
Abstract
Background
Management of suspicious microcalcifications in very thin breasts is problematic.
Purpose
To evaluate whether sonographically-guided vacuum-assisted biopsy (USVAB) with digital mammography-guided skin marking (DM) for the diagnosis of breast microcalcifications is comparable to stereotactic-guided vacuum-assisted biopsy (SVAB) in Asian women with thin breasts.
Material and Methods
Retrospective review was performed for 263 consecutive suspicious microcalcification lesions in 261 women who underwent USVAB with DM or SVAB using a prone table between January 2004 and December 2007. SVAB was performed for 190 lesions and USVAB for 73 lesions. Biopsy results were correlated with surgical pathology or followed up for at least 12 months. The diagnostic outcomes of SVAB and USVAB to diagnose microcalcifications were compared.
Results
Of 263 lesions, 104 (40%) underwent surgery and 159 (60%) were followed up. SVAB and USVAB groups showed similar final categories or the extent of microcalcifications. US visible lesions were 57 (78%) of 73 at USVAB and 14 (10%) of 140 at SVAB. Of 57 US visible lesions at USVAB, 29 (51%) were not found in initial US but were detectable with the help of DM. Specimen radiographs were negative in 2.1% of lesions at SVAB and in 4.1% at USVAB (p = 0.4008). The under-estimation rate and false-negative rate were similar in SVAB and USVAB.
Conclusion
US with DM facilitates US visibility of microcalcifications. USVAB with DM can produce acceptable biopsy results, as can SVAB, to diagnose breast microcalcifications in patients with thin breasts.
Vacuum-assisted biopsy is a diagnostic tool used under stereotactic or ultrasound (US) guidance. Stereotactic guided vacuum-assisted biopsy (SVAB) is a technique for the diagnosis of non-palpable breast lesions discovered by mammography, especially suspicious microcalcifications not seen on US. However, SVAB has several limitations, including being uncomfortable for the patient, compressed too thinly to allow for successful biopsy of a lesion, exposure to ionizing radiation, and expensive and not universally available (1–3).
US-guided vacuum-assisted biopsy (USVAB) is a useful tool in diagnosis and interventional procedures of breast masses. USVAB has several advantages, which include improved patient comfort, real-time visualization of needle placement, no radiation exposure, shorter duration of the procedure, and relatively low cost (4). Although USVAB is limited in detecting mammographic microcalcifications without a mass (23–97% detection rates), USVAB can be efficient under some conditions (5–7). For example, for lesions in thin breast tissue, too close to the chest wall or in the breast tissue of the axillary tail, USVAB could be more efficient than SVAB. Therefore, it may be useful in Asian women, where thin breast tissues are common.
USVAB with digital mammography-guided skin marking may be useful for diagnosing suspicious microcalcifications when SVAB is unavailable or unsuccessful (7). However, there are few reports on the outcomes of USVAB and SVAB in a single institution.
Therefore, we evaluated whether sonographically-guided vacuum-assisted biopsy (USVAB) with digital mammography-guided skin marking (DM) for the diagnosis of breast microcalcifications is comparable to stereotactic-guided vacuum-assisted biopsy (SVAB) in Asian women with thin breasts.
Material and Methods
This study had institutional review board approval, and a patient informed consent requirement was waived because it was a retrospective study.
Patients
A retrospective review was performed of 315 consecutive breast microcalcification lesions classified as BI-RADS category 3, 4, and 5 in 308 consecutive women who underwent percutaneous USVAB (n = 87) or SVAB (n = 228) between January 2004 and December 2007. BI-RADS category 3 lesions were biopsied owing to cases referred from other hospitals or request of physicians. We excluded 47 lesions from patients who did not receive follow-up for at least 12 months nor underwent further pathological confirmation of the lesions in our institution. Five lesions underwent a biopsy twice for the same site (two cases, two times SVAB; three cases, both SVAB and USVAB). Only the first attempt for each lesion was retained for analysis. Finally, we included 263 lesions from 261 patients (age range 29–80 years; mean age 44.9 years). Of these patients, two underwent VABs of two separate lesions. All patients had no palpable lesions.
