
Abstract
Background
Several studies have reported the effectiveness of high b-value diffusion-weighted MR imaging (DWI) in the abdominal region, and have found that various malignant tumors may show high signal intensity on DWI, reflecting their high cellularity and/or their long relaxation time. The value of ADC measurement has also been documented for the diagnosis of several abdominal malignancies.
Purpose
To retrospectively evaluate the usefulness of high b-value DWI in differentiating between benign and malignant polypoid gallbladder lesions.
Material and Methods
The study population consisted of 10 benign (three hyperplastic polyps and seven adenomas) and 13 malignant (all adenocarcinomas) polypoid gallbladder lesions. DWI was evaluated by two observers. Qualitatively, the signal intensity of the lesions on DWI was visually evaluated and categorized as iso, high, or very high. Quantitatively, the ADC values of the lesions were measured from ADC maps. Statistical analysis was performed using a two-tailed Fisher's exact test and the Mann-Whitney test, respectively.
Results
Qualitative analysis revealed a statistical difference (P = 0.0041). Six of 10 benign lesions were categorized as iso, and the remaining four were categorized as high. In the 13 malignant lesions, one was categorized as iso, five as high, and seven as very high. The ADC values of the malignant lesions (1.34 ± 0.50 × 10–3 mm2/sec) were significantly lower than those of the benign lesions (2.26 ± 0.44 × 10–3 mm2/sec) (P = 0.00016).
Conclusion
High b-value DWI may be useful for differentiating between benign and malignant polypoid gallbladder lesions by the visual assessment of DWI and ADC measurement.
Gallbladder carcinomas are the most common malignant tumor of the biliary tract (1). A preoperative diagnosis is important, since advanced and potentially curative radical surgical techniques are increasingly used (1). Although the usefulness of MRI for diagnosing gallbladder abnormalities has been recognized (2–4), MRI cannot always differentiate a gallbladder carcinoma from other conditions (5, 6). When considering differential diagnoses of gall bladder carcinomas, it may be appropriate to categorize them morphologically into three subtypes: polypoid, diffuse wall thickening, and exophytic (7). The differential diagnosis of a polypoid gallbladder lesion includes cholesterol polyp, hyperplastic polyp, inflammatory polyp, adenomyomatosis and adenoma, and adenocarcinomas. In general, malignant lesions are larger than benign lesions, and polypoid lesions greater than 10 mm in diameter raise the possibility of malignancy (4). However, the prevalence of malignancy in gallbladder polyps greater than 10 mm ranges from 37–88%, and benign gallbladder polyps greater than 1 cm in diameter are not infrequent (8). It has been reported that enhancement patterns on dynamic MRI can be useful in differentiating between benign and malignant polypoid gallbladder lesions. That is, the former usually shows early enhancement with subsequent washout, while the latter demonstrates early and prolonged enhancement (7). However, the opposite findings have also been reported, that benign gallbladder polyps show contrast enhancement that is best seen on delayed images (4). Thus, it is still a diagnostic challenge to differentiate benign from malignant polypoid gallbladder lesions.
Diffusion-weighted MR imaging (DWI) has enabled us to obtain additional information derived from the microscopic motion of water protons, which is not possible using conventional MR imaging. An experimental study found an inverse correlation between the apparent diffusion coefficient (ADC) calculated from DWI and tumor cellularity (9). The introduction of parallel imaging, which enabled the TE, echo-train length, and k-space filling time to all be reduced, led to substantially fewer motion artifacts at image acquisition, and thus provided much improved images in high b-value DWI (10). As a result, the effectiveness of high b-value DWI in the abdominal region has been reported in several studies, and various malignant tumors may show high signal intensity on DWI, reflecting their high cellularity and/or their long relaxation time (11–14). ADC measurement has also proven valuable for the diagnosis of several abdominal malignancies (13, 14).
The purpose of our study was to retrospectively evaluate the usefulness of high b-value DWI for differentiating between benign and malignant polypoid gallbladder lesions.
Material and Methods
The institutional review board at our hospital did not require us to obtain written informed consent for this study, due to its retrospective nature. This study was designed and conducted in accordance with the Declaration of Helsinki. From January 2007 to February 2010, 23 patients (six men, 17 women; mean age 69 years, range 40–85 years) had surgically proven polypoid gallbladder lesions (size range 1.0–3.3 cm, mean 1.86 cm), 10 benign, and 13 malignant. The benign lesions included three hyperplastic polyps and seven adenomas (size range 1.0–2.0 cm, mean 1.36 cm), while all malignant lesions were adenocarcinomas (size range 1.0–3.3 cm, mean 2.17 cm). Malignant lesions were significantly larger than benign lesions (P = 0.0014, Student's t test). All patients underwent diffusion-weighted MRI within three weeks before surgery. These 23 lesions constituted the study population.
