
Abstract
Creutzfeldt-Jakob disease is a rare and fatal neurodegenerative disorder with MR findings predominantly limited to the grey matter of the cortex and the basal ganglia. Sporadic Creutzfeldt-Jakob disease can produce a spectrum of MR imaging findings of the brain, most notably on DWI and FLAIR sequences. Involvement of the basal ganglia and neocortex is the most common finding, but isolated involvement of the cortex can also be seen. We describe the clinical history and MRI findings of three patients with sporadic Creutzfeldt-Jakob disease confirmed by brain biopsy or autopsy and review the literature of imaging manifestations of this disease.
Creutzfeldt-Jakob disease (CJD) (1, 2) is a rare and fatal neurodegenerative disorder characterized by neuronal loss, spongiform encephalitis and astrocytic gliosis predominantly limited to the grey matter of the cortex and the basal ganglia (3). CJD has an incidence of 1 per 1 million per year worldwide, affecting both men and women (3). In the USA, 200 people are affected with CJD per year (4). Several types of CJD are known: sporadic, the most common form; familial, which has a genetic predisposition; acquired, which develops after iatrogenic transmission; and variant, which is transmitted after ingesting infected cow meat. The infectious agent is a protein called a prion.
Clinically, patients present with rapidly progressing dementia, myoclonus, and impaired vision mimicking other neurodegenerative diseases. The disease progresses to akinetic mutism and death after approximately 1 year.
Currently no single diagnostic test is available, however, clinical presentation and additional testing help to narrow the differential diagnosis prior to biopsy or autopsy. The clinical history classically includes rapidly progressive dementia with myoclonus and ataxia. Electroencephalogram (EEG) will often reveal periodic sharp wave complexes at a frequency of 1–2 Hz. Lumbar puncture can be helpful to test for specific proteins in the cerebrospinal fluid (CSF), such as protein 14-3-3, neuron specific enolase, and tau protein. Direct tissue sampling revealing the pathognomonic spongiform transformation of the cerebral cortex and deep gray structures remains the only confirmatory test. Numerous studies have described increased T2 and FLAIR signal in the basal ganglia and thalamus, often combined with restricted diffusion in these locations. The combination of positive FLAIR and diffusion weighted imaging (DWI) has a high sensitivity and specificity for CJD. The imaging findings in combination with the clinical history, EEG, and CSF can often times provide sufficient supporting evidence of the diagnosis of CJD to avoid the risks associated with premortem biopsy.
The clinical history, hospital course, and MR imaging of three recent consecutive cases of sporadic CJD are examined. These three patients were admitted to the Neurology service at our institution between June 2006 and May 2009 with progressive neurologic impairment and underwent MR imaging of the brain. Autopsy or brain biopsy was performed on each patient, confirming the diagnosis of CJD.
Case reports
Case 1
A 70-year-old woman presented with a gradual decline in visual acuity, ataxic gait, and cognitive decline. Her initial physical examination was significant for a left hemianopsia and mildly decreased strength in the left upper extremity, as well as an ataxic gait. Normal serum blood levels and cerebrospinal fluid analysis were revealed. EEG was significant for triphasic waves. An MRI of the brain was performed (General Electric [GE] Signa 3T Excite HD; GE Healthcare, Milwaukee, WI, USA; 3.0 Tesla [T]), which included diffusion-weighted images (repetition time [TR] = 4200 ms; echo time [TE] = 99 ms; flip angle [FA] = 90; number of excitations [NEX] = 4) and a FLAIR sequence (TR = 9500 ms; TE = 121 ms; inversion time [TI] = 2500 ms; FA = 180). The predominant MRI finding included a ribbon-like hyperintensity on diffusion-weighted images with corresponding decreased apparent diffusion coefficient (ADC) values within the cortex of the occipital and parietal lobes (Figs. 1 a–c). The frontal lobes were not affected. The basal ganglia and thalamus demonstrated normal signal on FLAIR sequences (Fig. 1d). She was ultimately diagnosed by brain biopsy that revealed spongiform encephalopathy (Fig. 2), confirmed as CJD by immunostaining. After diagnosis, she had a continued cognitive decline and lost the ability to interact with surroundings. She ultimately passed away shortly thereafter. A diagnosis of the sporadic form of Creutzfeldt-Jakob disease was given based on imaging findings, clinical history, and absence of a family history of CJD.
