
Abstract
Background
Diagnosis of mucinous carcinoma can be difficult due to its benign appearance on mammograms and ultrasonographic (US) images. In the light of the rather scarce literature, core needle biopsy (CNB) has proved useful in diagnosing mucinous lesions.
Purpose
To assess mammographic, US, and CNB findings of mucinous breast tumors and to correlate them with final histology obtained in therapeutic surgery.
Material and Methods
From 2000–2006, 25 mucinous carcinomas detected with CNB were surgically removed. The mammography, US, and CNB results were analyzed and correlated with final histology.
Results
Ninety-six percent of the mucinous carcinomas (24/25) were visible with US. All except two of the 24 tumors were solid masses. All the mixed-type lesions (group 2) were hypoechoic and had irregular or lobulated margins and heterogeous internal echotexture. The US features were more variable among the 14 pure mucinous carcinomas (group 1) and the six US visible mucinous carcinomas with cancerous cells outside the tumor (group 3). Fifty-seven percent of group 1 and 50% of group 3 tumors had clearly lobulated or irregular margins. Fifty-seven percent of group 1 and 67% of group 3 cancers were hypoechoic. A vast majority of these tumors had heterogenous echotexture. Seventy-one percent (17/24) of the lesions visible with US had posterior acoustic enhancement. Eighty percent (20/25) of the mucinous carcinomas were classified as BI-RADS 4 lesions in US. All the lesions with images available were visible on mammograms, where most of the tumors were seen as a high-density circumscribed lesion and classified as BI-RADS 4 lesions, while none were classified as BI-RADS 1, 2 or 5. The sensitivity and positive predictive value of CNB regarding mucinous carcinoma was 100%.
Conclusion
CNB was found to be a highly reliable diagnostic tool for diagnosing mucinous carcinoma in this selected material. US findings of pure mucinous carcinoma were variable, however, all reached BI-RADS 4 category. The presence of posterior acoustic enhancement beneath a solid breast lesion should raise suspicion of mucinous carcinoma. Most of the tumors appeared as BI-RADS 4 lesions in US and in mammography thus making both a useful tool for raising a suspicion of malignancy in mucinous cancers.
Pure and mixed (non-specific invasive carcinomas containing a mucinous component) mucinous carcinomas each account for about 2% of all breast cancers (1–3). Slow growth rate, rare occurrence of nodal metastasis, and a more favorable overall prognosis are attributed to pure mucinous carcinoma in comparison with ductal or mixed-type carcinoma (1, 3–6).
Although specific imaging findings are lacking, mucinous carcinoma of the breast shows different features that depend on its histologic type (7). A typical mammographic appearance of pure mucinous carcinoma includes a relatively well-defined lobulated mass that rarely calcifies (8), whereas irregular margins are more characteristic of mixed mucinous tumors (2, 7). The mammographically benign appearance of pure mucinous carcinoma can easily cause a delay in diagnosis. Sonographically, hypoechogenicity, mixed cystic and solid components, distal enhancement, and (micro)lobulated margins have all been reported (9–11).
Identification of mucinous lesions on the basis of fine needle aspiration, let alone distinguishing between benign and malignant lesions, can be difficult (12, 13). On the other hand, core needle biopsy (CNB) has proven its worth in diagnosing mucinous lesions, although literature specifically focusing on this topic is relatively scarce (14, 15).
The purpose of this study was to evaluate radiological and CNB findings of mucinous carcinoma of the breast and to correlate them with final histology obtained in therapeutic surgery.
Material and Methods
During 2000–2006, the pathology database of our hospital was searched for surgically treated mucinous breast tumors. Patients who underwent both CNB and surgery were included. Patient charts were examined for information on clinical, radiological, and surgical data.
The study population consisted of 25 patients with 25 mucinous breast carcinomas, which were divided into the following categories according to the histological finding by excisional biopsy: (1) pure mucinous carcinoma (n = 14); (2) mucinous carcinoma with intraductal carcinoma (DCIS) and/or invasive carcinoma within/at the edge of the tumor (n = 4); and (3) mucinous carcinoma with DCIS and/or invasive carcinoma in the vicinity of the tumor (n = 7). One case classified as pure mucinous carcinoma had additional ductal invasive carcinoma, but since it was located far from the mucinous tumor (in a different quadrant), it was not considered a mixed type in the imaging analysis. One lesion (multifocal mucinous carcinoma with DCIS) with calcification as the sole finding based on written information in the patient charts was excluded, since original mammograms and US images were lost. Consequently, it remained unclear whether calcifications were related to DCIS or to mucinous carcinoma. In addition, this material does not include cases without preoperative CNB. The average age of the patients was 63.5 years (median 64 years, range 30–82 years).
