
Abstract
The purpose of this article is to review the imaging features of thoracic epithelioid hemangioendotheliomas with pathologic correlation. The thoracic manifestation of epithelioid hemangioendotheliomas is one of three different CT patterns: multiple pulmonary nodules, multiple pulmonary reticulonodular opacities, or diffuse infiltrative pleural thickening. Without any evidence of histological malignancy, malignant features (multiplicity of pulmonary nodules, hepatic or bone involvement, lymphangitic tumor spread, and infiltrative pleural masses) are characteristic of these infrequent tumors.
Pulmonary epithelioid hemangioendothelioma (EH) is a rare neoplasm of vascular origin with an epithelioid appearance, initially referred to as an intravascular bronchioloalveolar tumor (1). Being considered as a low- to intermediate-grade sarcoma, the tumor predominantly involves the liver and lungs, and rarely, bones, and can be aggressive and multicentric, even resulting in systemic metastases (1–5). Pulmonary EHs are four times more common in women than men and are often detected incidentally, as patients are usually asymptomatic (1, 4, 6). The tumors have variable prognosis; life expectancy may range from less than one year up to 30 years. There are no established standard treatment of choice (1, 4, 6). Surgery and/or chemoradiation therapy could be considered depending on intrathoracic tumor spread and systemic metastases (3).
There have been a limited number of sporadic case reports (4, 7–10) and one article (11) regarding the CT findings of thoracic EH. When we review and put together all these reports, there are three different patterns of CT findings of thoracic EHs: multiple pulmonary nodules (8, 10); multiple pulmonary reticulonodular opacities (4, 7, 8); and diffuse infiltrative pleural thickening (9, 11). This pictorial review will summarize these three distinctive CT patterns of thoracic EHs with pathologic correlation.
