
Abstract
Background
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) displays microcirculation and permeability by application of contrast-media and diffusion-weighted imaging (DWI) is a tool for quantification of cellularity in the investigated area. Recently published examples cover breast cancer, CNS tumors, head and neck cancer, gastrointestinal cancer, prostate cancer as well as hematologic malignancies.
Purpose
To investigated the influence of age, sex, and localization of the investigated region on findings of DCE-MRI and DWI.
Material and Methods
DCE-MRI-parameters amplitude A and exchange rate constant kep as well as the DWI-parameter ADC of the bone marrow of the lumbar vertebral column of 30 healthy individuals covering the typical range of age of tumor patients were evaluated. ADC was calculated using b=0 and a maximal b value of either 400 or 750 s/mm2.
Results
Amplitude A of DCE-MRI decreased with age (P = 0.01) and amplitude A, exchange rate constant kep as well as ADC based on b = 400 s/mm2 and b = 750 s/mm2, respectively, decreased significantly from the first to the fifth lumbar vertebra with P = 0.02, P = 0.05, P = 0.003, and P = 0.002, respectively.
Conclusion
Quantitative parameters of functional imaging techniques in bone marrow are influenced by the age of the examined individual and the anatomical location of the investigated region.
Conventional magnetic resonance imaging (MRI) is considered to be the best available imaging method for qualitative evaluation of bone marrow (1). This technique demonstrated that the distribution of hematopoietic and fatty bone marrow is age-related.
Dynamic contrast-enhanced MRI (DCE-MRI) and diffusion-weighted imaging (DWI) are functional MRI methods displaying changes caused by benign and malignant bone marrow diseases (2–5). Both methods comprise the possibility to acquire non-invasively (semi-) quantitative surrogate parameters representing perfusion and diffusion aspects in the analyzed region of interest (ROI). As multiple ROIs can be drawn in areas containing hematopoietic bone marrow, morphologic and functional information can be acquired from an extended area and finally compared to histology. As main advantages imaging information is available rapidly and all examinations can be repeated to monitor pathological changes as well as response to treatment.
The apparent diffusion co-efficient (ADC) of DWI reflects random movement of water molecules. This is mainly influenced by the presence of cell membranes and therefore by tissue cellularity (6). DCE-MRI measures the inflow and distribution of contrast agents in a defined tissue compartment. The distribution of contrast agents can be described by different models. The most common of them acquires two different parameters. According to the one used by our group amplitude A reflects vascular volume and exchange rate constant kep represents vascular permeability (7, 8).
The present analysis was performed to investigate the relation of DWI- and DCE-MRI-parameters as well as the dependency of age and sex in the bone marrow of 30 healthy controls. Furthermore, we were interested in the influence of the level of each lumbar vertebra on the different parameters.
Material and Methods
Subjects
In the context of a clinical study investigating the application of either DCE-MRI and DWI in patients with monoclonal plasma cell disease, 30 healthy Caucasian individuals (16 men, 14 women) with a median age of 56 years (range 29–74) were examined with DWI and DCE-MRI covering the lumbar spine. Age distribution was as follows: one individual was aged 20-29 years; four individuals were aged 30–39 years; four individuals were aged 40–49 years; 10 individuals were aged 50–59 years; 10 individuals were aged 60–69 years; and one individual was aged 70–79 years. The median age of the women was 56 years (range 33–67) and of the men 57 years (29–74) with no significant difference between them (P = 0.9). None of the test persons had a history of any systemic disease influencing bone or bone marrow. Non-related, healthy subjects were randomly chosen from volunteers raised by an invoking of individuals fitting in the age cohort of patients with multiple myeloma because the present study was performed in the context of a trial investigating the application of DCE-MRI and DWI in this disease entity. As basis for selection a median age of 55–59 years was aimed to fit the median age of the examined patients of the respective trial. However, we also tried to cover the whole range of ages comparable to that of patients. The study, as well as the participation of healthy volunteers, was approved by the institutional ethics committee. All examinations were performed after written informed consent on a 1.5 Tesla scanner (Magnetom Avanto with a CP spine array, Siemens Medical Solutions, Erlangen, Germany).
