incidence of bronchocavitary fistula was much lower in the current study of TB, observed only in eight patients (22.9 %). However, we believe that tuberculous bronchocavitary fistula evolves from bronchial wall thickenings or peribronchial nodules, just as they do in NTM lung infection (17).
The CT findings shown in this study are similar to the study by Lee et al. (18), who studied thin-section CT findings in 22 EBTB patients, although they did not separate abnormalities of the segmental bronchus from those of the more distal bronchi. Another difference between the two studies is that all of the patients studied by Lee et al. were bronchoscopically diagnosed as EBTB while our patients were diagnosed by sputum or BAL culture. Still, the similarity in the CT findings is striking. This makes one re-think the concept of EBTB. Contrary to the connotations of the term ‘endobronchial’ TB, the current study shows that abnormalities of the small- and medium-sized airways in patients with pulmonary TB are not so exceptional.
Due to the technical limitations and poor recognition, the SMB abnormality has not been utilized widely in the diagnosis of TB. However, now that MDCT is being used conventionally, it would be helpful to pay closer attention to and familiarize oneself with the MDCT findings of tuberculous SMB abnormalities.
There are limitations to the present study. Pathologic proof was available in only a few patients (n = 3), making us rely on previous studies for the pathologic explanation. Second, although the patients were collected in a consecutive manner, thin-section CT data enabling multiplanar reformation were available in only 35 patients, causing bias to the results. Third, we did not compare the performance of axial and multiplanar reformation images for the detection of SMB abnormalities, although it is almost intuitive that multiplanar reformation, especially that oriented along the long axes of an abnormal bronchus, would be helpful for an accurate characterization of SMB. Fourth, although the medium-sized bronchi were fairly well assessable with MDCT, the resolution of CT was not enough for evaluation of smaller bronchi. Fifth, due to relatively short periods of follow-up (mean 8.1 months), this study failed to reveal the long-term fate of SMB abnormalities. More studies are needed to find out the implication of SMB abnormalities in the post-therapeutic follow-up of TB patients.
In conclusion, MDCT commonly shows signs of tuberculous invasion of the peripheral bronchus, such as wall thickening, BI, peribronchial cuff of soft tissue, bronchial dilatation, air column amputation, and bronchocavitary fistula. Familiarity with these CT features will help radiologists make accurate imaging diagnosis of pulmonary TB.