Imaging evaluation
All cases underwent mammography with dedicated equipment (Senographe 2000D, GE Healthcare, Buc, France). Standard craniocaudal and mediolateral oblique views were routinely obtained and additional spot compression magnification images for areas of microcalcifications were obtained as needed. Medical records and imaging reports were retrospectively reviewed. The mammographic features of SVAB and USVAB groups were compared on the basis of the extent, the number of microcalcifications per group, the distribution of microcalcifications, and Breast Imaging Reporting and Data System (BI-RADS) final assessment category (8). The extent of microcalcifications was measured as the greatest diameter of the group in either craniocaudal or mediolateral oblique views and categorized as smaller than 1 cm, 1–2 cm, or larger than 2 cm. The number of microcalcifications was assessed on magnification images and categorized as fewer than 10 microcalcifications, 10–50, or more than 50. The distribution of microcalcifications was classified according to BI-RADS descriptors: clustered, regional, linear, or segmental. The thickness of the compressed breast was recorded from mammograms.
Ultrasonography was performed using high-resolution ultrasonography equipment (IU22, Phillips Medical Systems, Bothell, WA; HDI 5000, Advanced Technology Laboratories, Bothell, WA; or Logiq 700, General Electric, Milwaukee, WI, USA) with 5-12 MHz linear array transducers. Before biopsy, US was performed by a radiologist on bilateral whole breasts as well as the targeted area after referencing the location of the microcalcifications on mammography. According to sonographic reports, each lesion was classified into two groups after US with or without digital mammography-guided skin marking: those with microcalcifications identified on US (US visible microcalcifications) or those with no microcalcifications identified on US (US invisible microcalcifications).
Biopsy procedure and management
All biopsy procedures were performed by one of nine board-certified radiologists specialized in breast imaging, which consisted of experienced radiologists with fellowship training (n = 4) or an average of 10 years (range 5–15 years) of clinical experience (n = 5) in US and mammography interpretation. The radiologist that reviewed the mammography and performed US determined the biopsy method of choice. US images were available in 140 (74%) of 190 lesions that underwent SVAB. The choice of stereotactic or US guidance was based on lesion visibility, radiologist and patient preference, and equipment availability.
Stereotactic-guided vacuum-assisted biopsy was performed for 190 microcalcification lesions using a prone table (Stereoguide with digital spot mammography; Lorad, Danbury, CT, USA). For all SVAB, a vacuum-assisted biopsy device with an 11-gauge probe (Mammotome; Biopsys/Ethicon Endo-Surgery, Cincinnati, OH, USA) was used to sample the microcalcifications. In all lesions, biopsy was performed at one skin entry site with a standardized protocol. The planned protocol was to obtain a minimum of 12 VAB specimens by rotating the probe ‘around the clock’ in 2-hour (60°) increments.
Sonographically-guided vacuum-assisted biopsy was performed for 73 microcalcification areas that were confirmed by digital mammography-guided skin marking. For all USVAB, a vacuum-assisted biopsy device with 11-gauge probe (Mammotome; Biopsys/Ethicon Endo-Surgery, Cincinnati, OH, USA) was used. Before the biopsy, craniocaudal and lateromedial (or mediolateral) mammography (Senographe DS, General Electric Medical Systems, Buc, France) using an open paddle was performed over the microcalcifications found on mammography for skin marking (Fig. 1). A radiologist marked the expected location of the microcalcifications with an oil-based pen drawn on an orthogonal line defined by an optical localizer for two-dimensional localization in each view. A skin line drawn in the mediolateral or lateromedial view indicates the height of the lesion. Another skin line drawn in the craniocaudal view determines the mediolaterality of the lesion. Once the skin was marked, US examinations were performed focusing on the crossed site of two skin marking lines. The visibility of microcalcifications before and after skin marking was recorded. The lesion depth, subcutaneous fat arrangement, and parenchymal features on mammography correlated with those on US. The planned protocol for USVAB was to obtain a minimum of five VAB specimens per one session. For both SVAB and USVAB, at least five or more flecks of calcium or three or more cores containing calcium were considered to ensure adequate sampling of microcalcifications. We generally tried the same biopsy process up to three times with checking the specimen radiograph.