Three distinctive CT patterns of thoracic epithelioid hemangioendotheliomas
Multiple pulmonary nodules (mimicking hematogenous pulmonary metastases)
The most common feature of pulmonary EH on chest CT is the presence of multiple small discrete pulmonary nodules with well-defined margins in both lungs. The nodules range in size up to 2 cm, but most are less than 1 cm in diameter (Figs. 1–3) (1, 10). In a review of 20 cases, Dail et al. (1) showed that 20% of the patients had less than 10 nodules, 25% had more than 20 nodules, and the rest were somewhere in-between. This presentation of multiple small pulmonary nodules is easily mistaken for metastatic carcinoma, which is the initial radiologic interpretation in nearly all cases (7). However, little or no growth is shown on serial chest CT examinations (Figs. 2 and 3) (1, 4, 10). While histologic calcifications and ossification is common, radiologic visible calcifications are not (4).

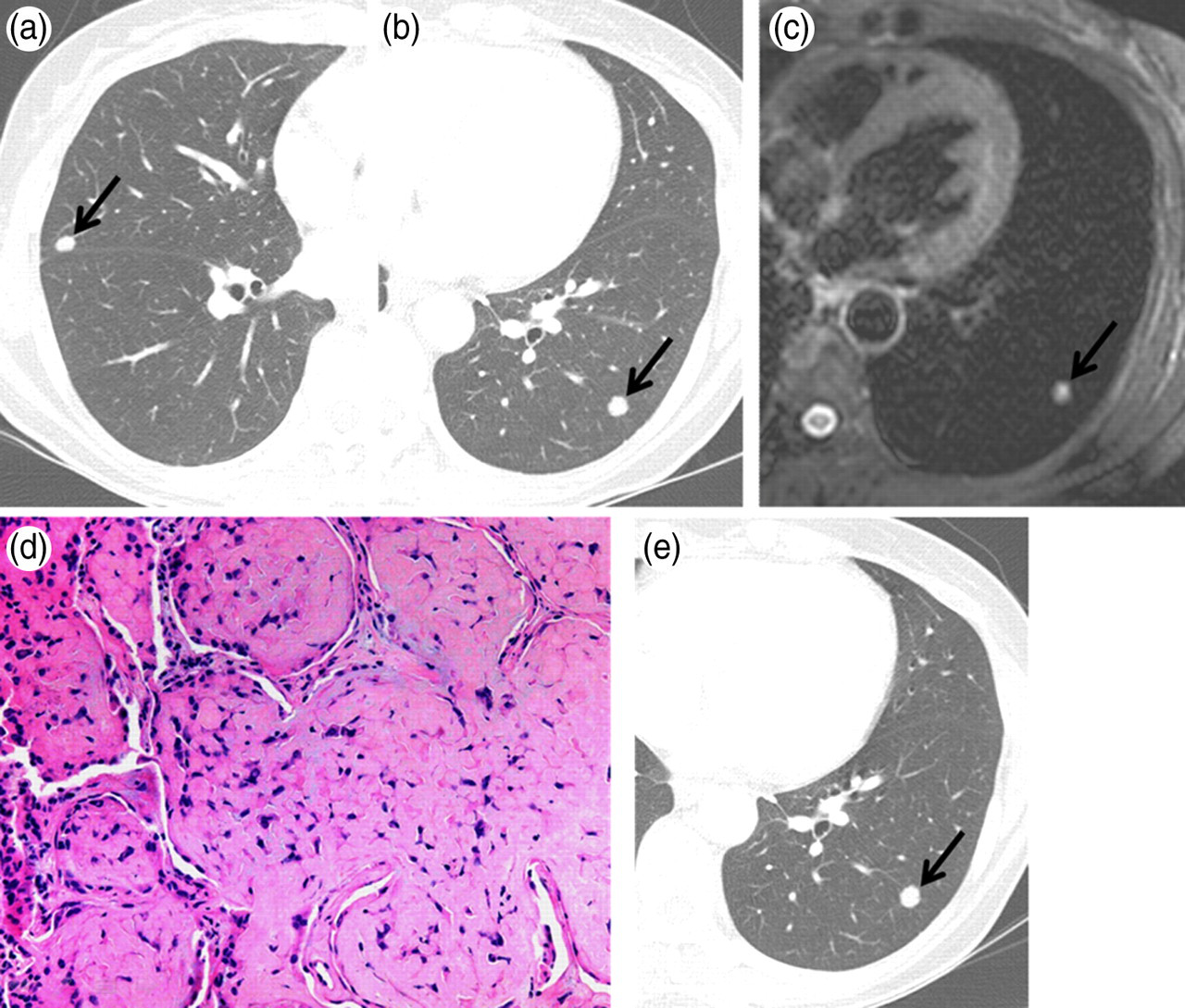
A 39-year-old woman with pulmonary epithelioid hemangioendotheliomas. (a, b) Chest CT images show two well-defined nodules (23 and 20 mm in longitudinal diameter, respectively) (arrows) in the left lower lobe; (c) PET shows mild FDG-uptake of the nodule (arrow) in the left lower lobe (the standardized uptake value was not available for measurement because her PET/CT had been performed at another hospital); (d) Photograph of the specimen obtained from wedge resection of the left lower lobe reveals a well-defined subpleural nodule, which typically has a central sclerotic, hypocellular zone and a cellular peripheral zone (H and E stain, ×1); (e) Photomicrograph of the nodule shows abundant eosinophilic stroma and tumor cells containing prominent cytoplasmic vacuoles or intracytoplasmic lumina (arrows) (H and E stain, ×200)