MR imaging technique
MR imaging was performed with a 1.5-T MR unit (Siemens; Avanto, Erlangen, Germany) with the use of a dedicated abdominal eight-channel surface coil. Parallel image-encoding techniques were employed. An axial respiratory-gated echo-planar diffusion-weighted sequence with spectral fat saturation was performed by using the following parameters: b-values of 0 and 1000 (with diffusion-weighted gradients applied in three orthogonal directions) sec/mm2; repetition time (TR) msec/echo time (TE) msec 2951–5858/67–72; five to seven signals acquired; echo train length (ETL) 1; flip angle (FA) 90°; section thickness 5 mm; slice gap 1 mm; field of view (FOV) 206–270 × 300–360; matrix 128 × 64–80; and acquisition time 3–5 min. The ADC map was then automatically generated on the imager console from the DW sequence, and ADC values were obtained by measuring the intensity of the map. Routine MR examinations including T1-weighted images, T2-weighted images, MR cholangiopancreatography, and dynamic contrast-enhanced T1-weighted study were also performed, but those images were not evaluated in this study. However, respiratory-triggered fast spin-echo T2-weighted images were used for the reference images of gallbladder lesions in image analysis. The parameters for T2-weighted images were as follows: TR/TE 3152-6442/75 msec; one signal acquired; ETL 9; FA 150°; section thickness 5 mm; slice gap 1 mm.
DWI was evaluated by two observers with a picture archiving and communication system that enabled them to change the window level and window width of an image suitable for evaluation. They were blinded to the histological diagnoses of the lesions. T2-weighted images were provided for reference in the detection of gallbladder lesions. Qualitatively, the signal intensities of the gallbladder lesions on DWI were visually evaluated and categorized as iso (isointense to adjacent liver), high (hyperintense to adjacent liver, but hypointense to spleen), or very high (hyperintense equal to spleen). Agreement between the two radiologists was reached after careful individual evaluation. The results of benign and malignant polypoid gallbladder lesions were compared by using the two-tailed Fisher's exact test. A value of P < 0.01 was considered statistically significant.
ADC values of the lesions were quantified in a circular region of interest (ROI) within the gallbladder lesions from ADC maps. ADC was measured by another observer who had not performed qualitative analysis. All gallbladder lesions were detected on ADC maps by changing the window level and window width appropriately. The circular ROI was placed so as to cover the largest possible area of the lesion in ADC maps (Figs. 1c and 2c). If there was a very high area indicating necrosis, this area was planned to be excluded from the ROI setting, although we did not encounter any such cases. Care was taken to avoid including in the ROI any area outside the lesions. The ADC values of the benign and malignant polypoid gallbladder lesions were compared by using the Mann-Whitney test. A value of P < 0.01 was considered statistically significant.

A 74-year-old woman with hyperplastic polyp. (a) T2-weighted MR image shows a polypoid lesion (arrow) 17 mm in diameter within the gallbladder; (b) High b-value DWI shows no high signal intensity within the gallbladder; (c) Circular ROI was placed so as to cover as much as possible the large area of the lesion in the ADC map. The ADC value in the polyp was 2.39 × 10−3 mm2/sec

An 80-year-old woman with gallbladder carcinoma. (a) T2-weighted MR image shows polypoid lesion (arrow) 22 mm in diameter within the gallbladder; (b) Polypoid lesion (arrow) shows high signal intensity, the same as the splenic parenchyma (arrowhead) in high b-value DWI; (c) The ADC value in the polyp was 1.25 × 10−3 mm2/sec measured by ROI placement in the polyp on the ADC map
Finally, in order to ascertain reproducibility and reliability of ROI setting and ADC measurements, two observers who had performed qualitative analysis did ADC measurements twice with interval of more than 24 hours. Using those data-sets, intra- and interobserver variance was calculated. Coefficients of variation were applied for intra- and interobserver variance.
Results
For qualitative analysis, six of 10 benign lesions were categorized as iso (Fig. 1) and the remaining four were categorized as high. No benign lesions were categorized as very high (i.e. DWI hyperintensity corresponding to the spleen). In 13 malignant lesions, one was categorized as iso, five as high, and seven as very high (Fig. 2). There was a statistically significant difference in signal intensity between benign and malignant polypoid gallbladder lesions (P = 0.0041).