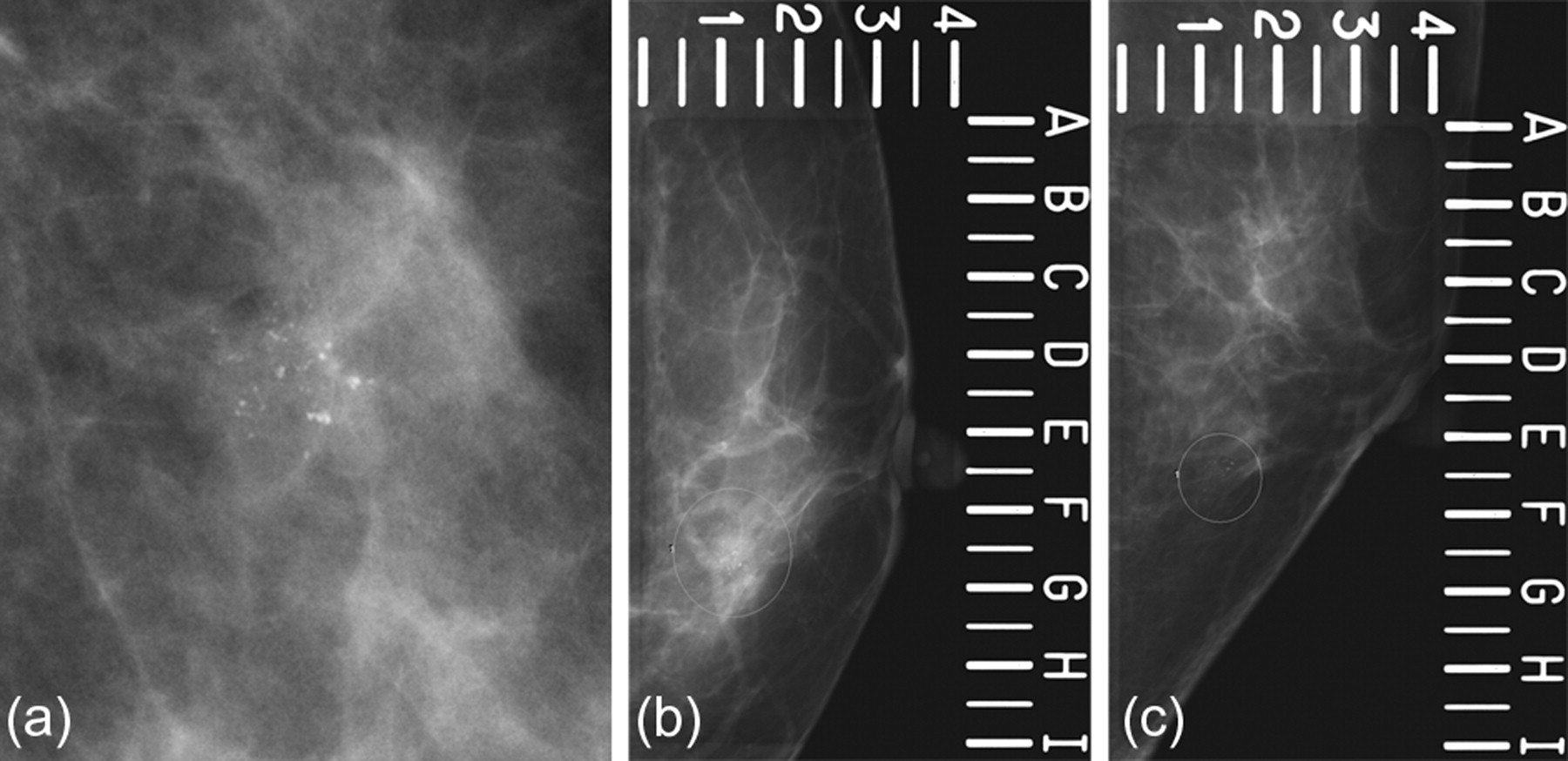
48-year-old woman with suspicious microcalcifications in left breast detected by screening mammography. The patient underwent a successful sonographically-guided vacuum-assisted biopsy after digital mammography-guided skin marking. Patient was diagnosed with ductal carcinoma in situ and underwent further wide excision, which revealed no residual tumor: (a) Magnified craniocaudal mammography shows 0.9 cm – extent of clustered amorphous microcalcifications; (b) and (c) Mammograms using an open paddle were taken for the skin marking before sonographically-guided vacuum-assisted biopsy; Microcalcifications (circle) are located in F.5 and 1 point on the craniocaudal view (b) and in E.5 and 1.3 point on the mediolateral view (c). Skin lines to mark the location of microcalcifications are determined in F.5 on the craniocaudal view and in E.5 on the mediolateral view
At our institution, patients with pathological results of malignant lesion, high-risk lesion, or benign lesion but suspicious (discordant) mammographic findings undergo surgery. Biopsy results were correlated with surgical pathology. Those with benign pathological results of concordant imaging findings are assigned to follow-up mammography at 6 months and then annually for at least 2 years. However, we only included patients with a follow-up of at least 12 months because of a relatively short follow-up period.
Specimen
After biopsy, specimen radiography was taken in every case to determine whether microcalcifications were retrieved. Retrieval failure was defined as no identification of microcalcifications on specimen radiographs. The number of core specimens was recorded: fewer than 7, 7–12, 13–24, 25–36, or more than 36. All of the specimens with and without microcalcifications were sent for pathological examination separately into two different bottles. The pathologists indicated in the reports whether microcalcifications were included or not on slides.
Data collection and analysis