A 60-year-old woman with pulmonary epithelioid hemangioendotheliomas. (a, b) Chest CT images show well-defined, round, small (5 mm and 8 mm, respectively) nodules in the right middle and the left lower lobe, respectively (arrows); (c) T2-weighted MR image shows high signal intensity of the nodule (arrow) in the left lower lobe; (d) On high-power histological examination of the specimen obtained from wedge resection of the right middle lobe, the tumor cells typically spread into adjacent bronchioles and alveolar spaces in a micropolypoid manner. (H and E stain, ×200); (e) Follow-up CT obtained 17 months after the initial CT scan (b) shows minimal interval growth of the nodule (from 8–9 mm in diameter) in the left lower lobe (arrow)
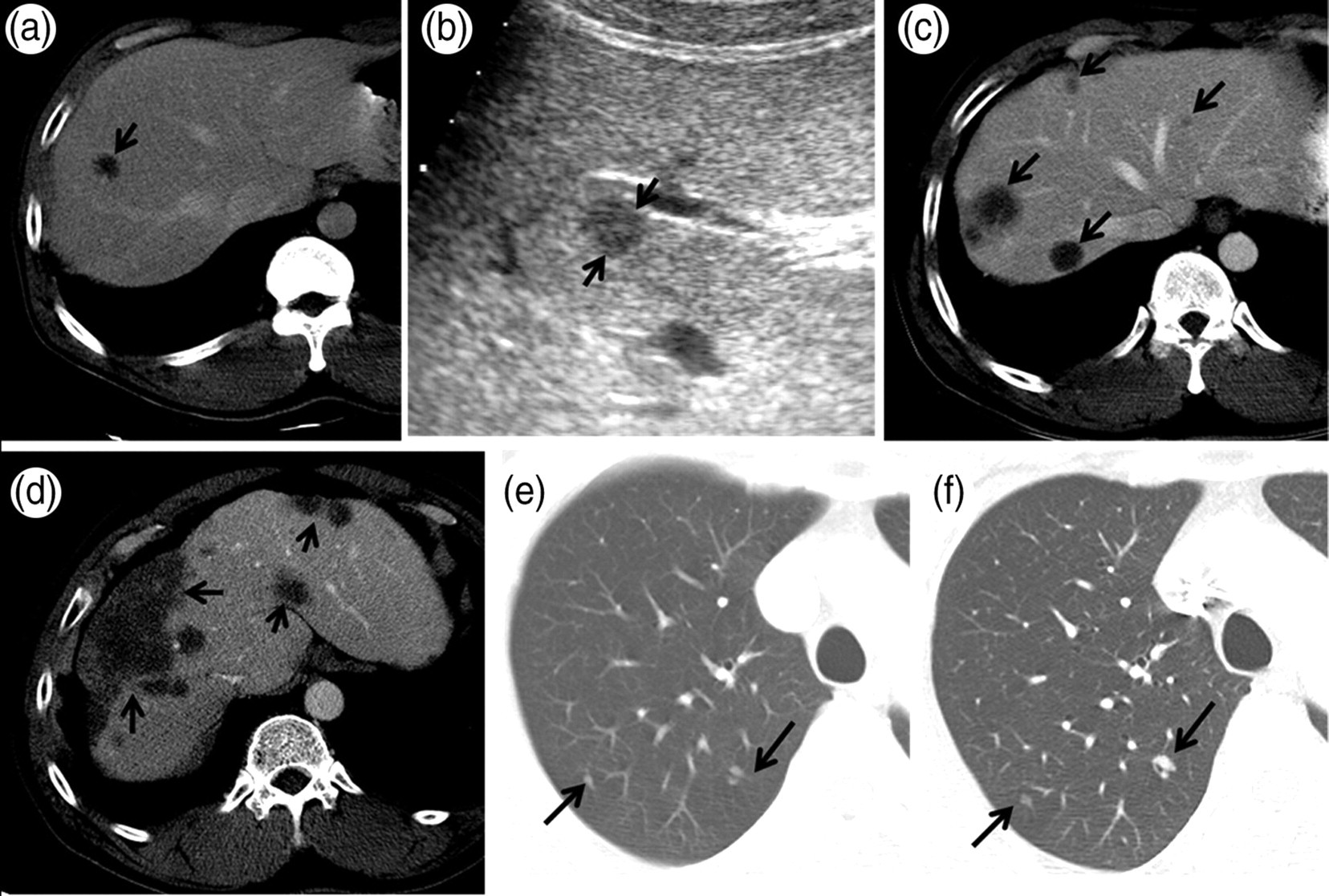
A 52-year-old man with hepatic and pulmonary epithelioid hemangioendotheliomas. (a) Initial abdomen CT of portal-venous phase shows a hypo-attenuated nodule (arrow) in the right hepatic lobe; (b) On ultrasonographic examination, the corresponding hepatic nodule shows hypo-echogenicity (arrows); (c) Follow-up CT obtained 19 months after the initial CT scan shows interval increase in size and number of the hepatic nodules (arrows); (d) Recent CT obtained 118 months after the initial CT scan shows the hepatic nodules have increased in size, coalesced and formed diffuse masses, mainly in the periphery of the liver (arrows). Compensatory hypertrophy of unaffected liver is also noted. In contrast, (e) initial and (f) follow-up chest CT scans show little or very slow interval growth of the pulmonary nodules in the right upper lobe during 66 months of period (arrows)
