
Abstract
Background
Previous studies have reported chest radiographic findings of consolidation and ground-glass opacity in patients with swine-origin influenza A (H1N1). However, most of these studies include both hospitalized and outpatients.
Purpose
To evaluate initial chest radiographic and CT findings of hospitalized swine flu patients, adults and children, confirmed with a real-time reverse transcriptase polymerase chain reaction (PCR) assay for H1N1 virus.
Material and Methods
All PCR-verified swine flu patients admitted to the Department of Emergency Medicine (October 1 to December 15, 2009) at Oulu University Hospital, in Northern Finland, who underwent frontal chest radiography within 24 hours of presentation and who were hospitalized, were included. The radiographs and CT scans were assessed for the presence of pneumonia and characterized by pattern and distribution. The patients' medical records were analyzed for demographics, underlying medical conditions, the admission to the intensive care unit (ICU), initiation of mechanical ventilation or non-invasive ventilation support (NIV) and death.
Results
Of 159 H1N1 influenza patients, 135 (85%) underwent chest radiographs at admission; 113 adults and 22 children. Findings of pulmonary infiltrates were detected in 62% (70/113) of adults and 64% (14/22) of children, being bilateral in 67% of adults and 64% of the children. The anatomic location of infiltrates was more often peripheral in adults; 42/70 (60%) vs. 4/14 (29%), P = 0.041, and diffuse among children; 9/14 (64%) vs. 26/70 (37%), P = 0.078. When the ICU and NIV patients were compared to less severe cases, on their chest radiographs four or five lobes were more often affected (65%, 11/17 vs. 34% 23/67, P = 0.029 ). The predominant radiographic findings were consolidation (93% of all patients, 91% of adults and 100% of children) and ground-glass opacity (74% of all, 77% of adults and 57% of children). Pulmonary emboli were detected by CT in 2/9 (22%) patients.
Conclusion
The pandemic 2009 swine influenza causes common and widely distributed infiltrates on chest radiographs among hospitalized patients, which are not peculiar to usual respiratory viral infections, and these findings can not be differentiated from usual bacterial pneumonia.
During the influenza pandemic in 1957–1958, it was observed that in pure influenza virus pneumonia, diffuse, bilateral, and perihilar infiltrates were demonstrated, which were indistinguishable from cardiac pulmonary edema (1). On the other hand, patients with simultaneous bacterial pneumonia commonly showed typical focal infiltrates confined to one or more lobes. In April 2009, the first case of swine-origin influenza A (H1N1) was reported in Mexico (2). Since then the infection has rapidly spread throughout the world as a new pandemic. In June 2009, the World Health Organization declared the H1N1 influenza infection a global pandemic (3). In August 2010 more than 214 countries and overseas territories worldwide have reported laboratory confirmed cases of pandemic influenza H1N1 2009, including over 18,449 deaths (3). In Finland, there have been reported 7669 laboratory confirmed infections and 44 deaths since June 2009 (4). Postmortem lung specimens have shown that in the USA, 29% of 77 swine flu patients who died between May and August 2009 had simultaneous bacterial pneumonia (5).
There have been some studies published about patients who underwent chest radiography during their hospitalization during the 2009 Influenza A (H1N1) pandemic from different parts of world, such as the United States, Canada, Brazil, Israel, Britain, Turkey, and Italy (6–19). According to these publications, swine flu causes widespread and typically bilateral involvement of the chest parenchyma. However, in some of these publications the results are based on medical records, or are small series, or include both inpatients and outpatients.
The purpose of this study is to review the chest radiographic and CT findings of 135 laboratory confirmed swine-origin influenza A (H1N1) patients, who represent practically all hospitalized patients among the population of 391,000 inhabitants of Oulu University Hospital district in Northern Finland.