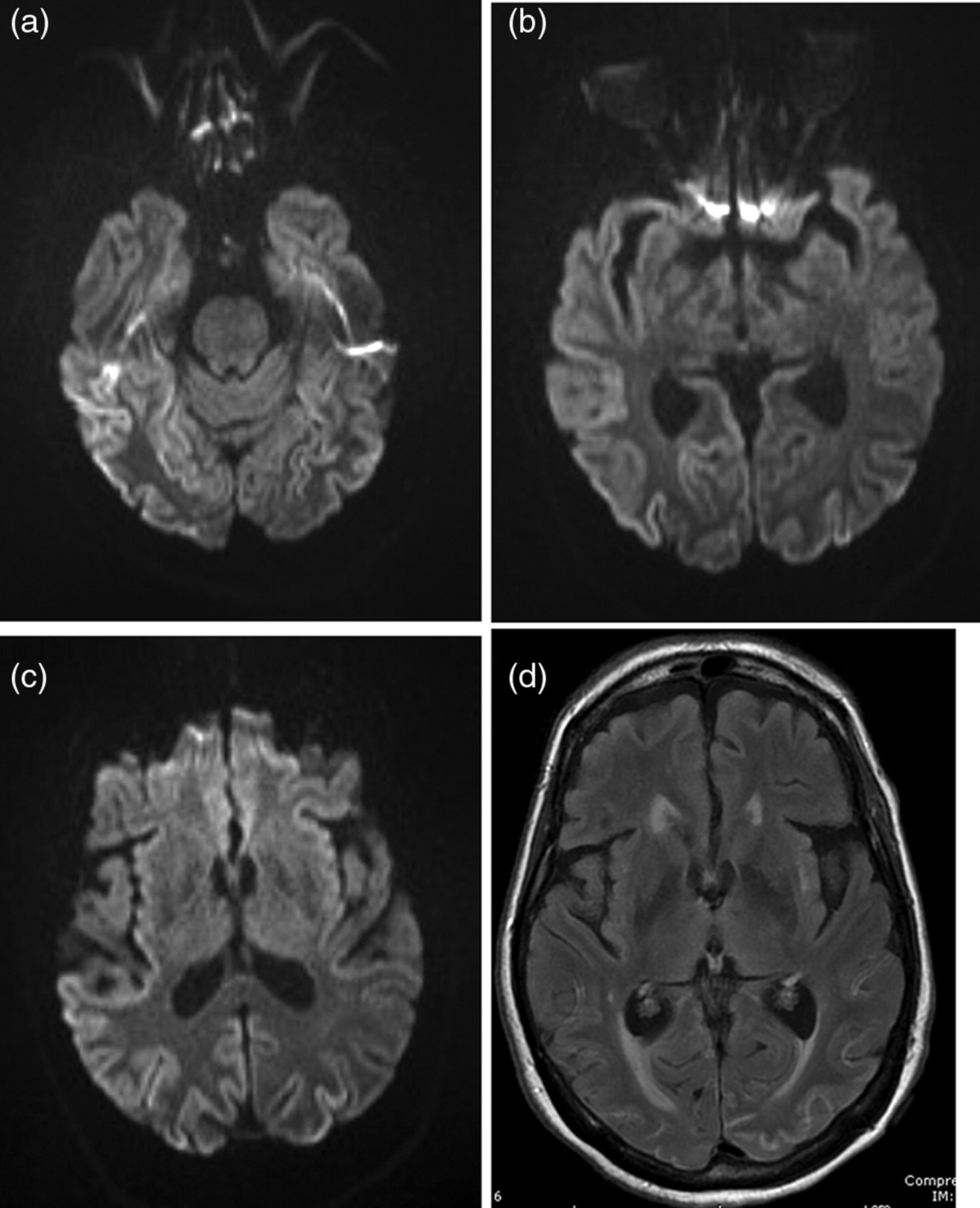
Sporadic Creutzfeldt-Jakob disease in a 70-year-old woman. (a–c) Diffusion-weighted images through the brain reveal restricted diffusion within the cortex of the parietal and occipital lobes bilaterally. There is no diffusion restriction within the basal ganglia; (d) The FLAIR image demonstrates a lack of hyperintense signal in the basal ganglia
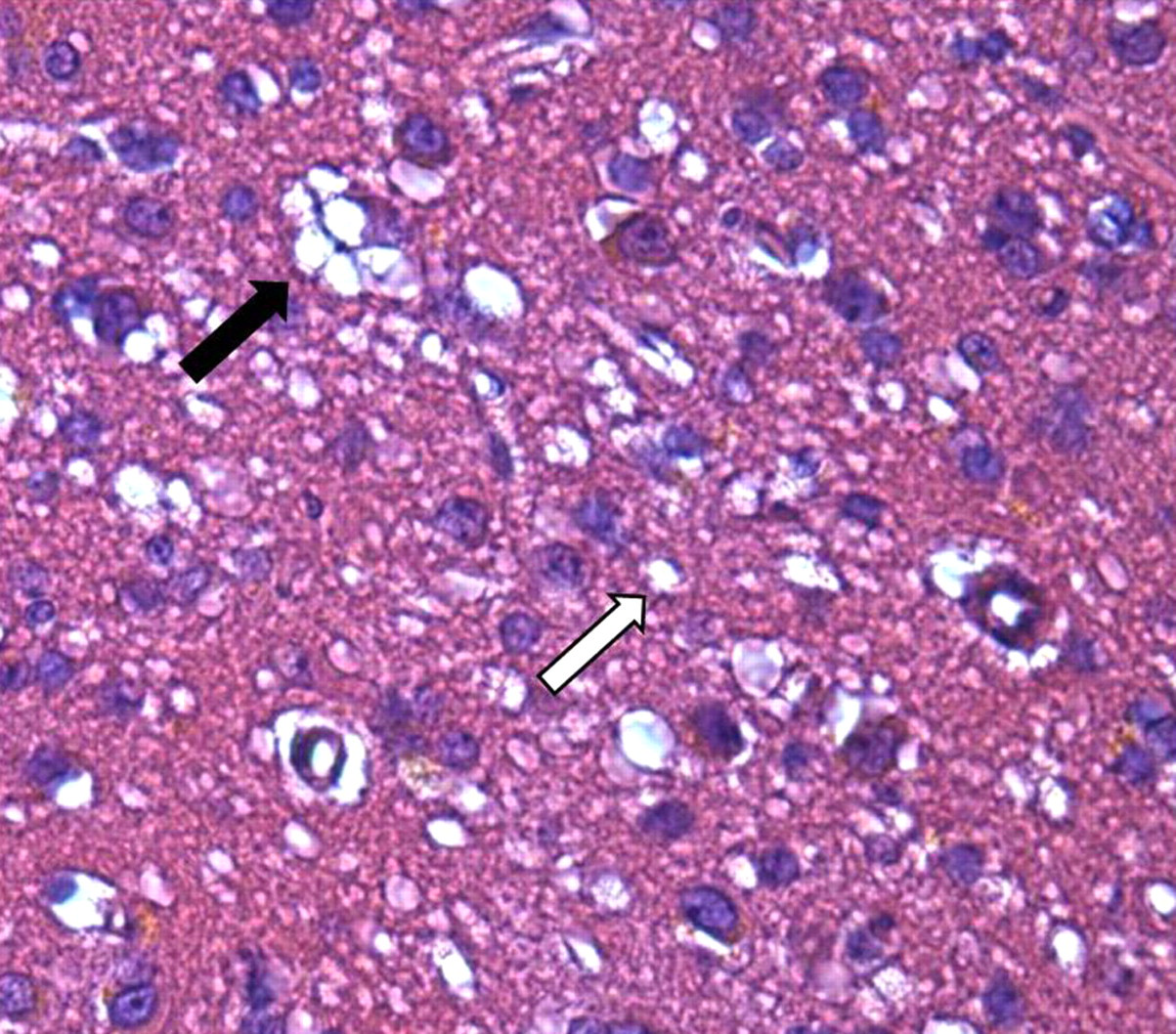
Sporadic Creutzfeldt-Jakob disease in a 70-year-old woman. Hematoxylin and eosin (HE) stain with 600x magnification demonstrating cytoplasmic vacuolization predominantly adjacent to the nucleus (black arrow) and additional vacuoles within neuritic processes (white arrow)
Case 2
A 52-year-old woman experienced a four-month gradual decline in cognition and change in sleeping pattern. She eventually lost the ability to feed herself and ambulate independently. Her neurological examination was significant for impaired cognition and aphasia, as well as frequent myoclonic jerks. Her serum and CSF evaluation was normal. EEG revealed 1 