Epithelioid hemangioendotheliomas can affect multiple organs, and controversies exist regarding the multicentric or metastatic nature of EHs. Approximately 15–20% of patients with pulmonary EHs have hepatic involvement (1, 5, 12). In its early stage, hepatic EH is characterized by multiple, small, round peripheral nodules (Fig. 3). These nodules have low attenuation at contrast-enhanced CT, and most of the nodules are hypoechoic relative to adjacent hepatic parenchyma on ultrasonography (13). In the advanced stage, the nodules increase in size, coalesce and form diffuse large masses, which are mainly peripherally located and usually cause infiltration of hepatic vessels (Fig. 3d) (14, 15). On sonography, the liver may appear with diffuse heterogeneous echotexture in regions of diffuse extensive involvement (13, 16). Compensatory hypertrophy of unaffected hepatic segments or signs of portal hypertension can be seen (14, 15). Knowledge of these CT manifestations of hepatic EH may be helpful to narrow the differential diagnoses in patients having both pulmonary and hepatic nodules.
Multiple pulmonary reticulonodular opacities (mimicking hematolymphangitic pulmonary metastases)
Several case reports have described an atypical CT manifestation of pulmonary EHs with multiple small pulmonary reticulonodular opacities associated with interlobular septal thickening (4, 7, 8) and ground-glass opacities (4, 7) on high-resolution CT. This unusual CT pattern of pulmonary EH might mimic the appearances of hematolymphangitic metastases or diffuse interstitial lung diseases (Fig. 4). Histopathologically, these reticulonodular opacities and interlobular septal thickening are attributed to multiple, small, infiltrating nodular proliferation of neoplastic cells within the lumina of small blood vessels and lymphatic vessels (4, 7, 8). This growth pattern of pulmonary EH is known be related to a poor prognosis (1). Rarely, EH can involve bones with the classic radiographic appearance of multiple osteolytic lesions, which has the tendency to involve a single anatomic region or extremity (17, 18). Cortical destruction and cortical expansion are uncommon (17).
