
Abstract
Splenic artery aneurysm is the most frequent visceral artery aneurysm and rupture of the aneurysm is associated with a high mortality rate. It is important to discriminate between a true aneurysm and a pseudoaneurysm that may be caused by pancreatitis, iatrogenic and postoperative causes, trauma and peptic ulcer disease. Multidetector-row CT angiography (MDCTA) allows detailed visualization of the vascular anatomy and may allow identification of aneurysms and pseudoaneurysms that affect the splenic artery. The objective of this article is to provide a review of the general characteristics of splenic artery aneurysms and pseudoaneurysms and to describe the findings of MDCTA.
Splenic artery aneurysm is the most frequent visceral artery aneurysm and rupture is associated with a high mortality rate (1, 2) whereas pseudoaneurysms are localized arterial disruptions caused by blunt or penetrating trauma, vascular intervention, or anastomotic disruption. It is important to discriminate between aneurysms and pseudoaneurysms because they require a different therapeutic approach. Splenic artery aneurysms can be managed by interventional radiological techniques (arterial stent or percutaneous angiographic embolization) or by surgery (operative occlusion, resection or arterial bypass) whereas splenic pseudoaneurysms are successfully treated with selective catheterization of the splenic artery and direct thrombin injection into the pseudoaneurysm lumen.
Multidetector-row CT angiography (MDCTA) allows detailed visualization of the vascular anatomy and allows identification of aneurysms and pseudoaneurysms affecting the splenic artery. The potential and diagnostic applications of MDCTA have greatly improved because of its high spatial and temporal resolution, the use of fast contrast material injection rates and postprocessing tools.