The clinical, histological, and imaging findings were reviewed including the results from each biopsy and surgery, and follow-up imaging studies. The number, distribution, extent, and final category of microcalcifications on mammography were compared between SVAB and USVAB. The high-risk under-estimation rate was defined as the number of high-risk lesions upgraded to ductal carcinoma in situ (DCIS) or invasive cancer at surgical excision divided by all the high-risk lesions with surgical excision. The DCIS under-estimation rate was defined as the number of DCIS lesions upgraded to invasive cancer at surgical excision divided by all the DCIS lesions with surgical excision. The false-negative rate was defined as the number of false-negative cases divided by all the cancers. These rates were compared between the SVAB and USVAB groups.
We reviewed the specimen mammography and assessed the total number of specimen cores and the presence of microcalcifications in the specimen.
Statistical analysis
The retrieval failure rate, high-risk under-estimation rate, DCIS under-estimation rate, and false-negative rate of SVAB and USVAB for a diagnosis of suspicious breast microcalcifications were compared using Mann-Whitney test and Fisher's exact test. The performance of US with or without skin marking were compared using McNemar's test. Findings with p < 0.05 were considered statistically significant. Analyses were carried out using the SAS version 9.1.3 software (SAS Institute, Research Triangle Park, NC, USA).
Results
Of 263 microcalcification lesions, 104 (40%) lesions underwent surgery and 159 (60%) lesions were followed up for at least 12 months. Mean breast thickness of patients was 26 mm (range 10–49).
Mammographic findings
The extent, number, distribution, and BIRADS category of each microcalcification lesion are shown in Table 1. Both biopsy methods produced similar final assessments, extent, number, and distribution of microcalcifications (p = 0.2349, p = 0.5651, p = 0.1315, and p = 0.4126, respectively).