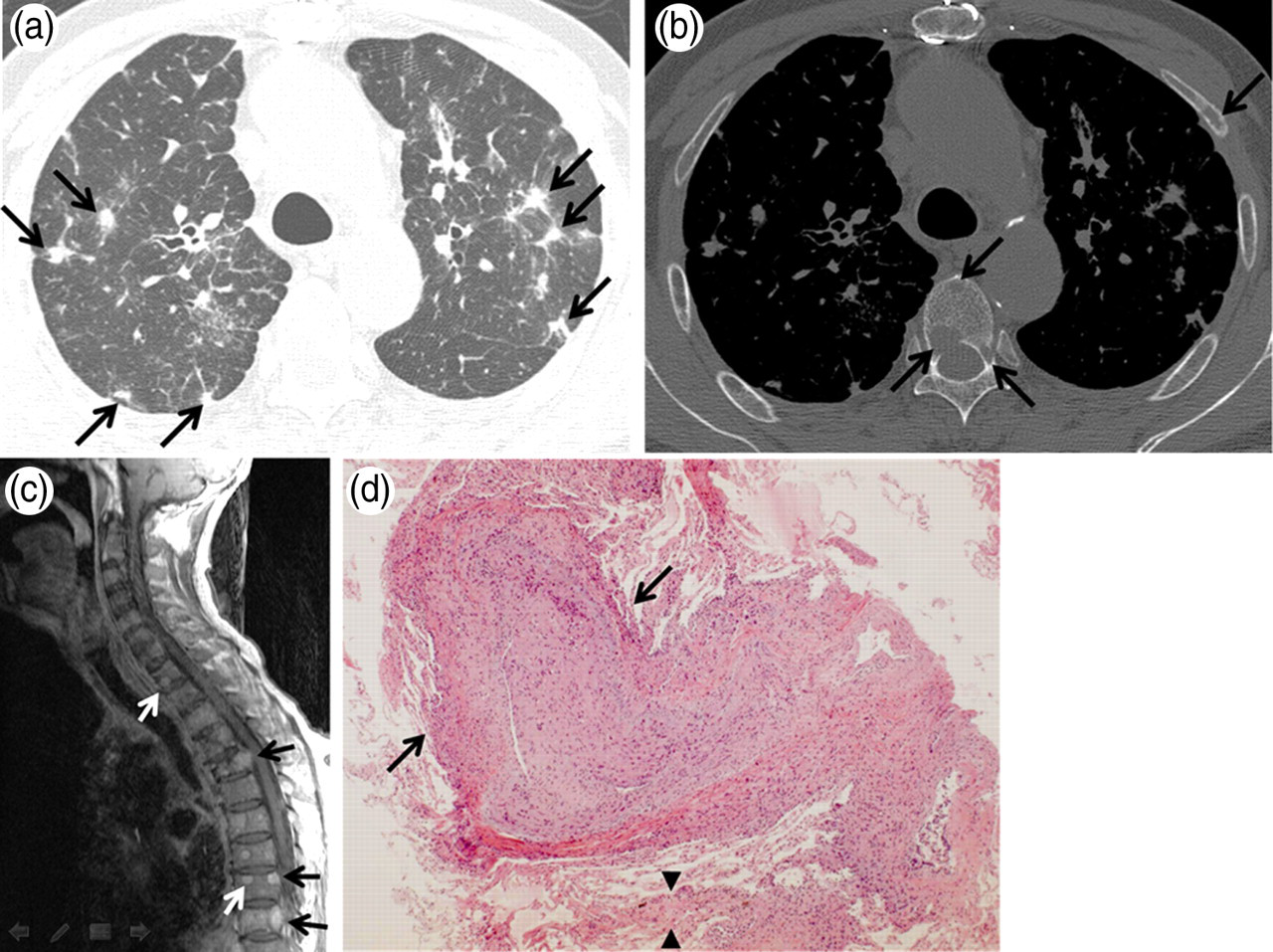
A 69-year-old man with pulmonary epithelioid hemangioendotheliomas. (a) Chest CT shows innumerable reticulonodular opacities scattered in both lungs. These poorly-defined nodules with irregular margin (arrows) are accompanied with interlobular septal thickening and patchy areas of ground-glass opacity; (b) Chest CT with bone window setting shows multiple osteolytic lesions (arrows) in the spine and ribs; (c) Gadolinium-enhanced, T1-weighted mid-sagittal MR image of the spine reveals multiple enhancing nodules involving thoracic spines (arrows); (d) Photomicrograph obtained from transbronchial lung biopsy demonstrates tumor cells packing the lumina of lymphatic vessels (arrows) along bronchovascular bundles. Also note thickening of interlobular septa by infiltration of tumor cells (arrowheads) (H and E stain, ×4)
Diffuse infiltrative pleural thickening (mimicking malignant pleural mesothelioma)
Pleural involvement of EH has been less frequently described, and this subtype typically affects older men who present with chest pain and dyspnea (9, 11). Pleural-based EH manifests as diffuse and nodular pleural thickening with pleural effusions on chest CT scans, and hence, it appears quite similar to malignant pleural mesothelioma or diffuse pleural carcinomatosis (Fig. 5) (9, 11). While pulmonary EHs have a relatively good prognosis, pleural-based EHs almost always have an aggressive clinical course (9, 11). Other poor prognostic factors of EH include presence of symptoms, hepatic metastases, peripheral lymphadenopathy, extensive intravascular or interstitial tumor spread, pleural effusion, fibrous pleuritis with extrapleural proliferation of tumor cells, and spindle tumor cells (1, 9, 19).