DCE-MRI protocol and image analysis
The entire spine of all individuals was examined from the first cervical vertebra to the sacral bone with sagittal STIR and sagittal T1-weighted SE sequences. This initial routine sequences were performed to gain further diagnostic information about the patients' bone marrow status within the study mentioned above. To achieve best comparability between patients and healthy controls the same protocol was used for the latter as well. The following dynamic MRI protocol was used: Optimized Saturation-recovery-TurboFLASH-Sequence (TR/TE 79/4.76 ms, FOV 380 mm, slice thickness 8 mm, voxel size 1.5 × 1.5 × 8 mm, matrix size 256 × 380 [FOV read 50%]), in eight sagittal slices, 22 measurements (total acquisition time 5.5 minutes), temporal resolution 11.25 sec per measurement cycle. Contrast media injection was started with the fourth measurement cycle using an automatic power injector (Spectris Solaris® EP MR-injection system; Medrad, Volkach, Germany). The i.v. injection of 0.1 mmol/kg Gadolinium-DTPA (Magnevist®, Bayer Schering Pharma, Berlin, Germany) was given over 30 s via a cannula placed in the antecubital vein followed by a saline flush of 30 mL at the same injection rate. Data were analyzed on a conventional PC workstation with the ‘MeVislab’ Software (MeVis Medical Solutions AG, Bremen, Germany).
The tissue-specific information contained in DCE-MRI–based signal intensity-time curves is described by two relevant model variables: Amplitude A (arbitrary units [a.U.]), which is proportional to the relative signal enhancement and the exchange rate constant kep (min−1) reflecting the contrast agent transit between the extra vascular and the intravascular compartment. A systematic analysis of ROIs encompassing a complete vertebral body was carried out using the commercial DCE-MRI tool mentioned above. For the manually drawn ROIs, encircling the whole bone marrow space of the five lumbar vertebrae, the software automatically calculated mean signal intensities on single image, respective vertebra. Also the change of mean signal intensity inside each ROI over time was plotted. Amplitude A and exchange rate constant kep were calculated for the signal intensity curve according to the model described by Brix et al. (7, 8). As proven by computer simulations, kep can be determined reliably in the range kep <13 min−1 so that all values for kep≥13 min−1 were fixed to 13 min−1 and were censored in the statistical analysis (9).
DWI protocol and image analysis
Dependent upon the body height of the study person the five lumbar vertebrae and 1–3 adjacent thoracic vertebrae were examined using a diffusion-weighted HASTE sequence with b values of 0, 400 and 750 s/mm2, respectively. Data were analyzed on a conventional PC workstation with custom made Software based on the ‘MeVis DWI-Stat-Module’ Software (MeVis Medical Solutions AG, Bremen, Germany). Analysis of ADC of manually drawn ROIs encompassing the bone marrow of a complete vertebra was performed. If the vertebral artery was visible in the dorsal vertebral body the ROI was drawn sparing the vessel. A ROI was drawn in the three central slices and the median was calculated (Fig. 1).