In this article we review the general characteristics of splenic artery aneurysms and pseudoaneurysms and describe the findings of MDCTA.
True splenic artery aneurysms
Splenic artery aneurysm (SAA) is the most frequent visceral artery aneurysm (60% of all visceral aneurysms) and the third most common of intra-abdominal aneurysms after aortic and iliac artery aneurysms (1, 2). The incidence of SAA is 0.01–0.2% and the reported prevalence is 0.8% at angiography and 0.04–0.10% at autopsy (3). However, data on prevalence vary widely, and in fact a prevalence of 10.4% was reported in an autopsy series on patients 60 years or older with special attention given to the splenic artery (4).
SAA are usually small (<3 cm in diameter) and the mean size of SAA is reported to be 2.1 cm (5) (Fig. 1). The size of a SAA rarely exceeds 3 cm and if larger than 3 cm (Fig. 2), it is known as a giant splenic artery aneurysm (GSAA). GSAA larger than 10 cm are extremely rare (6) and must because of their size be treated rapidly before rupture. SAA are most often saccular, exceptionally fusiform and are in about 80% of the cases located in the distal third of the splenic artery (2, 7). Peripheral calcifications are frequent and it has been reported that 80% of SAA show atherosclerotic changes including calcifications and mural thrombi (8) (Fig. 3).
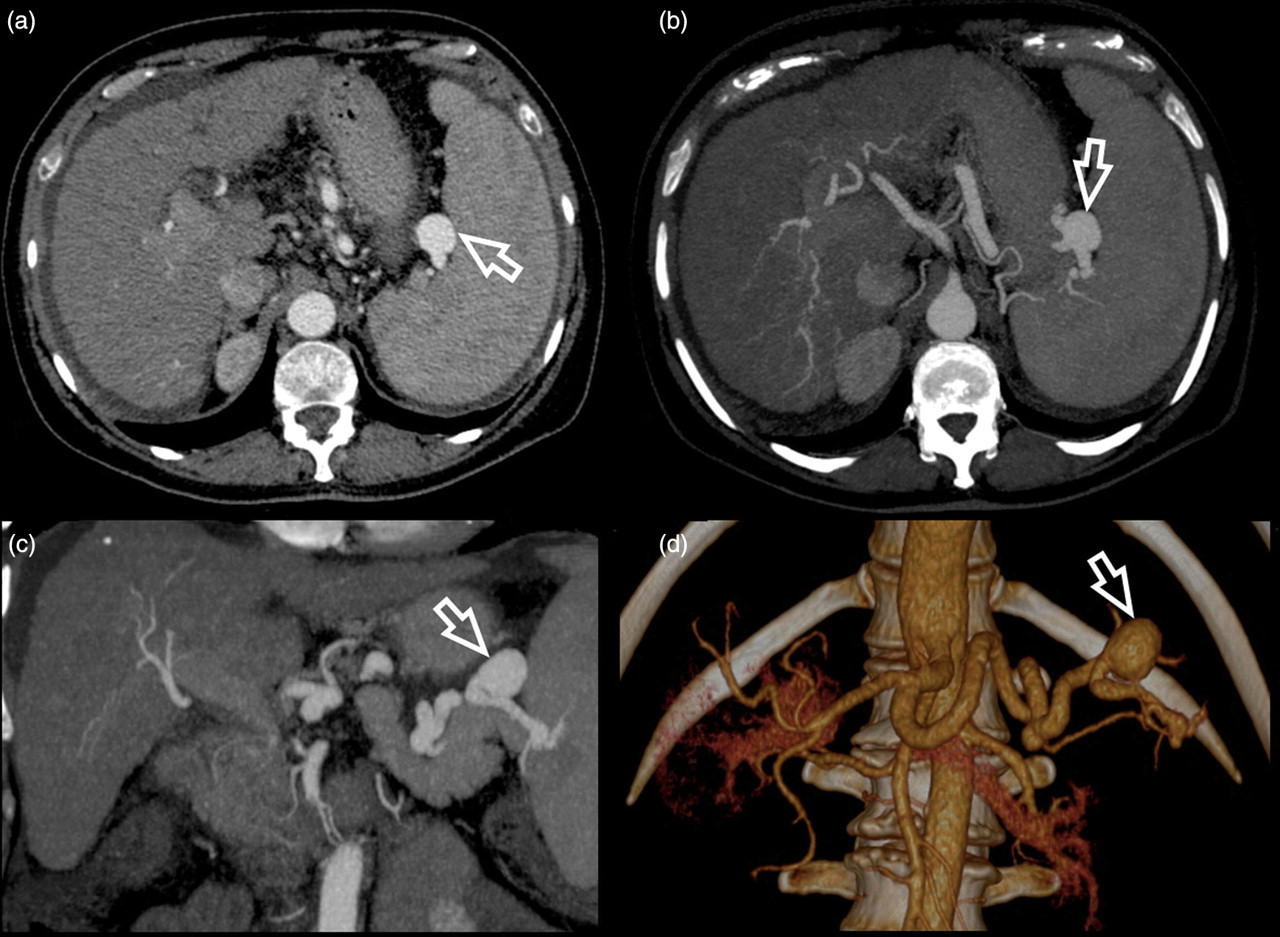
A 67-year-old man undergoing liver evaluation for suspected HCC. Arterial phase contrast-enhanced MDCT scan shows 2.9 cm distal splenic artery aneurysm located (white open arrow) near the splenic hilum. (a) MDCTA axial image, (b) MIP postprocessed images according to the axial plane, and (c) coronal plane and (d) VR post-processed image clearly demonstrate the aneurysm
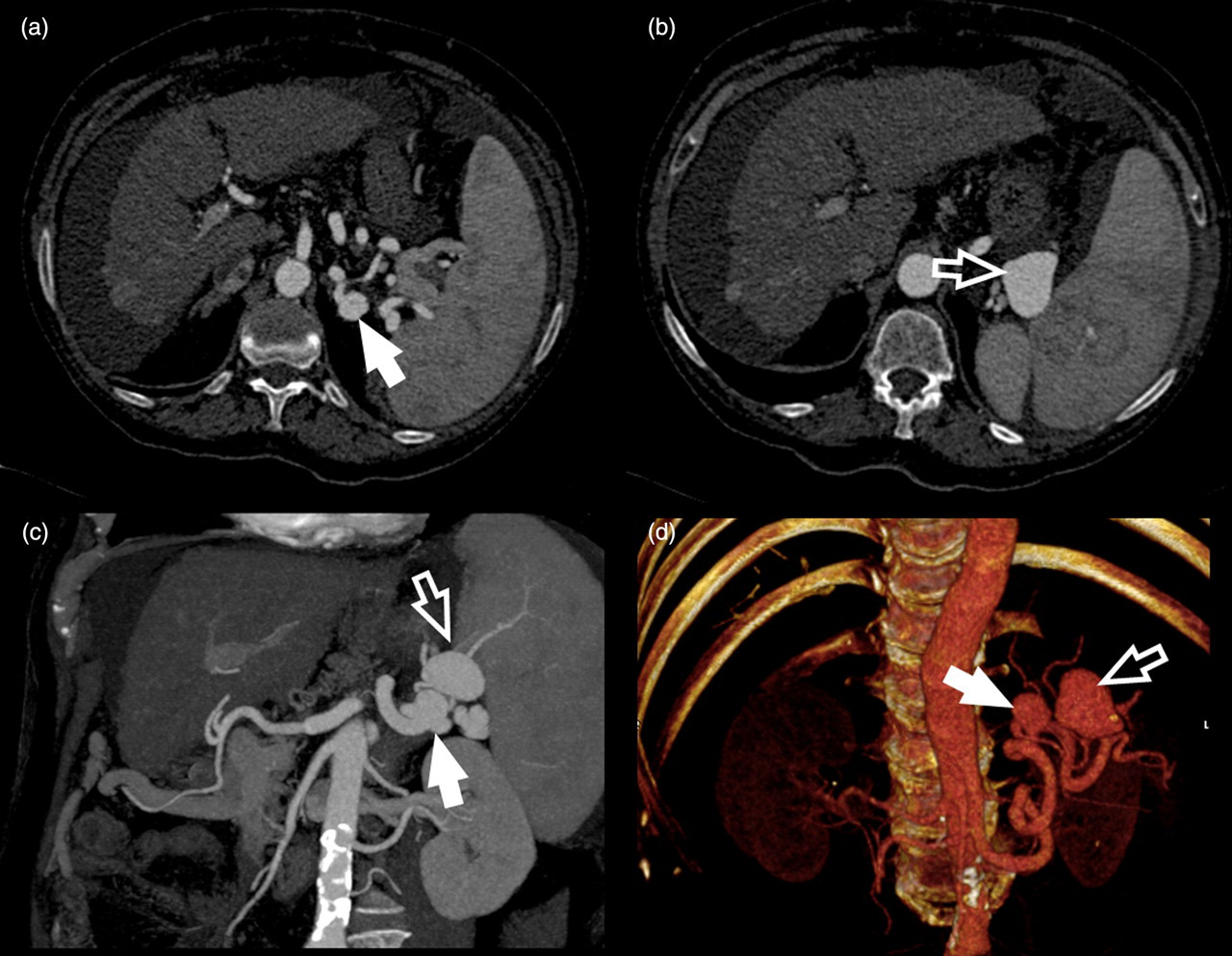