Material and Methods
Patients
Our study was retrospective and based on register data. Therefore, the approval of the institutional review board was waived according to instructions of our hospital ethical committee. The study was performed in Oulu University Hospital, Finland. Data were collected for all the 159 consecutive hospitalized patients who had positive results of a real-time reverse transcriptase polymerase chain reaction (PCR) assay for the H1N1 virus, between October 1 and December 15, 2009. All patients who fulfilled the clinical criteria for confirmed H1N1 infection, who had undergone frontal chest radiography within 24 hours of presentation, and who were hospitalized after initial evaluation, were included in this study. Between October and December 2009, 135 patients fulfilled these criteria. Their medical records were analyzed for demographics, underlying diseases, symptoms, length of hospitalization, admission to the intensive care unit (ICU), initiation of mechanical ventilation or non-invasive ventilation support (NIV), and death.
Chest radiographs
The majority (90%, n = 121) of the chest radiographs were obtained with Fujifilm FCR XG-1 (Fujifilm Corporation, Tokyo, Japan) computed radiography equipment at the Oulu University Hospital, and the rest of the chest radiographs were acquired with other computed (Agfa CR MD4.0, Agfa HealthCare NV, Mariakierke, Belgium) or digital radiography (Canon CXD1-40, Canon Inc. Medical Equipment Group, Tokyo, Japan) equipment in primary healthcare. The portable anteroposterior chest radiographs were available in 62% (n = 84) of the patients and upright posteroanterior and lateral radiographs were obtained in 38% (n = 51) of the patients. Previous chest radiographs for comparison were available for 54% (n = 73) of the cases. The chest radiograph images were recalled from the digital image archive and were analyzed using a diagnostic workstation (neaView Radiology version 2.23, Neagen, Finland), equipped with two diagnostic quality 3 megapixel gray-scale monitors.
Chest CT
Chest CT examination was performed in nine patients. Eight of the CT scans were obtained using a 64-MDCT scanner (Siemens Sensation 64; Siemens AG Medical Solutions, Erlangen Germany) and one with a 16-MDCT scanner (GE LightSpeed Pro, GE Healthcare, Milwaukee WI, USA). All patients received IV contrast material (Omnipaque 350; GE Healthcare AS, Oslo, Norway, 80 mL, administrated at 4 mL/s) and were scanned in full inspiration with whole chest MDCT (detector configuration 64 × 0.65, kV 120, modulated mA, 1 mm reformation with 0.7 mm intervals or 16 × 1.25, kV 120, modulated mA, 1.25 mm reformation with 0.625 mm intervals). Three of the patients had also separate high-resolution CT scans (HRCT) of the chest. The CT images were also reviewed using a diagnostic workstation (neaView Radiology version 2.23, Neagen, Finland), equipped with two diagnostic quality 3 megapixel gray-scale monitors.
Image analysis
Two experienced radiologists (AJ and ER) separately analyzed all the chest radiographs and the computed tomography studies. If the interpretations differed, the reviewers analyzed the images together and made a consensus interpretation. The radiographs and CT scans were assessed for the presence of pneumonia, and the specific radiologic patterns of ground-glass opacities (GGO), consolidation, nodular opacities, tree-in-bud pattern, interstitial thickening of the peribronchovascular branches, airway wall thickening, and septal lines (20, 21). The presence of associated hilar, mediastinal, and pleural abnormalities, and the presence of pulmonary embolism were also assessed. In children, the hyperinflation of the lungs was assessed as well (21).
The involvement was categorized as unilateral or bilateral and the affected number of lobes was recorded. The anatomic distribution of the findings was characterized as central (≤4 cm from the hila), peripheral, or diffuse.
Statistical analysis
Statistical evaluations were performed with SPSS for Windows software (SPSS, version 13.0, Chicago, IL, USA), using Fisher's exact test.