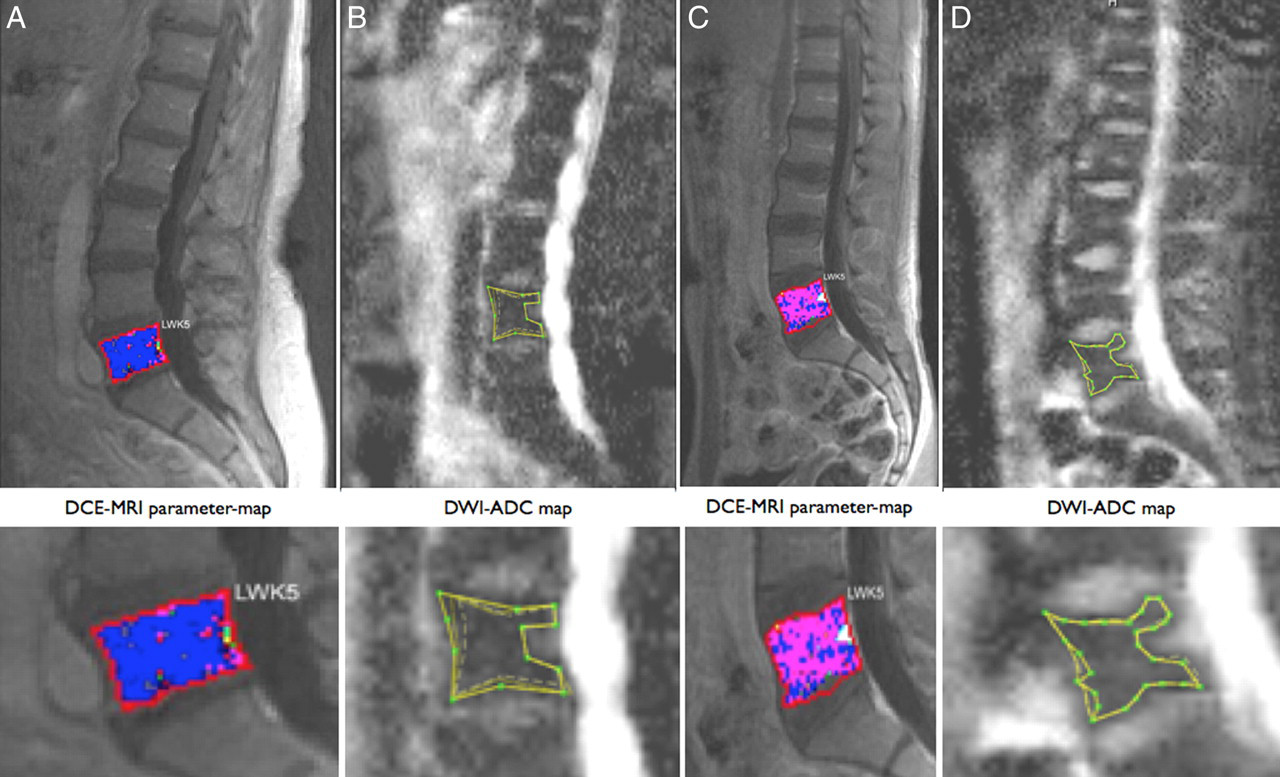
(A, B) Screenshots of parameter map of DCE-MRI (combination of amplitude A and kep) and ADC map DWI of the lumbar spine of a 60-year-old woman; and (C, D) a 29-year-old man. In each image a ROI is drawn manually as example around the fifth lumbar vertebra as it was done in the present analysis. Especially in the parameter map of DCE-MRI the difference of color coded parameters can be seen with higher values of Amplitude A and exchange rate constant kep in the younger subject
Statistical analysis
Wilcoxon's rank sum test was used to compare groups for age distribution. The study has a repeated measurement design, i.e. for each patient multiple MRI measurements were taken due to five different vertebra assessments. Impact of clinical parameters age and sex as well as of level of the examined vertebra within the spine on MRI parameters was evaluated with a linear mixed effects model with the investigated subject being a random effect in order to account for multiple measurements per individual. In addition, Page's exact two-sided non-parametric L trend test was used to test for a monotonic trend in MRI measurements across vertebrae. Correlation between DCE-MRI and DWI parameters was assessed with Pearson's correlation coefficient (rho) including 95% confidence intervals (95% CI) based on the subject's median values. P values less than 0.05 were considered statistically significant. Statistical analyses were carried out using the software package R, version 2.9.2 (10). Page's exact trend test was calculated with StatXact 7.0 software (STATCON, Witzenhausen, Germany).
Results
In 30 healthy controls 148 vertebral bodies were analyzed. Due to artifacts presumably caused by early osteoarthritis two lumbar vertebrae were not evaluable. Median, range, 25%- and 75%-quartile of median values of all five lumbar vertebrae of amplitude A and exchange rate constant kep of DCE-MRI as well as ADC of DWI at b = 400 s/mm2 and b = 750 s/mm2 are shown in Table 1 and Fig. 2.