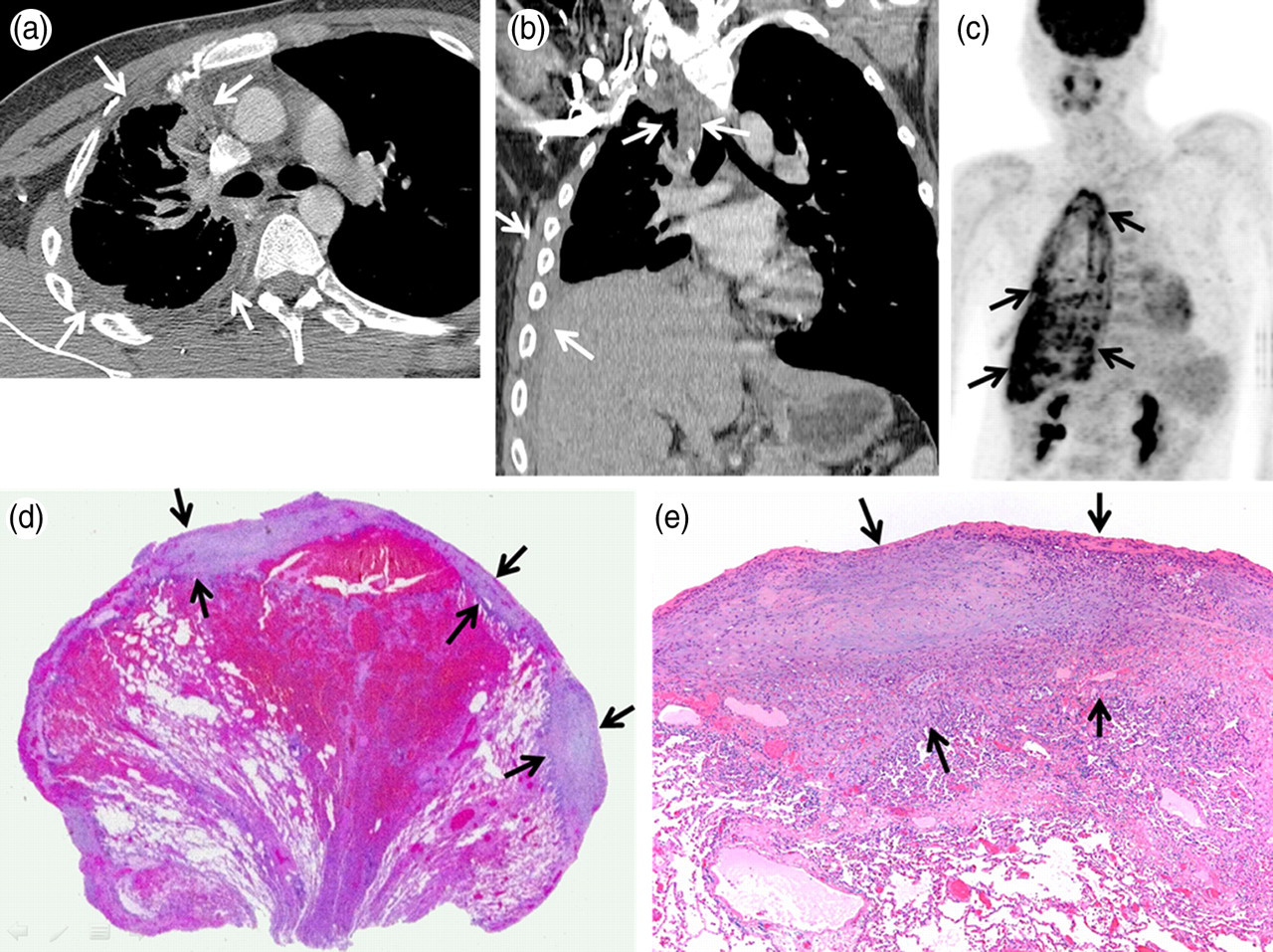
An 18-year-old man with pleural epithelioid hemangioendothelioma. (a) Axial and (b) coronal-reformatted chest CT images on mediastinal window setting show diffuse irregular infiltrative pleural thickening in the right hemithorax (arrows); (c) PET shows diffuse strong FDG-uptake of the infiltrative pleural thickening (arrows) in the right hemithorax (the standardized uptake value was approximately 7.0); (d) Photograph of the specimen obtained from pleural biopsy shows diffuse irregular thickening of the visceral pleura (arrows) (H and E stain, ×4); (e) Low-magnification view of the specimen reveals an infiltrative growth pattern of epithelioid tumor cells along the pleura (arrows) (H and E stain, ×40)
Role of PET or PET/CT
PET/CT findings have been reported for a few patients with thoracic EHs with variable increased FDG-uptakes (Figs. 1c and 5c) (20–22). Because 18-flurine-fluorodeoxyglucose (18F-FDG) is incorporated into rapidly growing, aggressive tumors, 18F-FDG-PET/CT would be valuable for patients with thoracic EHs in the evaluation of the metabolic activity of the multiple pulmonary nodules and in search for other foci of EHs throughout the body (22). The standardized uptake value (SUV) of EHs on 18F-FDG-PET/CT might also be used as an indicator for therapeutic decision-making. However, when deciding surgical resection of small EH nodules less than 2 cm in diameter, it should be considered that the measurement of the SUVs could be of a limited value because of the partial volume averaging effect, which is one of many factors affecting the SUV and would underestimate the real hypermetabolic activity of EH nodules (22, 23).
Histopathologic findings