Mammographic features and biopsy method in 263 microcalcification lesions, n (%)
*Mann-Whitney test
**Fisher exact test
SVAB = stereotactic-guided vacuum-assisted biopsy, USVAB = sonographically-guided vacuum-assisted biopsy
Ultrasonographic findings
For 73 lesions, USVAB after digital mammography-guided skin marking was performed for 16 (21.9%) US invisible microcalcification lesions and 57 (78.1%) US visible lesions. Of 57 US visible lesions, 29 (51%) were not found in initial US but were detectable with DM (p < 0.0001). Calcifications were depicted as echogenic dots on US. US visible microcalcification lesions showed ill-defined hypoechoic lesions (n = 5), periductal thickening (n = 2), cystic lesions (n = 2), and architectural distortion (n = 1) that were associated with microcalcifications, or microcalcifications only (n = 47).
In 190 SVAB lesions, US was available in 140 (74%) cases. Fourteen (10.0%) lesions were US visible and the remaining 126 (90.0%) were US invisible. Fourteen lesions demonstrated subtle ill-defined hypoechoic lesions (n = 4), cystic lesions (n = 4), ductal ectasia (n = 2), and architectural distortion (n = 1). Three lesions showed only faint microcalcifications.
Specimen radiography
All lesions after a biopsy were checked by specimen radiography. The mean number of specimens obtained was 19.5 (range 6–45) in SVAB and 16.7 (range 6–41) in USVAB (p = 0.0798) (Table 1). Radiographs showed no calcification in 2.1% (4 of 190) lesions in SVAB and 4.1% (3 of 73) lesions in USVAB (p = 0.4008) (Table 2).
Correlation of VAB and follow-up results in seven lesions with negative specimen mammography
SF = stromal fibrosis, IDP = intraductal papilloma, FCC = fibrocystic change, DCIS = ductal carcinoma in situ, MIC = microinvasive ductal carcinoma, IDC = invasive ductal carcinoma
Biopsy results
Of the 190 lesions, the pathological results for SVAB were malignant in 42 (22.1%) lesions with invasive carcinoma in five and DCIS in 37, high-risk (ADH in seven cases and flat epithelial atypia in one case) in eight (4.2%), and benign in 140 (73.7%) (9, 10). At SVAB, DCIS was upgraded to invasive carcinoma in two, ADH to DCIS in one, and flat epithelial atypia to invasive carcinoma in one at surgical excision. The high-risk and DCIS under-estimation rate were 25% (2/8) and 5.4% (2/37) for SVAB, respectively. Seven benign histologies that were confirmed as malignancies at surgical excision showed four cases of stromal fibrosis, two cases of ductal hyperplasia, and a fibrocystic change at initial SVAB. These cases were surgically confirmed due to imaging-histology discordance. The false-negative rate of SVAB was 17.6% (9/51).
Of the 73 lesions, the pathological results for USVAB were malignant in 19 (26.1%) lesions, with invasive carcinoma in two and DCIS in 17, high-risk (ADH in all cases) in two (2.7%) and benign in 52 (71.2%). One (1.4%) case was underestimated at USVAB. ADH was upgraded to DCIS in one. The high-risk and DCIS under-estimation rate were 50% (1/2) and 0% (0/17) for USVAB, respectively. One of 52 benign lesions was initially diagnosed as a few atypical ducts with solid growth, but surgery of this lesion due to imaging-histology discordance confirmed it as invasive carcinoma. The false-negative rate of USVAB was 9.5% (2/21).
Diagnostic outcomes of SVAB and USVAB
There were no significant differences in the retrieval failure rates, high-risk lesion under-estimation rates, DCIS under-estimation rates, and false-negative rates for the diagnosis of suspicious microcalcifications between SVAB and USVAB (Table 3).
Diagnostic outcomes of SVAB and USVAB, % (n)
*Fisher exact test
Discussion
A stereotactic biopsy of suspicious microcalcifications is not performed for various technical reasons, especially for thin breasts in Korean women. A large fraction of this study population had thin breasts, with a mean breast thickness of 26 mm (range 10–49). Pathological confirmation of microcalcifications prior to surgery, therefore, requires another technique (11–13).
The yield rate of USVAB with digital mammography-guided skin marking is similar to that of SVAB to diagnose suspicious microcalcifications in our study. We were able to achieve acceptable outcomes for retrieval of microcalcifications by SVAB compared to previous studies, with 0–5% retrieval failure rates (14–17). In our study, 97.9% (186/190) of suspicious microcalcifications were successfully sampled by SVAB and 95.9% (70/73) by USVAB (p = 0.4008).