Results
Chest radiographs
Of the 159 confirmed hospitalized H1N1 influenza patients, 135 (84.9%) underwent chest radiographs. The median duration of the symptoms was two days for children and three days for adults, while 38% of the patients were admitted to hospital either the day they became ill or during the second day from the onset of symptoms. Those 135 patients with chest radiographs had significantly more cough, dyspnoea and gastrointestinal symptoms than the 24 patients in whom chest radiographs were not taken (Table 1). The same held true for underlying diseases: in 63% with and in 29% without chest radiograph (P = 0.003, Table 1). In the chest radiograph group, there were 113 adult patients whose mean age was 45.7 years (range 17–88 years) of whom 52 were men (46%) and 61 women (54%). The remaining 22 patients were children (under 16 years old), of whom nine (41%) were boys and 13 (59%) were girls, with the mean age of 6.4 years (range 0–16 years). Eighteen of the patients (13%) required ICU admission and ventilation support. Three patients died (2%) at the ages of 25, 68, and 80 years due to severe underlying medical conditions (chronic neurological disease, coronary heart disease with severe heart failure, and severe obstructive pulmonary disease, respectively). All of them had pulmonary infiltrates on the initial chest radiograph. One of the patients had two lobes affected, while two of the patients had 4–5 lobes affected.
Symptoms and underlying diseases of hospitalized patients with laboratory-confirmed H1N1 infection
*Comparison between 135 patients with and 24 patients without chest radiographs
Five patients had a known secondary bacterial infection (4%). Their radiographic findings did not differ substantially from those of other influenza patients. When the chest radiographs between patients having underlying diseases were compared with those without co-morbidities, there were no differences in pulmonary infiltrates in chest radiographs (data not shown).
The imaging findings of chest radiographs are summarized in Table 2. Pulmonary infiltrates were observed in 84 of the patients (62%) and there was no difference between adults and children in this respect. Similarly, both groups had bilateral changes in two-thirds of cases. Among adults, at least four lobes were more frequently affected (43%) than among children (29%). Probably due to the small number of pediatric cases the difference did not reach statistical significance.
Summary of initial radiographic findings in hospitalized patients with laboratory-confirmed H1N1 infection
*Patient comparisons made between adults and children
†Proportion of all the affected lobes
The distribution of pulmonary infiltrates in different lobes is revealed in Fig. 1. When the distribution of infiltrates – i.e. peripheral, central, and diffuse, were compared (Table 2), adult influenza patients had peripheral findings more often (60% vs. 29%, P = 0.041, Fig. 2). On the other hand, diffuse infiltrates tended to be present more often among children (64% vs. 37%, P = 0.078). The predominant chest radiographic finding was consolidation (93% of all patients). However, consolidation, resembling typical air-space pneumonia, was rare as the only finding, both in adults 2/70 (3%) and children 3/14 (21%). Findings of GGO were detected frequently, 62/84 (74%), affecting 54/70 (77%) of adults and 8/14 (57%) of children (Fig. 3). GGO was accompanied with consolidations in 52/70 (74%) in adults and 8/14 (57%) in children. Significant lymph node enlargement was not identified on any chest radiographic images.