Hz generalized sharp waves. An MRI of the brain was subsequently performed (Siemens Espree; Siemens, Erlangen, Germany; 1.5 T), which included diffusion-weighted images (TR = 4500 ms; TE = 112 ms; NEX = 4; FA = 90), a FLAIR sequence (TR = 8000 ms; TE = 123 ms; TI = 2500 ms; FA = 180) and T2-weighted images (TR = 4790; TE = 90; NEX = 2; FA = 150). The MRI showed asymmetric restricted diffusion within the cortex of the frontal, parietal and occipital lobes, with the right hemisphere affected more than the left (Figs. 3 a–d). The basal ganglia were affected asymmetrically, with the right caudate nucleus and putamen demonstrating hyperintensity on FLAIR and T2-weighted images (Figs. 3e and f) and restricted diffusion (Figs. 3a and c). The striatum on the left demonstrated normal signal on all sequences. Following her initial presentation, she had near continuous generalized myoclonus and lost her ability to communicate and feed. She ultimately died approximately one month after presentation. Autopsy examination, including brain tissue sample analysis at the National Prion Disease Pathology Surveillance Center (NPDPSC) (Department of Neuropathology, Case Western Reserve University, Cleveland, OH, USA), confirmed the diagnosis of the sporadic form of Creutzfeldt-Jakob disease.
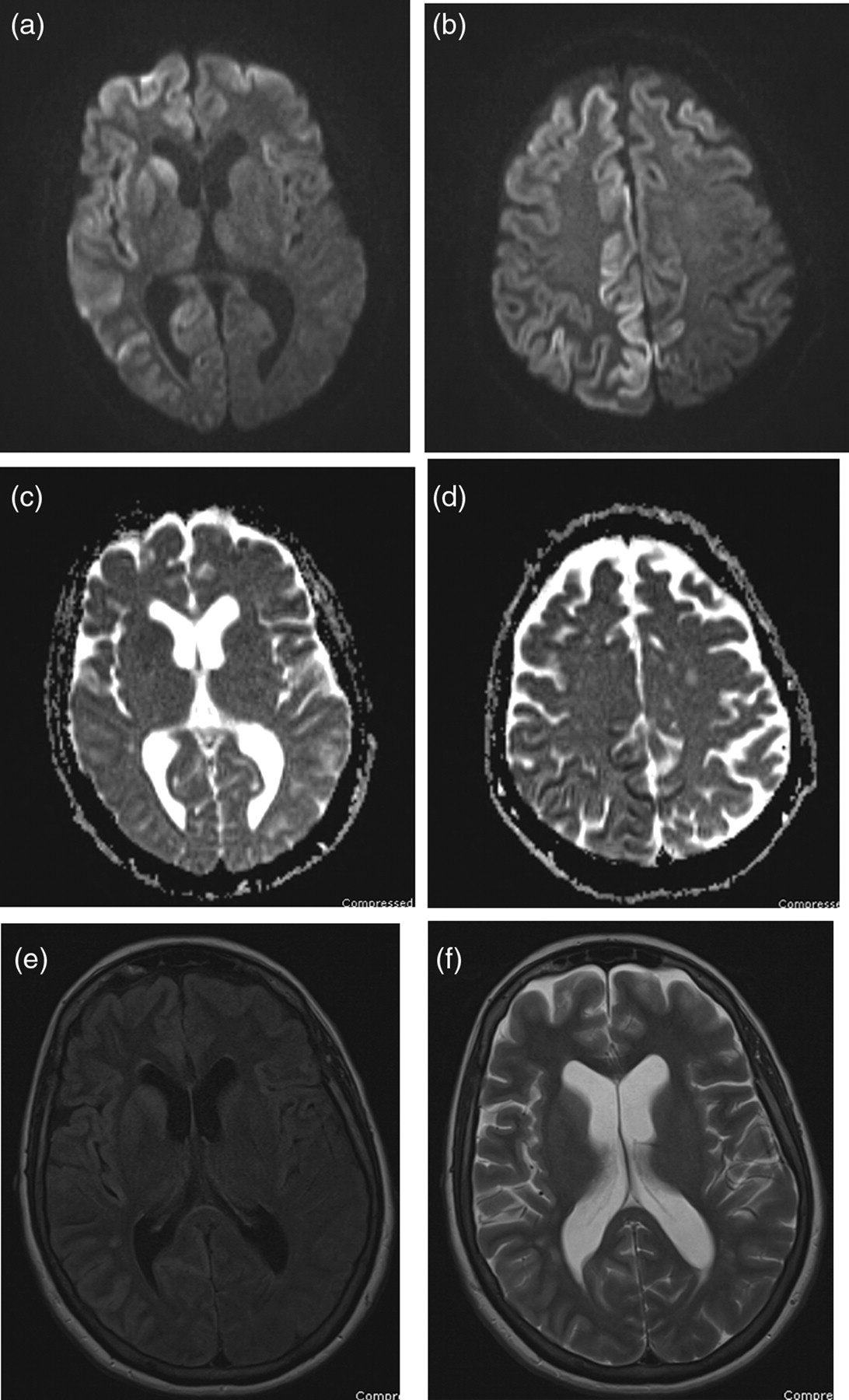
Sporadic Creutzfeldt-Jakob disease in a 52-year-old woman. (a, b) Diffusion-weighted images and (c, d) their corresponding ADC maps through the brain show asymmetric restricted diffusion in a cortical distribution within the frontal, parietal, and occipital lobes; (e) The FLAIR and (f) T2-weighted images demonstrate mild hyperintense signal within the cortex of the right temporal and frontal lobes. Restricted diffusion and FLAIR hyperintensity affect the basal ganglia asymmetrically, with involvement of the right caudate nucleus and the anterior right putamen
Case 3
A 58-year-old man presented with a history of progressive dementia over an eight-month period with incoordination and frequent falls. His neurological examination was significant for markedly impaired cognition, hypophonic speech, bradykinesia, limb ataxia, muscle rigidity, and absent vertical eye movements. His EEG showed generalized symmetrical slowing of the background rhythm. An MRI of the brain was performed (Siemens Espree; Siemens, Erlangen, Germany; 1.5 T), which included diffusion-weighted images (TR = 4900 ms; TE = 112 ms; FA = 90; NEX = 4), a FLAIR sequence (TR = 8000 ms; TE = 108 ms; TI = 2500; FA = 90) and T2-weighted images (TR = 4830 ms; TE = 101 ms; NEX = 2; FA = 150). His MRI revealed restricted diffusion within the putamen and caudate nucleus (Figs. 4a and b) and intense bilateral hyperintensity on FLAIR and T2-weighted images (Figs. 4c and d), left greater than right. Subtle restricted diffusion was noted in the bilateral thalami (Figs. 4a and b). The cortex demonstrated normal signal on DWI and FLAIR sequences. He progressed to have significant generalized myoclonus and akinetic mutism prior to his death. Autopsy examination, including analysis of brain tissue at the NPDPSC, confirmed the diagnosis of the sporadic form of Creutzfeldt-Jakob disease.