Although radiologists know about the mammographic location of microcalcifications, US-guided biopsy for a US invisible lesion without associated findings is limited. This study showed that digital mammography-guided skin marking is useful for US-guided biopsies of suspicious microcalcifications despite subtle associated findings. This procedure could narrow the targeted area during targeted US after the correlation with mammographic findings such as depth and distance from the nipple (18). In our study, skin marking enhanced the visibility of microcalcifications in 51% of US visible cases. However, USVAB with DM is not completely accurate for large and pendulous breasts, because of discrepancies between lesion location and the marked skin, the presence of peripherally located lesions, which may not allow two coordinate lines, or lesions deep in the middle of the breast because of the lack of landmarks. If microcalcifications are not documented on the initial specimen radiography, additional specimens can lead to the removal of an excessive amount of breast tissue.
USVAB may have several complications such as hematoma or infection (19). Compared with SVAB, there might be more bleeding because of the missing compression. Repeated insertion of the biopsy needle might also introduce a higher risk of infection. However, we did not observe any serious complications that required treatment or delayed discharge.
We found a lower DCIS under-estimation rate for microcalcifications, especially in USVAB (5.4% for SVAB and 0% for USVAB) than previous studies (1–20%) (1, 6, 18, 20). The vacuum-assisted device allows the radiologist to obtain samples more quickly, and requires less accuracy in the placement of the needle for retrieval because of suction from the adjacent areas. The vacuum-assisted device can also reduce the potential for sampling errors as well as under-estimation of the disease by the multi-pass techniques (13, 21, 22). Thus, USVAB can help prevent the under-estimation of DCIS in calcifications and retrieve invasive carcinoma manifesting as a subtle US lesion. An alternative explanation may relate to the nature of the disease itself in that DCIS frequently occur in scattered ducts rather than as a confluent area of abnormal cells (23). SVAB samples the tissue by rotating the probe within one hole, whereas USVAB can approach multidirectionally from a skin orifice.
Both groups showed similar mammographic extent of microcalcifications and under-estimation rates. Under-estimation of disease in cases diagnosed as DCIS at SVAB increased with increasing mammographic size of the biopsy target (24). However, we have found that USVAB is more effective for widely distributed mammographic lesions and trends toward fewer DCIS underestimation.
In our study, the prevalence of ADH, 4.2% at SVAB and 2.7 % at USVAB, was similar to previous studies, with 4–7% at SVAB (22, 25–31) and 0.4–2.5% at USVAB (1, 32–34). The rates of under-estimation of high-risk lesions at SVAB and USVAB in this study were 25% and 50%, respectively, consistent with previous reports (10–27% at VAB [22, 25, 26, 31, 35, 36] and 33.3–48% at USVAB [20, 37]). We had a lower under-estimation rate of DCIS but a similar under-estimation rate of ADH, potentially because of variation in pathologists' thresholds for diagnosing ADH and DCIS.
There are some limitations in this study. First, we have not used a localization clip during biopsy. However, we used needle localization or US-guided tattooing using a charcoal suspension if all calcifications were removed. Second, our study was designed as a retrospective study, and prospective studies with a large series are needed to demonstrate USVAB utility with or without DM. Third, we set a standard follow-up period of at least 1 year in this study population, which may be insufficient to diagnose a lesion with microcalcifications as benign. Fourth, breast US tends to be very operator-dependent, with reproducibility dependent on radiologist skill. Last, we did not analyze whether power Doppler US would be helpful to identify microcalcifications. Abnormal power Doppler vascularity may be useful in the detection and guidance of microcalcification biopsy (38).
In conclusion, US with digital mammography-guided skin marking facilitates US visibility of microcalcifications. USVAB with digital mammography-guided skin marking can produce acceptable biopsy results, as can SVAB, to diagnose breast microcalcifications in patients with thin breasts.