All the patients underwent ultrasonography performed with HDI 5000 equipment (Advanced Technology Laboratories, Bothell, WA, USA) and a 5-cm-wide linear multifrequency probe operating at 5–12 MHz. Six of the patients were not scheduled for mammography or the mammograms were lost. The US images (all lesions, one of the tumors in group 3 was not visible with US) and available mammograms (19 lesions) were analyzed by two radiologists (MKB, TR). The lesions were evaluated for their size, margin, echogenicity, echotexture, and acoustic transmission, as well as shape and density. Both US and mammography features were categorized according to the American College of Radiology (BI-RADS) classification for breast imaging.
Biopsies were performed under US guidance (22 lesions) or under stereotactic guidance (three lesions) using a spring-loaded biopsy instrument and either a 16-gauge (14 cases) or a 14-gauge (three cases) needle; in the remaining eight lesions the size of the needle was not reported. Two to six core samples were obtained; the most frequent number of samples was two or three per lesion (eight each). Imaging findings and findings from the CNBs were correlated with the final pathology at surgical excision. When appropriate, statistical analysis was performed using a 2-tailed Student's t-test, and a significant difference was determined with p < 0.05.
Results
Of all the lesions, 76% (19/25) were palpable. Of the six non-palpable tumors, three were pure mucinous carcinomas, one was of a mixed type, and two were mucinous carcinomas with separate DCIS/invasive carcinoma. Analysis of size was based on US, except for one tumor in group 3 which appeared only on mammograms. The average maximum diameter of the pure mucinous carcinomas was 2.3 cm (median 2.5 cm, range 0.8–4.7 cm); the respective values of the mixed mucinous carcinomas and mucinous carcinomas with separate cancerous foci were 1.8 cm (median 1.7 cm, range 1.2–2.7 cm) and 1.6 cm (median 1.6 cm, range 0.7–2.2 cm). The groups did not differ statistically in terms of size. The sonographic and mammographic findings of the mucinous carcinomas, correlated with the final histological diagnoses, are presented in Tables 1 and 2.
US findings of mucinous breast carcinoma correlated with final histology
*Missing one lesion not visible with US, accounted for in the BI-RADS classification
†Includes two mixed solid and cystic lesions
Mammography findings of mucinous breast carcinoma correlated with final histology. Nineteen cases with mammograms available for review
Ultrasonographic findings
On the ultrasonographic images, most of the visible lesions (22/24) were solid (Fig. 1A) and only two, both pure mucinous carcinomas, had a mixed solid and cystic appearance (Fig. 2A). All four mixed mucinous carcinomas (group 2) had a lobulated or irregular margin, were hypoechoic in relation to fat and had heterogeneous internal echotexture (Fig. 3). US features were more variable among the 14 pure mucinous carcinomas (group 1) and the six US-visible mucinous carcinomas with cancerous cells outside the tumor (group 3). Fifty-seven percent (8/14) of the pure mucinous carcinomas and 50% (3/6) of the group 3 cancers had lobulated or irregular margins and the rest had smooth margins with or without 1–2 lobulations. Fifty-seven percent (8/14) of the pure and 67% (4/6) of the group 3 cancers were hypoechoic and the rest were iso- or hyperechoic (Fig. 4), and 83% (10/12) of the solid pure and 83% (5/6) of the US-visible group 3 cancers had heterogeneous internal echotexture, while the remaining three lesions were homogeneous. Most of the lesions had posterior acoustic enhancement: 79% (11/14), 50% (2/4), and 67% (4/6) for groups 1, 2, and 3, respectively (Table 1). Eighty percent (20/25) of the mucinous carcinomas were classified as BI-RADS 4 lesions, two were classified as category 3 and two as category 5 lesions. The one lesion not visible on US was classified as BI-RADS 1.