The distribution of pulmonary infiltrates in different lobes

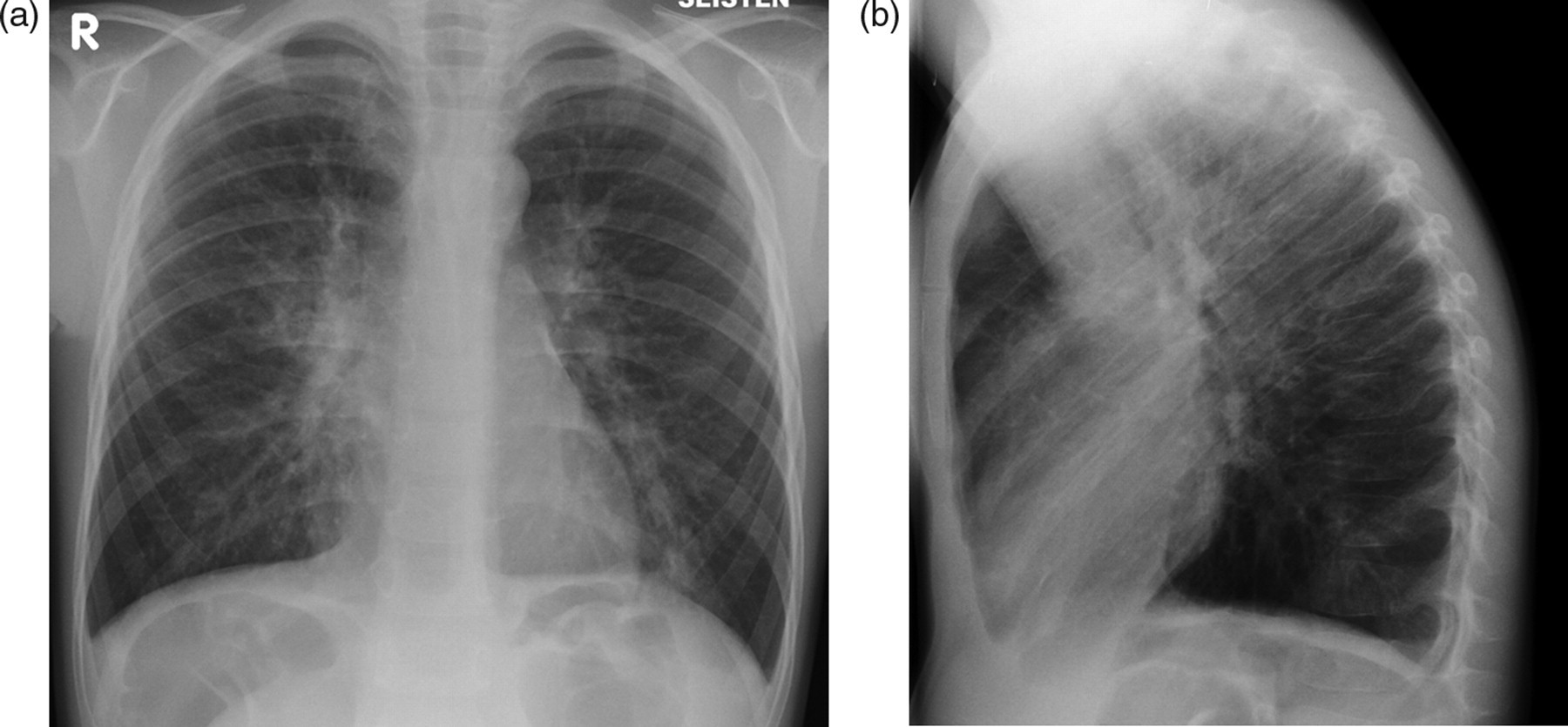
Typical pulmonary infiltrates in H1N1 influeza; 62-year-old man, who presented with cough and fever. The initial chest radiographic findings were bilateral peripheral consolidations and areas of GGO. Also peri-bronchial thickening was present
A 10-year-old girl with asthma had severe dyspnea, but no fever. Initial chest radiograph revealed area of GGO in the right middle lobe accompanying thickening of the peri-bronchovascular branches. She recovered after 3 days of hospitalization
In children, the second most common predominant finding after consolidation was the interstitial thickening of the peri-bronchovascular and airway branches, 10/14 (71%) (Fig. 4). In adults this finding was detected in 40/70 (57%). Hyperinflation of the lungs was present in three pediatric patients (3/14, 21%) and was associated with thickening of the peri-bronchovascular branches.

A 5-year-old boy with asthma had severe dyspnea, cough and fever. Initial chest radiograph presents thickening of the peribronchovascular branches and hyperinflation. This patient had desaturation, but recovered rapidly after 2 days of hospitalization
When the initial chest radiographic findings of severe cases (i.e. 18 ICU patients with mechanical ventilation and three patients needing NIV) were compared to 114 patients with milder disease, the following differences were observed: severe cases tended to have pneumonia more often than milder cases; 17/21 (81%) vs. 67/114 (59%), P = 0.085 and they had significantly more often four or five lobes affected than did milder cases; 11/17 (65%) vs. 23/67 (34%), P = 0.029. The infiltrates with severe cases were slightly more often bilateral than those with milder disease; 14/17 (82%) vs. 42/67 (63%), P = 0.157 (Fig. 5). Consolidations were observed as often both in severe cases 94.1% (16/17) and in milder cases 94.0% (63/67), P > 0.9.