Median, 25%-quartile, 75%-quartile and range of functional imaging parameters amplitude A [a.U.], exchange rate constant kep [min−1] and ADC [10−4 mm2/s] at b = 400 s/mm2 and 750 s/mm2, respectively, in the five lumbar vertebrae of the healthy volunteers
Median values and ranges of amplitude A, exchange rate constant kep and ADC at 400 and 750 s/mm2
Median estimated volume investigated per vertebral body was 8.018 mL (range 6.709–11.052 mL) for DCE-MRI and 9.112 mL (range 1.705–18.570 mL) for DWI.
In two individuals one vertebra each showed signs of osteoarthritis in DCE-MRI. The respective vertebrae were excluded from the subsequent analysis due to possible bias by minimal contrast enhancement.
Effect of age
A significant negative correlation between amplitude A and age was found with a P value of 0.01. Exchange rate constant kep was not correlated to age (P = 0.7) as were ADC based on b values of 400 s/mm2 and 750s/mm2 (P = 0.2 and P = 0.1, respectively) (Fig. 3)

Mean amplitude A [a.U.] and real amplitude A [a.U.] of each lumbar vertebra as functions of age. Black dots show median and white dots real values of amplitude A
Functional MRI and gender
No significant differences between men and women was found for amplitude A, exchange rate constant kep or ADC at b = 400 s/mm2 or 750 s/mm2 (P = 0.6; P = 0.2; P = 0.8 and P = 0.4 respectively).
Influence of the level of the investigated vertebra in the spine
For all parameters of functional MRI from the first to the fifth lumbar vertebra, a decrease of values was detected (Fig. 4). Median ranks and P values are shown in Table 2.
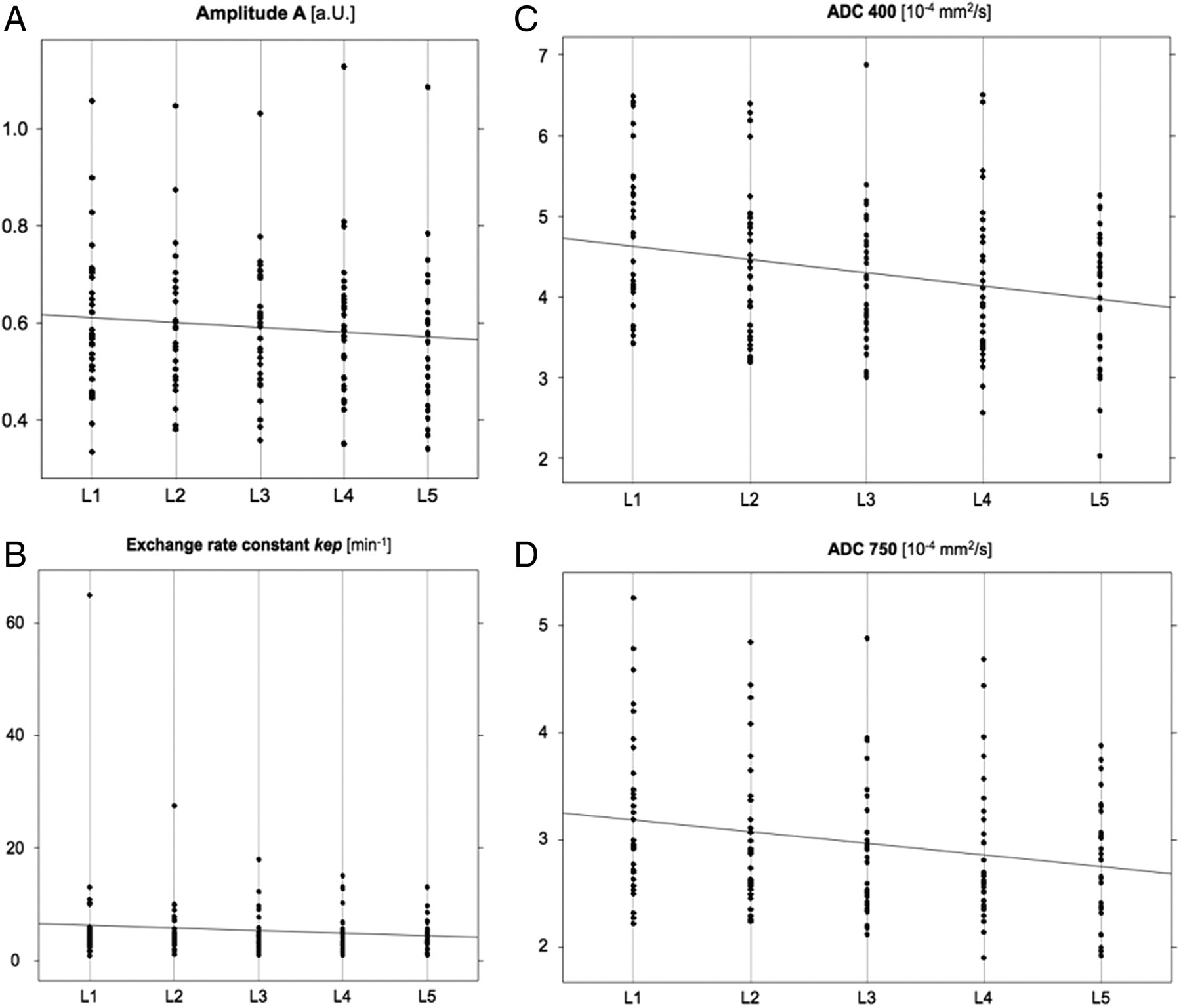
Decrease of functional MRI parameters from the first to the fifth lumbar vertebra: (A) amplitude A [a.U.]; (B) exchange rate constant kep [min−1]; (C) ADC [10−4 mm2/s] at a b value of 400 s/mm2; and (D) ADC [10−4 mm2/s] at a b value of 750 s/mm2 with linear regression line
Decrease in functional MRI parameters from upper to lower lumbar vertebrae
*Two-sided Page's L trend test
Correlation of DWI with DCE-MRI