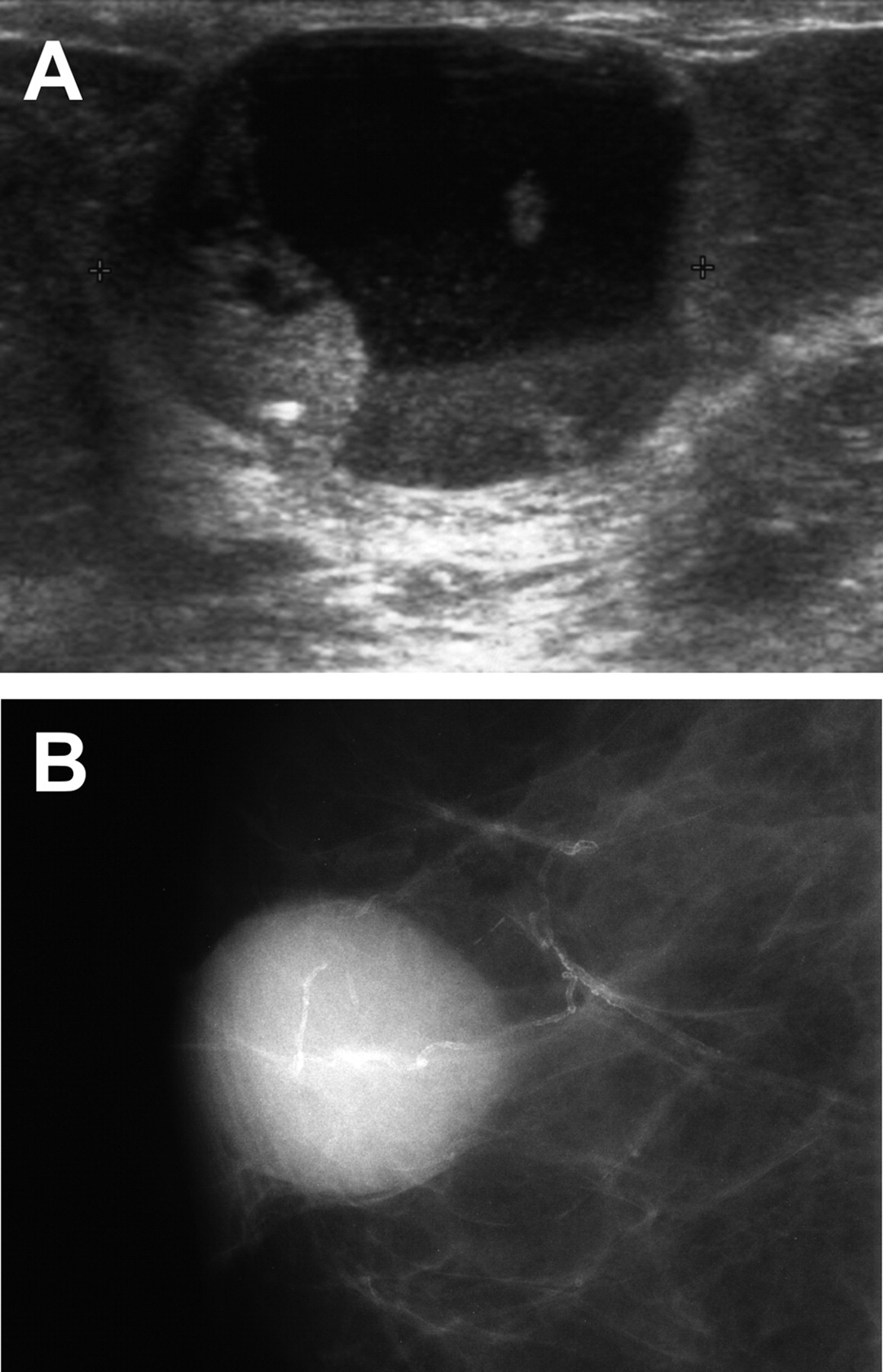
Ultrasonographic and mammographic findings of a palpable left breast tumor of a 77-year-old patient. (A) US scan shows a 0.7 × 1.1 × 1.2 cm circumscribed solid hypoechoic tumor with posterior acoustic accentuation (BI-RADS 3); (B) On the mammogram the tumor appears as a round BI-RADS 3 lesion. Final histology revealed mucinous carcinoma with small cancerous foci outside the tumor
Ultrasonographic and mammographic appearance of a pure mucinous carcinoma of a 72-year-old patient with a palpable right breast tumor. (A) US scan shows a 2.2 × 2.5 × 2.7 cm circumscribed tumor with mixed solid and cystic components (BI-RADS 4); (B) On the mammogram the tumor appears as a round, dense BI-RADS 3 lesion
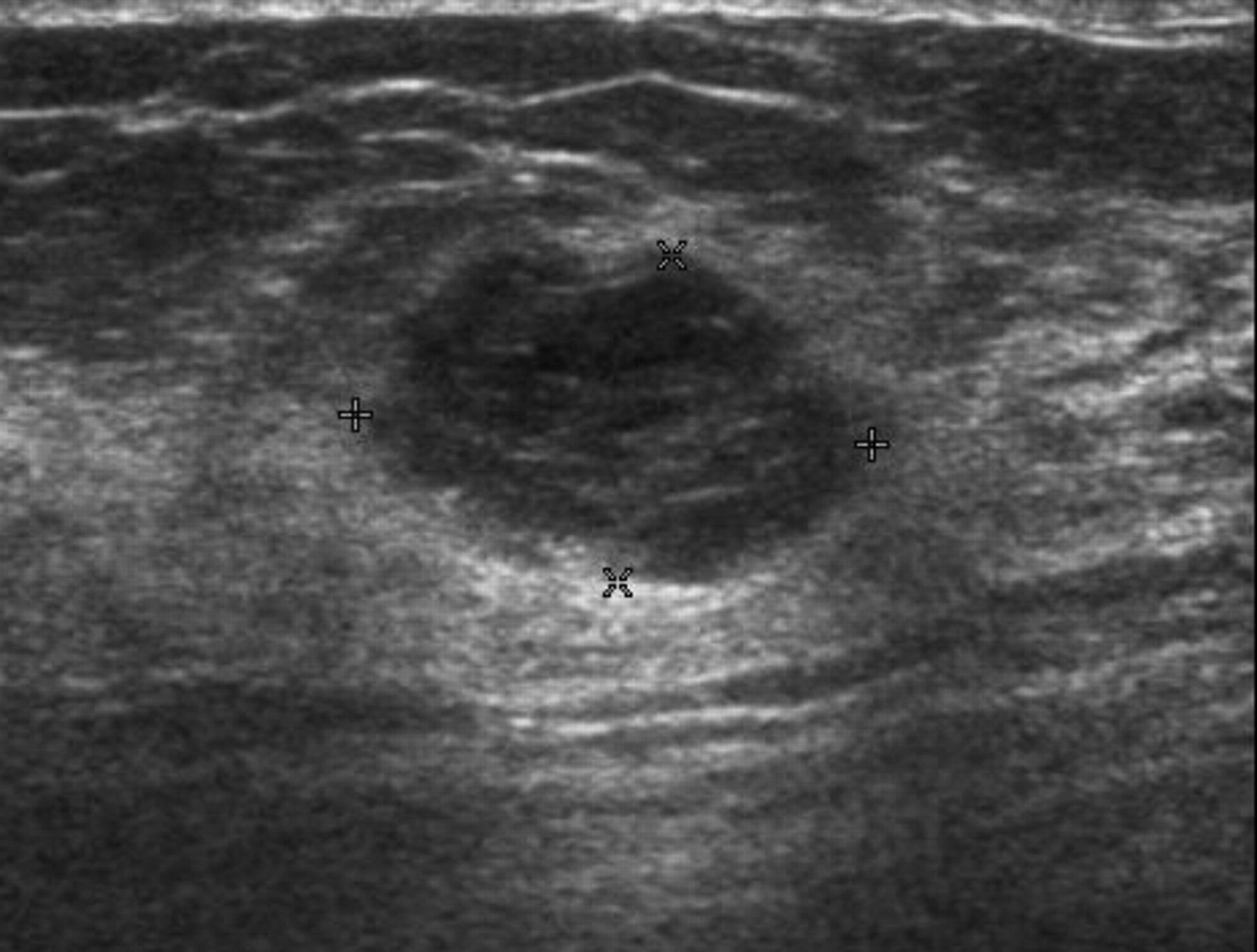
US image of a palpable left breast mucinous carcinoma of mixed type in a 56-year-old-patient. A lobulated hypoechoic heterogenous tumor with posterior acoustic accentuation (BI-RADS 4)

US image of a pure mucinous carcinoma of a 74-year-old patient with a palpable left breast tumor. A solid, slightly lobulated heterogenous, mostly hyperechoic tumor with posterior acoustic accentuation (BI-RADS 4)
Mammographic findings
All the 19 lesions with available mammograms had the appearance of a circumscribed mass (Figs. 1B and 2B), except for one architectural distortion (Fig. 5, classified as irregular on Table 2). Sixty-three percent (12/19) were high-density lesions, and 68% (13/19) had lobulated or indistinct margins (Table 2). Only one lesion in group 2 and two lesions in group 3 contained calcifications.