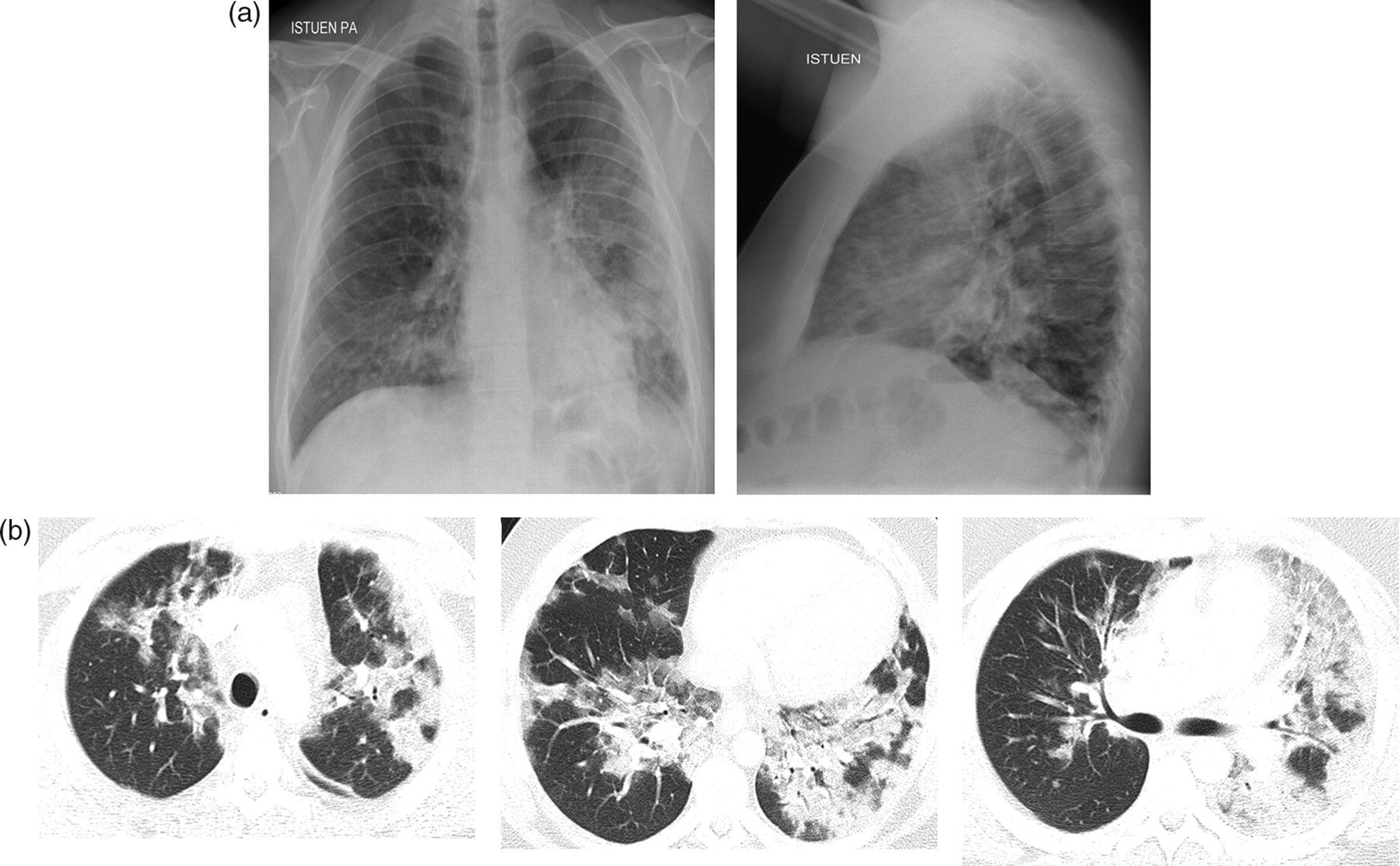
(a) A 27-year-old man with asthma, who presented with fever and cough 5 days before this initial chest radiograph. Despite antibiotic drugs (amoxicillin) the dyspnea had become worse. Bilateral GGO is seen and in the left lower lobe there are multiple consolidations. Because of hypoxia, the patient required ICU admission; (b) Chest CT on the second day of hospitalization showed multiple bilateral GGO and areas of consolidation. There were also nodular GGO present. The patient recovered and was discharged following 10 days of hospitalization
Chest CT scans
Chest CT examination (n = 9) was performed at 1–15 days (mean 5 days, median 4 days) after the initial chest radiographs in nine patients. The patients were aged 25–74 years old (mean 46.8 years), four were men and five women. Five of the patients had required ICU admission. The indications for CT scan were hypoxia in 6/9 (66%) cases and in most of the cases there was a need to exclude pulmonary embolism. Pulmonary infiltrates were seen in eight patients, of these, infiltrates were bilateral in seven (83%) (Fig. 6). All five lobes were affected in 6/8 (75%). Five of these patients suffered from hypoxia. The combination of GGO and consolidations was found in 6/8 (75%), and a pattern of predominant GGO in one patient. Consolidation was also the predominant finding in one patient. In