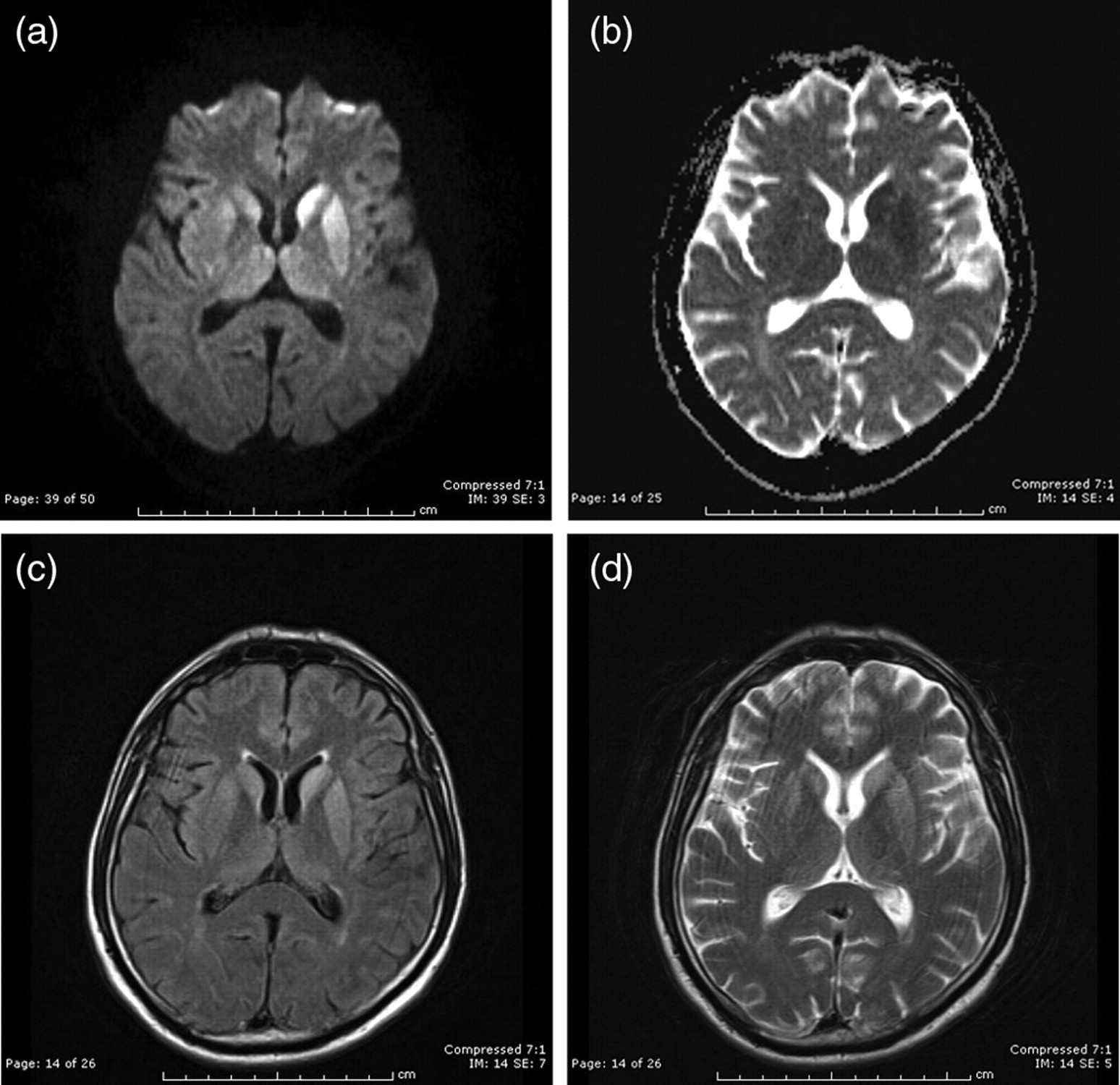
Sporadic Creutzfeldt-Jakob disease in a 58-year-old man. (a) Diffusion-weighted image and (b) ADC map demonstrate bilateral restricted diffusion in the putamen, caudate nucleus and pulvinar nucleus of the thalamus; (c) The FLAIR and (d) T2-weighted images demonstrate bilateral hyperintense signal in the putamen, caudate nucleus and pulvinar nucleus of the thalamus. The cortex was not involved in this case
Discussion
A characteristic feature of sporadic CJD is involvement of deep gray matter structures including the putamen and caudate nucleus. This can manifest as hyperintensity on FLAIR and T2-weighted images (3, 5) and restricted diffusion on diffusion-weighted images (DWI) (5). Diffusion-weighted imaging has been shown to be the most sensitive sequence (6), followed by FLAIR (7). Involvement of the deep gray matter structures may be unilateral or bilateral (8). Within the basal ganglia, the caudate nucleus is affected most frequently (8). Initial imaging may show abnormal signal in the basal ganglia limited to the caudate nucleus. Over the course of the disease, involvement may spread to involve the putamen (8). Thalamic involvement is typically seen in association with striatal and/or cortical involvement and is usually limited to the posterior and medial thalamus (9). Involvement of the thalamus in sCJD may be difficult to detect. Decreased ADC values in the thalamus may be observed when DWI and FLAIR changes are absent (9).
Abnormal signal is not limited to the basal ganglia in patients with CJD, however. The majority of patients with sCJD display signal abnormalities on FLAIR and diffusion weighted images in both the cortex and the basal ganglia (8). In early stages of sCJD, involvement of the caudate nucleus and the cortex is quite characteristic (8, 10). Signal abnormalities within the cortex manifest as ribbon-like hyperintensity on FLAIR and T2-weighted images and gyriform restricted diffusion on DWI (8). Diffusion weighting is the most sensitive sequence for detection of cortical changes (8, 11).