The 2004 World Health Organization Classification of Tumors regards pulmonary EH as a low- to intermediate-grade vascular neoplasm (5). In contrast, malignant angiosarcomas are defined as the presence of increased mitotic activity (>1 mitosis per 10 high-power fields) or zones of spindling of cells, marked nuclear atypia, and necrosis. All of these features are known to correlate with poor clinical outcome (5, 9). In patients with systemic EHs, despite the aggressive biological behavior, there are no histological characteristics suggestive of angiosarcoma or a high-grade neoplasm. Low-power histologic examination reveals round to oval-shaped nodules, which usually have a central sclerotic, hypocellular zone and a peripheral cellular zone (Fig. 1d). Histologic characteristics of EHs include epithelioid cells with abundant eosinophilic cytoplasm, and intracytoplasmic vacuolization having a signet ring-like appearance (Fig. 1e) (1, 5). These tumor cells typically spread into adjacent bronchioles and alveolar spaces in a micropolypoid manner (Fig. 2d) (1, 5). Infiltrative nodular proliferation of tumor cells within the lumina of small arteries, veins and lymphatics might mimic hematolymphangitic metastases (Fig. 4d) (4, 7, 8). In addition, this kind of infiltrative growth pattern of epithelioid tumor cells along the pleura could mimic diffuse malignant pleural mesothelioma (Figs. 5d and 5e) (9, 11). Immunohistochemistry for EHs reveals that all tumors display immunoreactivity to some or all of the vascular-endothelial markers (CD31, CD34, and factor VIII) (24).
Conclusion
Thoracic EHs manifest as one of three discrete CT patterns: multiple pulmonary nodules; multiple pulmonary reticulonodular opacities; or diffuse infiltrative pleural thickening. Although EHs are not showing any evidence of histological malignancy as low- to intermediate-grade vascular neoplasms, malignant clinical features such as multiplicity of pulmonary nodules, hepatic or bone involvement, pulmonary lymphangitic tumor spread, and infiltrative pleural masses are characteristic of these infrequent tumors, awareness of which can be helpful in the diagnosis of thoracic EHs.