addition to GGO and consolidation, thickening of the airway wall was detected in 3/8 (38%) and septal thickening in two patients. The distribution of the findings was diffuse in most of the cases, 6/8 (75%). Pleural fluid was present in 5/9 (55%). In one of these cases, there was a finding of pleural empyema. This patient did have laboratory confirmed Streptococcus pneumoniae pneumonia. Pericardial fluid was found in one patient. Pulmonary emboli were seen on CT in 2/9 (22%) patients. Lymph node enlargement was detected in 5/9 (55%), but it was relatively mild in all of the cases.
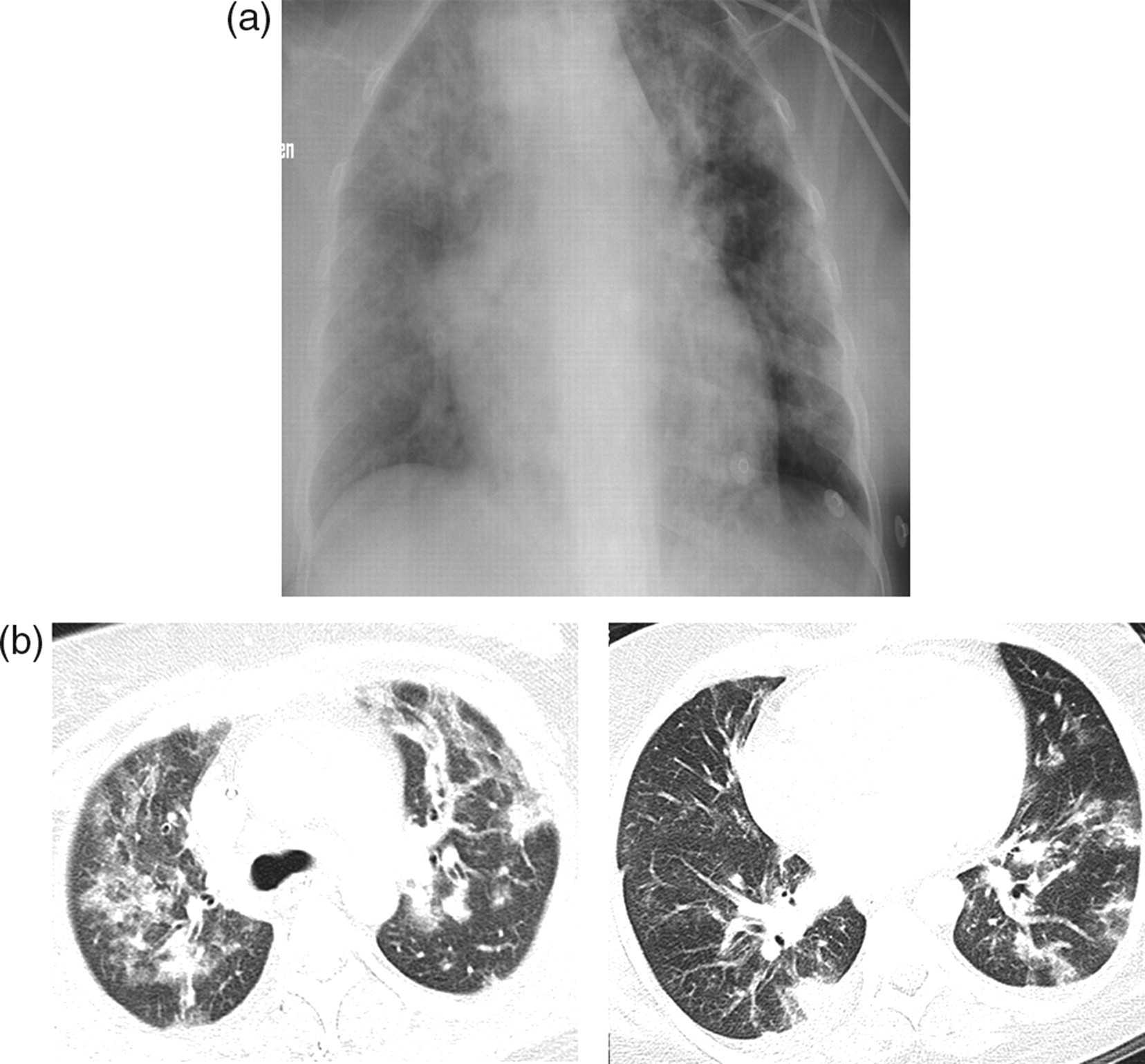
A 37-year-old woman with asthma had fever and cough for four days. She was treated in hospital for two days with antibiotics, but was admitted to the ICU because of dyspnea and hypoxia, where she needed mechanical ventilation. (a) The initial chest radiograph shows multiple bilateral areas of consolidation and GGO; (b) The following day, a chest CT showed bilateral areas of GGO and nodules. On the right, there is also small amount of pleural fluid. The patient recovered and was discharged following 5 days of hospitalization
Discussion
Our results showed that 62% of the hospitalized swine flu patients had pulmonary infiltrates of which consolidations and GGO were most frequently observed. Moreover, the most distinctive difference between adults and children was the anatomic location of infiltrates, which were more often peripheral in adults than children (60% vs. 29%) and diffuse among children (64% vs. 37%). In severe cases (ICU and NIV patients) four and five lobes were more often involved than in milder cases (65% vs. 34%).
Chest radiographs
In our series, 62% of all hospitalized patients had pulmonary infiltrates. This figure is almost identical of that reported on a large series from California, where 1088 hospitalized swine flu patients were analyzed. Chest radiographs had been taken of 833 patients (76%) and 547 (66%) had infiltrates suggestive of pneumonia or acute respiratory distress syndrome (6). In another USA series with 272 hospitalized swine flu patients from 24 states, 249 (92%) underwent chest radiography on admission, where findings consistent with pneumonia was observed only in 40% (7). This may be due to a selection bias, because study patients represented only 25% of those who were hospitalized due to swine flu during the study period. In a recent series from Israel, chest radiograph abnormalities were also seen less often than in our series with 179 swine flu patients treated in the emergency room on admission (8). Among these, 97 chest radiographs (54%) were available for analysis (80 hospitalized and 17 outpatients). Infiltrates compatible with influenza were observed in 39 patients (40%).