A 69-year-old man with a history of hepatic cirrhosis. (a and b) MDCTA axial images, (c) MIP postprocessed images according to the coronal plane, and (d) VR postprocessed image demonstrate two SAA (white arrows: SAA of 2.4 cm and open white arrows: SAA of 4.9 cm)
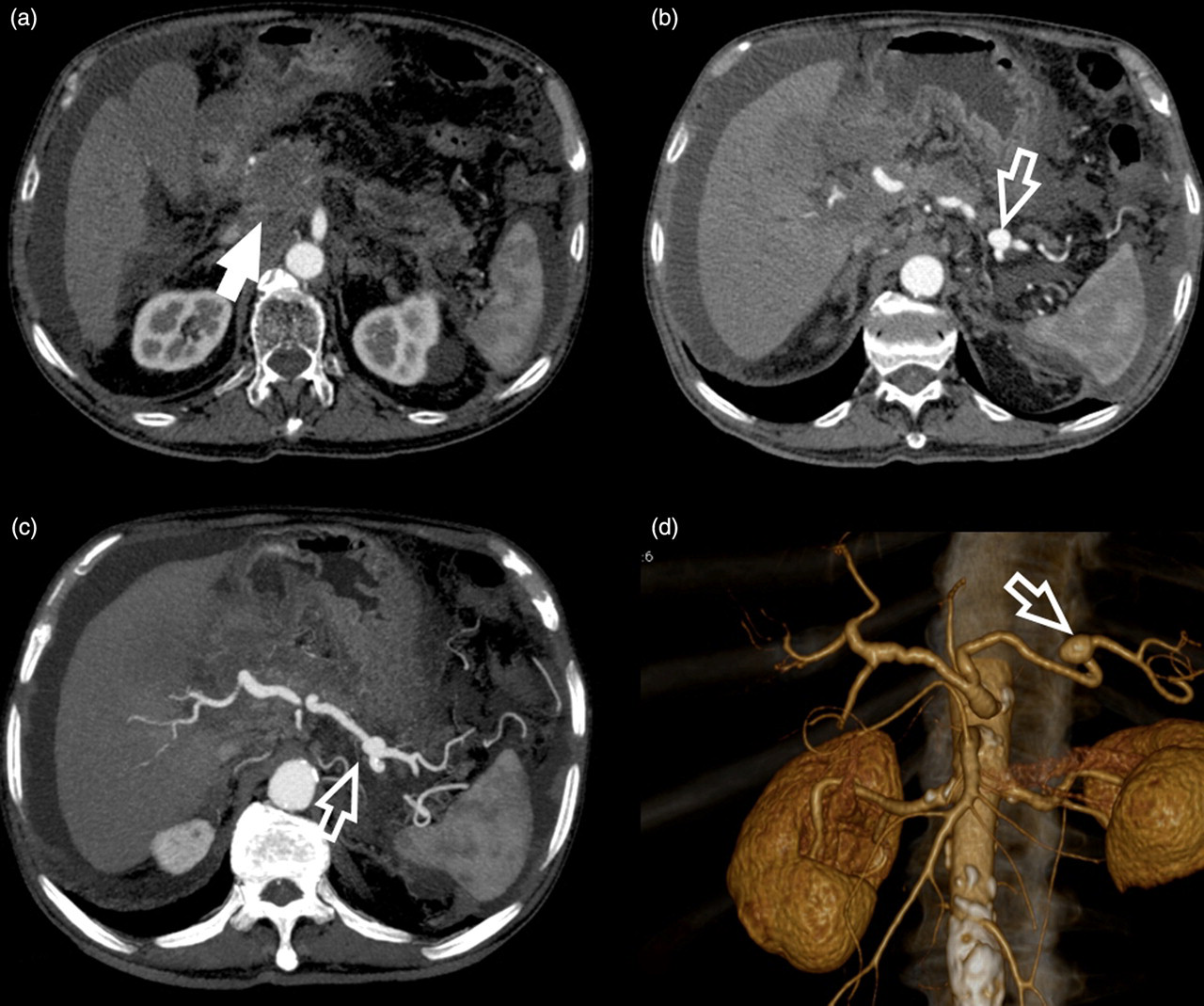
A 67-year-old woman with a history of (a) neoplasm of the head and pancreas body (white arrow). (b) A 1.9-cm enhancing mass is visible in the region of the pancreatic tail in the post-contrast axial image, (c) MIP image, and (d) VR image. This finding is related to previous obstructive pancreatitis secondary to the cephalic mass
Although arterial aneurysms are more common in men, GSAA occurs predominantly in women (nearly 80% of all GSSA cases) (9), especially during pregnancy or in multiparous women (2, 9, 10). Hormonal and hemodynamic alterations specific to pregnancy probably contribute to intimal hyperplasia and fragmentation of the arterial wall. In particular, during pregnancy, high splenic blood flow, and increased hormone levels (oestrogen, progesterone, relaxine) have a deleterious effect on the elastic tissue of the splenic artery (3, 10), which in turn may lead to aneurysm formation. These effects are cumulative with each successive pregnancy (5). Only 20% of all SAA are multiple (2, 11) (Fig. 2). Moreover, the prevalence of splenic artery aneurysm is markedly increased in patients with portal hypertension and is estimated to be between 7% and 20% in patients with cirrhosis (7). Other uncommon causes of SAA include fibromuscular dysplasia, infection, congenital anomalies, vascular trauma, inflammatory processes, and degenerative arterial disease (12, 13). However, arteriosclerosis is rarely the primary causative factor (14). The cause of SAA is unknown. However, local failure of the connective tissue of the arterial wall to maintain the integrity of the vessel wall probably plays a major role in the development of SAA. This leads to fragmentation of elastic fibres and a loss of smooth muscles.