The ADC values of the benign and malignant lesions are presented as a scatterplot in Fig. 3. The ADC values of the malignant lesions (average ± standard deviation: 1.34 ± 0.50 × 10−3 mm2/sec) were significantly lower than those of the benign lesions (2.26 ± 0.44 × 10−3 mm2/sec) (P = 0.00016).
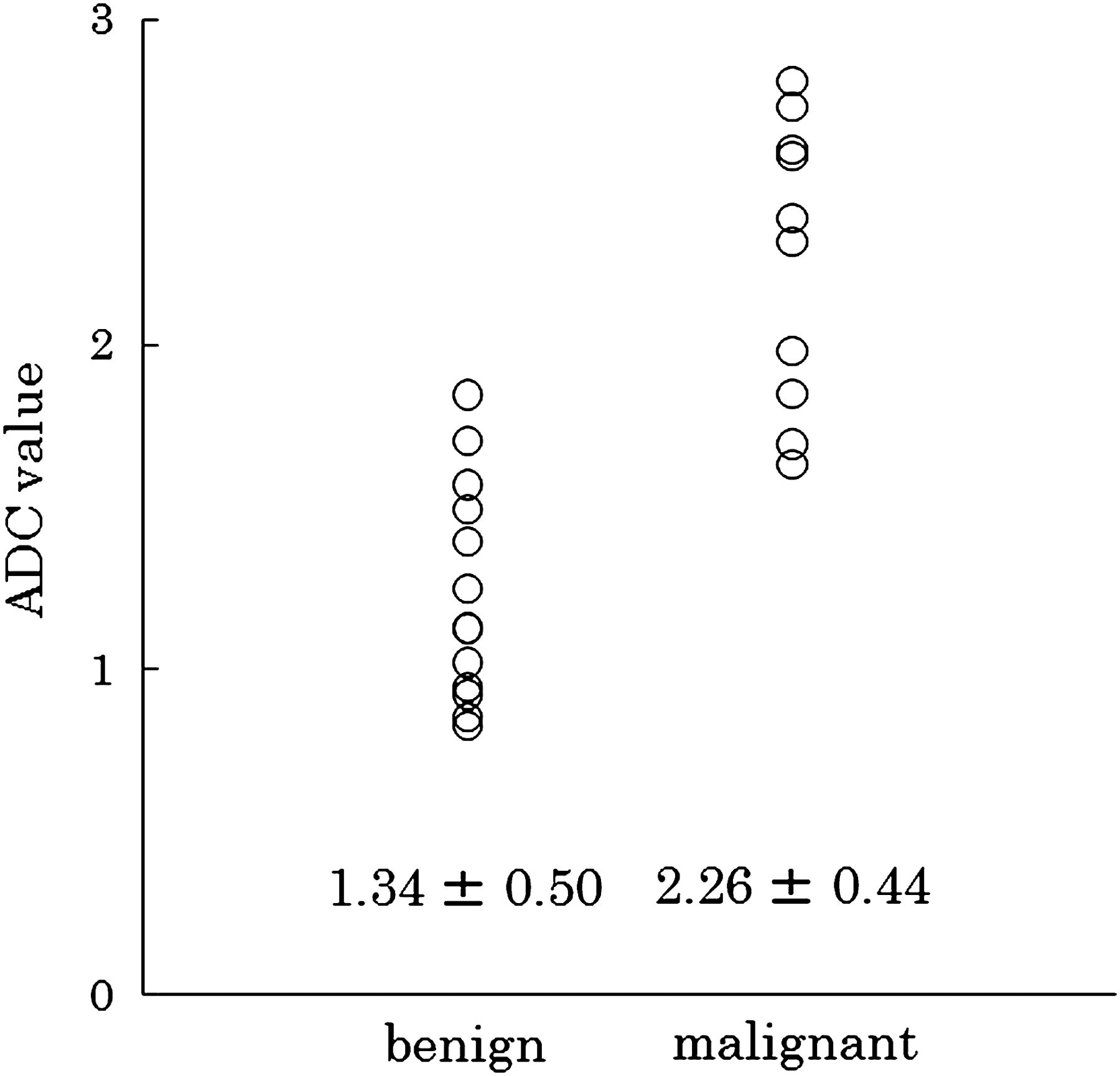
Scatterplot of the ADC values of benign (left column) and malignant (right column) lesions. The number below each column is the mean ADC value ± standard deviation (ADC value: × 10−3 mm2/sec)
Coefficients of variation for intraobserver variance were 3.80% and 3.93%, while those for interobserver variance were 3.14% and 3.59%.