Bilateral involvement of infiltrates was seen in 67% of our cases, while the anatomic location of infiltrates was the upper lobes in 36% and lower lobes 47%. This is in harmony with earlier reports (8, 9). When severe and mild cases were compared in our series, the only statically significant difference (P = 0.0299) was seen between the involvements of the number of lobes, where four or five lobes were affected in 11/17 (65%) in severe cases and 23/67 (34%) in milder cases. Consolidation and GGO were the most typical finding in adults, which has also been shown in earlier studies (8–11). In our material, the peripheral distribution of the lesions in adults was typical.
Among our 22 pediatric patients there were fewer (14, 64%) pulmonary infiltrates than have been published earlier from Boston, USA (35, 97%) among 36 hospitalized patients (14). Bilateral involvement was also less often seen in our series (64% vs. 92%). The difference may be due to the severity of the disease, because in the Boston series 14/36 (39%) of the hospitalized patients were treated in the ICU. Interestingly, in that series, hyperinflation was the most common finding among 72 children treated as outpatients (14). In the series from Boston, abnormal chest radiograph was observed in 24 cases (33%), while hyperinflation was demonstrated in 17 of 24 (71%). In our series only three children out of 14 abnormal chest radiographs (21%) had hyperinflation. When we compared children and adults in our series, the only statistically significant difference was observed in the anatomic location of the infiltrates. Peripheral distribution was seen less often among children (29% vs.60%, P = 0.041).
Although in our series only 4% of the cases had documented bacterial infection, larger figures have also been reported (22). According to our experience it is impossible to differentiate chest abnormalities of H1N1 infection from bacterial pneumonia on admission. Because both viral and bacterial etiologies are possible, there is an indication to the initiation of bacterial and antiviral regimens. When bacterial examinations do not support bacterial etiology, bacterial antibiotic treatment can be discontinued during the treatment course. According to our national recommendations, almost all of the hospitalized patients received antiviral treatment (98% of the adults and 78% of the children).
The findings on the chest radiographs were not the only reason for hospitalization. Although during the H1N1 infection 62% of the hospitalized patients had pulmonary infiltrates, more than one-third of the patients had normal chest radiographs, which must be kept in mind.
Chest CT
Most of the patients requiring CT scan suffered from hypoxia. Therefore, it was not surprising that the pulmonary lesions were widespread among these patients, representing severe forms of H1N1 cases. However, all but one recovered completely. The findings of bilateral GGO and consolidations are in concordance with earlier studies (9–13). The distribution in our series was diffuse in most of the cases, probably because these patients had a clinically severe course. We observed two pulmonary emboli among nine cases (22%), while five out of 14 cases (36%) in Michigan had pulmonary emboli (9). In our small and selected CT series five patients (55%) had pleural fluid and lymph node enlargement.
Our study has several strengths. To our knowledge, this is the largest series describing the initial chest radiographic findings in hospitalized H1N1 influenza patients. Although our series was retrospective, this represents practically all hospitalized H1N1 influenza patients among the population of 391,000 inhabitants of Oulu University Hospital district in Northern Finland. The chest radiographs were obtained on admission for 85% of swine influenza patients. Moreover, a reference radiograph was available in 54% of the cases. Furthermore, our series allowed comparisons both between adults and children and between milder and severe cases. Every patient had swine influenza confirmed by PCR test. Since the median duration of the symptoms was two days for children and three days for adults, imaging findings typically represent influenza A (H1N1) infection. This was further supported by the fact that among those five patients with a known secondary bacterial infection the radiographic findings did not differ substantially from those of other influenza patients.
The limitation of this study was that our results represent only experiences of one center in Northern Finland, which should be remembered in the generalization of the results.
In conclusion, our results emphasize that the pandemic 2009 swine influenza caused common and widely distributed infiltrates on chest radiographs among hospitalized patients even in the first days of the disease, which are not peculiar to usual respiratory viral infections and these findings can not be differed from those of usual bacterial pneumonia. This emphasizes the use of both bacterial and antiviral treatment of hospitalized patients with respiratory infections during the course of the influenza A (H1N1) pandemic.