Left magnified mammogram of a 62-year-old patient with a normal finding on palpation reveals an irregular, BI-RADS 4 tumor (arrow) also containing calcification. Histologic diagnosis: mixed mucinous carcinoma
Seventy-eight percent of the pure mucinous carcinomas (7/9) were classified as BI-RADS 4 and the remaining two as BI-RADS 3 lesions. Two of the three mixed mucinous carcinomas with mammograms available for review were classified as BI-RADS 4 lesions, as were four of the seven (57%) mucinous carcinomas in group 3. The rest of the lesions had a BI-RADS 3 appearance (Figs. 1B and 2B). None of the tumors were classified as BI-RADS 1, 2, or 5.
Histologic findings
All 25 CNBs showed mucinous carcinoma, and the diagnoses were confirmed on therapeutic surgery, indicating a positive predictive value and sensitivity of 100% in this selected material.
Discussion
Diagnosis of mucinous carcinoma is reported to be delayed in as much as 38% of cases due to a mammographically benign appearance (8). Mammographic features – low density, oval or round shape, and circumscribed or slightly lobulated margins – may make these tumors difficult to differentiate from benign lesions such as cysts or fibroadenomas (16). Mucin can comprise over 90% of the total volume of mucinous carcinomas. Mixed-type lesions consist of a non-mucinous carcinoma with a component of mucinous carcinoma, where the first-mentioned component clearly defines the behavior of the tumor (1, 3). An association between poorly differentiated margins on mammograms and a decreasing volume of mucin has previously been suggested by Conant et al. (10), which was later supported by the finding of more irregular margins in mixed-type mucinous carcinoma in comparison with pure ones and a correlation of poorly-defined margins with histologic grade (2, 7, 9, 17).
Previous articles have reported sonographic appearances of mucinous carcinoma in a relatively small patient series. In a study of 34 pure mucinous carcinomas, 76% of the tumors appeared as well-circumscribed masses with lobulated margins (8). In some other studies, the portion of poorly-defined margins has in general been higher even in pure-type lesions (2, 7, 11, 18), whereas results corresponding to Dhillon et al. (8) have also been reported (9, 17). In the current study, all three types (circumscribed, lobulated, and irregular) of margins were seen among pure mucinous carcinomas and among those with ductal carcinoma outside the mucinous tumor, whereas none of the four mixed mucinous carcinomas had circumscribed margins.
All except two of the 24 mucinous carcinomas visible on sonographic images in the present study were seen as a solid mass. This is in accordance with most of the previously published series. Lam et al. (9) report a higher, >30% proportion of mixed cystic and solid lesions. The internal echogenicity of pure mucinous and group 3 carcinomas was found to be variable. Fifty-seven percent (67%) were hypoechoic, while 43% (33%) were iso- or hyperechogenic in relation to fat. All the mixed-type (group 2) lesions were hypoechoic. Similarly to our results Memis et al. (7), reported all eight mixed-type lesions hypoechoic, while nine of the 19 pure mucinous carcinomas were hypoechoic, and the rest were isoechoic. In the paper by Lam et al. (9), only two out of 19 pure tumors and none of 13 mixed tumors were hypoechoic on sonographic images. Their results differ from most previous studies, in which 86–100% of mucinous carcinomas are reportedly hypoechoic (8, 10, 11). The homogeneity of the internal echotexture of mucinous cancers is described in only a few previous papers. Lam et al. (9) found 57% (8/14) of solid pure mucinous carcinomas and all six solid mixed mucinous carcinomas heterogeneous. In the study by Chopra et al. (11), all except one out of seven cancers were heterogeneous. The results of the current study are very comparable to these: 86% of the solid lesions seen on sonographic images were heterogeneous.
In the present study, 79% of the pure mucinous carcinomas presented with posterior acoustic enhancement, and of the whole material, only one mixed carcinoma appeared with acoustic attenuation. Accentuation was documented more frequently than in previous studies, which report acoustic enhancement in 38–70% of mucinous carcinomas (7, 9–11). In a study by Memis et al. (7), 57% of pure mucinous carcinomas (11 out of 19 cases) showed acoustic enhancement and shadowing was only seen in two cases, whereas half (four out of eight cases) of mixed mucinous carcinomas presented with marked shadowing and enhancement was seen in only one lesion. Conant et al. (10) reported an even higher degree of shadowing (five out of eight cases with seven pure-type lesions), and no correlation with mucin content was found. In the study by Lam et al. (9), none of the tumors with less than 40% mucin content showed acoustic enhancement.