Discussion
DWI can offer both quantitative and qualitative information that is helpful for tumor assessment (9). Tumors can be quantitatively assessed by calculating ADC after performing DWI using different b-values. ADC values in malignant lesions generally tend to be decreased, probably due to increased tissue cellularity or cell density, because the latter correlates with malignancy. In addition to the cellular membranes, intracellular cytoskeleton, organelles, matrix fibers, and soluble macromolecules contribute to diffusion restrictions in tumors (9). Therefore, ADC values are expected to reflect histological tissue characteristics. In fact, several authors have reportedly decreased ADC values in various malignant lesions of abdominal organs (13, 14). Recently, Sugita et al. applied DWI to the diagnosis of gallbladder carcinoma and benign gallbladder lesions, and have reported the usefulness of DWI (15). Although that was the first and only report of DWI applied to gallbladder carcinomas, their main concern was the detection of gallbladder carcinomas, and the number of polypoid gallbladder lesions in their study was fairly small: eight carcinomas and only three benign polyps. Thus, we undertook this study in order to differentiate between malignant and benign polypoid gallbladder lesions.
The results of our study demonstrated the clinical potential of DWI in differentiating between malignant and benign polypoid gallbladder lesions. In the visual or qualitative assessment of DWI, the malignant lesions demonstrated statistically higher signal intensity on DWI than the benign lesions. All but one malignant lesion showed higher signal intensity than the surrounding tissues or very high signal intensity equal to that of the splenic parenchyma. The lesion that did not show high signal intensity on DWI was a very small adenocarcinoma arising from a hyperplastic polyp. In other words, it was composed mainly of a hyperplastic polyp. Six of 10 benign lesions did not show high signal intensity on DWI; therefore, when a polypoid gallbladder lesion does not show high signal intensity on DWI, it is highly suspected to be benign. No benign lesions showed very high signal intensity equal to that of the splenic parenchyma; thus, gallbladder polyps demonstrating high signal intensity equal to that of the splenic parenchyma in DWI should be considered malignant. However, we should recognize that both benign and malignant gallbladder polyps can demonstrate high signal intensity compared to the surrounding tissues in DWI. In such cases, visual assessment of DWI alone cannot provide additional useful information, and ADC measurement might be needed.
In the quantitative assessment, ADC values of malignant lesions were statistically lower than those of benign lesions. The mean ADC value of malignant lesions in our study (1.34 ± 0.50 × 10−3 mm2/sec) was almost the same as that in a previous study (1.28 ± 0.41 × 10−3 mm2/sec) (15), which applied the same b-value of 1000 sec/mm2. In our study, only two lesions showed overlapping ADC values between benign and malignant lesions. ADC values were lower than 1.6 × 10−3 mm2/sec in 11 of 13 malignant lesions, whereas in all benign lesions the ADC values were higher than 1.6 × 10−3 mm2/sec. When the cut-off was set at 1.6 × 10−3 mm2/sec, the sensitivity, specificity, and accuracy were 85%, 100%, and 92%, respectively. One of the malignant lesions with an ADC value above 1.6 × 10−3 mm2/sec was a lesion that did not show high signal intensity on DWI; this lesion was composed mainly of a hyperplastic polyp and contained very small foci of adenocarcinoma. Another malignant lesion, with a higher ADC value, was a well-differentiated adenocarcinoma that was difficult to differentiate from adenoma even pathologically. Thus, these small or early-stage malignant lesions cannot be diagnosed correctly by measuring ADC values.
Coefficients of variation for intra- and interobserver variance were considered to be small, thus we believe that ADC values of polypoid gallbladder lesions can be reproducible and reliable.
The advantage of DWI is that it is completely non-invasive, does not require contrast material, and can be easily added to a routine MR examination protocol since it requires only a very short prolongation of the examination time (12). Although it may not always be possible to discriminate between malignant and benign polypoid gallbladder lesions by visual assessment of DWI or measurement of ADC values alone, they may provide useful additional information that cannot be obtained in other MR examinations. We conclude that DWI should be added to the routine MR protocol for diagnosing polypoid gallbladder lesions.
There are some limitations to our study. First, the study was conducted retrospectively and the study population was relatively small, so the results need to be confirmed in larger prospective studies. Second, the malignant lesions were statistically larger than the benign lesions, and this difference may have influenced our results. Third, our results may not influence patient management, because polypoid gallbladder lesions larger than 1 cm in diameter are usually an indication for surgical resection (4). However, the results of our study may be useful in limited situations. For example, when a patient for whom an operation would be risky due to poor condition has a polypoid gallbladder lesion, the operation may be avoided if the lesion does not show high signal intensity on DWI and a higher ADC value.
In conclusion, high b-value DWI may be useful in differentiating between benign and malignant polypoid gallbladder lesions by the visual assessment of DWI and ADC measurement.