Analysis of the correlation of DCE-MRI parameters with DWI parameters revealed a moderate correlation of amplitude A with the ADC at b values of 400 (rho = 0.52 and 95% CI [0.20, 0.74]) and 750 s/mm2 (rho = 0.55, 95% CI [0.23, 0.76]) and no correlation of exchange rate constant kep with ADC at 400 s/mm2 (rho = –0.1, 95% CI [–0.45, 0.27]) and 750 s/mm2 (rho = –0.16, 95% CI [–0.49, 0.22]).
Discussion
The aim of our examination was to detect influences of physiological and anatomic factors on parameters of functional MRI. Our analysis of functional MRI parameters in the lumbar spine of 30 healthy subjects revealed a decrease in amplitude A of DCE-MRI with increasing age. For all examined parameters, a decrease of values from the upper to the lower lumbar vertebrae was observed.
It is well-known that healthy bone marrow changes with age. The decline in hematopoietic marrow comes along with decreasing cellularity. The nascent space is filled mainly by fatty tissue. In a healthy adult approximately 50–60% of the whole bone marrow is hematopoietic (11). The cellular composition of red marrow consists of 60% hematopoietic cells and 40% adipocytes (12). In contrast, yellow marrow is almost entirely composed of fat cells (95%). Along with these changes of the blood forming compartment also the mineralized bone itself alters with age. The principal reason is senile bone loss, as for instance seen in postmenopausal osteoporosis and other conditions associated with an increased rate of bone remodeling.
While computed tomography is used to examine mineralized bone, MRI has demonstrated the highest sensitivity for imaging physiological or pathological processes that influence the distribution of fat and water (13, 14). This information is used to differentiate between normal and abnormal marrow. Therefore static and functional MRI techniques are applied in diseases arising from or affecting bone marrow. Especially in multiple myeloma, a number of studies demonstrated prognostic and pathophysiological significance of spinal and whole body MRI (3, 15–18).
Several studies and reviews have focused on multiple variables influencing the appearance of bone marrow in conventional MRI, however little is known about the changes in functional MRI techniques (19, 20). While DCE-MRI is applied to display microcirculation DWI is used to assess cellularity.