The delay in diagnosis reported by Dhillon et al. (8) was due to difficulty in differentiating mucinous cancers from benign circumscribed lesions on mammograms. Problems in recognizing these tumors relate partly to the rare occurrence of calcifications (7, 9, 18). Calcifications were seen in only three tumors in the current study. Nevertheless, most of the tumors were classified as BI-RADS 4 lesions and none were classified as BI-RADS 1 and 2 in the retrospective image analysis. All the lesions with images available were visible on mammograms, as compared with the study by Lam et al. (9), where as many as 21% of the mucinous carcinomas could not be detected by mammography. Five of the seven mammography-negative tumors in their study were non-palpable, and the size range was 0.9–2 cm, which is somewhat smaller than the size of the lesions in the present study.
Only one of the 25 lesions in the current study was not detected by sonography. This was probably due to abundant fatty tissue, which made the small non-palpable lesion indistinguishable in this particular case. In the paper by Dhillon et al. (8), 39% of lesions could not be detected sonographically. This difference is explained by different study materials. The current study dealt with selected material from a referral clinic, and 76% of the lesions were palpable, while 68% of the cancers in the screening study by Dhillon et al. (8) were non-palpable. Our result is very comparable to the paper by Lam et al. (9), who report 32 out of 33 lesions (85% of which were palpable) US positive.
Diagnosis of a mucinous breast lesion can be challenging, not only for the radiologist, but also for the pathologist (12), depending on the sampling technique. In a series of 37 mucinous carcinomas (13), fine needle aspiration achieved 56% sensitivity, whereas core biopsy reached 100% sensitivity and accuracy. In another study with 15 mucinous breast lesions – eight benign and seven malignant – the diagnosis at core biopsy remained the same at excision (14). Identical results were also reported in a series of 32 mucinous lesions with 21 carcinomas, which led the authors to conclude that every mucinous lesion detected by CNB does not necessitate excision (15). A more cautious approach has also been suggested (14) for reasons like the possibility of only sampling the mucin in a mucinous carcinoma, and the fact that benign mucinous lesions might be precursors of mucinous carcinoma (19). The risk of a false-negative core biopsy result can be minimized by extensive sampling. In the present study, two or three samples were obtained in most cases, and there were no false-negative CNB results. Most tumors were palpable and were biopsied under sonographic guidance, which at least partly explains the high accuracy. One should acknowledge that the results are biased due to study design, which excludes those patients who were not operated on after a benign core biopsy result.
Lesions examined with only fine needle aspiration and not core biopsy were excluded from this material. The core needle has replaced the fine needle in diagnosing breast tumors. Yet there still are some indications for using fine needle aspiration. In our clinic the technique is used to further investigate atypical or complex cystic lesions. If fluid obtained from a circumscribed cyst-like lesion appears mucous, it is important to subject it to cytologic analysis and to perform a repeat needle biopsy, if needed, in order not to miss a diagnosis of mucinous carcinoma.
The future may provide more tools for diagnosing mucinous carcinoma. Recently, the MRI features of mucinous carcinoma have been studied (20), and especially diffusion-weighted imaging has shown promise in differentiating mucinous carcinoma from other breast tumors (21).
In conclusion, most mucinous breast cancers were seen as a high-density circumscribed lesion on mammography and as a solid mass on sonographic images. On sonography, all mixed-type lesions were hypoechoic and had irregular or lobulated margins, while the internal echogenicity and margins of pure mucinous carcinomas and the mucinous carcinomas with cancerous cells outside the tumor were more variable. The presence of posterior acoustic enhancement – not a typical feature of invasive ductal carcinoma – should raise suspicion of mucinous carcinoma. Most of the tumors appeared as BI-RADS 4 lesions in US and mammography thus making both a useful tool for raising a suspicion of malignancy in mucinous cancers. CNB was found to be a highly reliable diagnostic tool for diagnosing mucinous carcinoma in this selected material.
Footnotes
ACKNOWLEDGEMENT
The authors would like to thank Meeri Apaja-Sarkkinen, MD, PhD (Department of Pathology, Oulu University Hospital), for her critical review of this manuscript and her valuable advice concerning pathology reports.