Isolated cortical abnormalities have been seen in 24% (6) to 33% (11) of patients with CJD. This may be the only finding in the early stage of disease before the onset of myoclonus or EEG findings. Patients with isolated cortical changes have been reported to have a prolonged disease course (5, 11).
Two of the three recent cases of sCJD at our institution displayed predominant involvement of the cortical gray matter, with one case demonstrating abnormal signal confined to the cortex only. Involvement of the deep gray matter was seen in two of the cases on both DWI and FLAIR imaging, but only one case demonstrated striatal involvement as the major finding. Diffusion-weighted imaging showed restricted diffusion in the involved gray matter in each case. Involvement of the cortical gray matter may only be apparent with diffusion-weighted imaging.
The cause of the diffusion restriction remains unclear. Bahn et al. suggested diffusion restriction was a direct result from spongiform degeneration (12–14). This could be owed to presence of vacuoles causing compartmentalization. Na et al. suggested direct deposition of the prion protein might add to the restriction of free water diffusion (15).
The authors believe the diffusion restriction to be secondary to predominantly intraneural vacuolization underlying the neurohistopathologic finding of spongiform degeneration within the soma and neurites. This would also explain the limitation in diffusion signal change to the cerebral cortex. Repetitive DWI evaluation in CJD patients may identify a disease specific pattern in diffusion signal/ ADC normalization which would explain reports on patients with normal or mildly elevated ADC values (16).
It is imperative to include CJD within the differential diagnosis of a patient with dementia and neurological abnormalities when isolated cortical restricted diffusion is present, with or without basal ganglia abnormalities.