Interestingly a correlation of DCE-MRI parameters with both micro vessel density and cellularity in bone marrow has been demonstrated (21, 22). Also differences between age groups and gender as well as the upper and lower vertebral column influence parameters measured by DCE-MRI (23–26).
Furthermore, different studies of DWI in oncology showed a wide range of results concerning the correlation of ADC with cellularity. While several investigations found a lower ADC in malignant tissue as metastases or fractured vertebral bodies (27, 28), other studies found higher ADC values in hypercellular tissues caused by both infections or malignancies (4, 5, 27, 28).
In our study sample we found higher ADCs in examinations with lower b values. Also a low significant positive correlation of ADC in both examined b values with amplitude A of DCE-MRI could be demonstrated. Surprisingly no significant difference in correlation of ADC values with amplitude A of DCE-MRI was found for the two b values. Theoretically, perfusion effects are dominant at lower b values and thus, low b value ADCs were expected to show an increased correlation with amplitude A. This can be attributed partly to the limited range of values of amplitude A. Further investigation with a full range of b values is warranted to clarify these results.
From a biological point of view this correlation is complex. Angiogenesis is triggered by an increasing need of nutrition and oxygen if the tumor exceeds a certain diameter. Therefore a correlation of microcirculation with cellularity could be expected. On the other hand an effect of perfusion on the ADC depending on the b value is explainable by the underlying concept of image acquisition. We presume that as in other studies the ADC value in our examinations may be influenced more by perfusion effects than by diffusion. Supporting this fact our results show a significant but moderate positive correlation of ADC and amplitude A.
In accordance with our investigation, an analysis of Zhang et al. found no correlation of ADC and age (29). For DCE-MRI several studies revealed an age-dependency of microcirculation parameters (24, 26, 30). In one of them even a difference of parameters depending on gender was shown (26). Differences in MRI parameters reliant on the gender of the examined subjects could not be confirmed in our cohort. The new information in our analysis is that amplitude A is correlated positively to ADC and negatively with age.
This observation might be fostered by further developments of DWI which allow measurement of microcirculation without contrast medium. This is even more important since many tumor patients suffer from renal impairment or pain leading to time and contrast dose constraints.
Since most malignant diseases investigated by functional MRI are predominantly seen in older patients it is crucial to take this factor into account. Nevertheless an analysis of a patient cohort with multiple myeloma revealed no significant influence of age on DCE-MRI parameters (31). Probably, the tumor-induced angiogenesis outperform the age-related effects. However, these observations have to be confirmed in a larger patient group.
The decrease of parameters of functional MRI from the first to the fifth lumbar vertebra could be explained by more pronounced mechanical stress and local ischemia leading to increased conversion from red to yellow marrow in the lower compared to the upper lumbar spine (23, 32). A study on the structural behavior of the human lumbar spine motion segments showed greater stiffness at L4–L5 compared to L2–L3 under physiological conditions of axial preload and fluid environment (33). This indicates that the lower lumbar vertebrae sustain greater stress, which may influence perfusion and the normal aging processes of the vertebral body (23, 32).
Limitations of the presented analysis are possible effects of selection of subjects caused by the non-random selection of the healthy volunteers. However, we tried to minimize this bias by choosing non-related, healthy individuals raised by an invoking.
Also the pharmacokinetic model used may be criticized. Due to the long-term use of this model in our patient population in earlier studies, we had to use this model. Since most other algorithms are quite similar, our data should be comparable. Also, recently published studies tend to make use of descriptive curve analyses instead of model based evaluation.
Since the ROIs included the whole vertebra we minimized any bias and limitations caused by inter- or intraobserver variability or reliability.
In conclusion, quantitative parameters of functional imaging techniques in bone marrow are influenced by the age of the examined individual and the anatomical location of the investigated region. However, individual patient characteristics as especially their age have to be considered in the interpretation of results. In the near future DWI might allow the measurement of perfusion in bone marrow without the need of nephrotoxic contrast agents. Above all, this assumption has to be further investigated in studies comparing DWI with biopsies from the investigated region.
Footnotes
Acknowledgement
This study was supported by grants of the Deutsche José Carreras Stiftung e.V., the Dietmar Hopp Stiftung and the German Cancer Research Center.