Splenic artery pseudoaneurysms
Pseudoaneurysms are localized arterial disruptions caused by blunt or penetrating trauma, vascular intervention, or anastomotic disruption. Blood is surrounded by adjoining tissues and fibrous reaction. Pseudoaneurysms must be distinguished from true aneurysms, which originate from a pathologic process in the arterial wall. Pseudoaneurysms are caused by arterial disruptions that can be categorized into two main types: those that result from a perforation of an artery by traumatic or iatrogenic injuries and those that result from rupture of a surgical vascular anastomosis. It is not uncommon after acute pancreatitis to detect splenic artery pseudoaneurysms secondary to digestion of the arterial wall by proteolytic pancreatic enzymes (15, 16). Secondary hemorrhage from pseudoaneurysms may also involve the pancreatic duct, peritoneum, retroperitoneum, adjacent organs (stomach, colon), or a pseudocyst if present (17). In the case of pancreatitis, pancreatic enzymes are thought to cause a necrotizing arteritis with destruction of the vessel wall architecture and fragmentation of elastic tissues and subsequent weakening of the wall by pancreatic enzymes. Other authors (17) have reported that pancreatitis-related pseudoaneurysms can form, in addition to direct damage of vascular structures by the spread of pancreatic enzymes from severe inflammation: a longstanding pseudocyst may induce a pseudoaneurysm, caused by vascular erosion from enzymes within the pseudocyst, direct compression, or ischemia.
Autodigestion of the arterial wall by the enzyme and the spread of inflammation can result in pseudoaneurysm formation secondary to pancreatitis. Alternatively, an established pancreatic pseudocyst may erode into a visceral artery, thereby converting the pseudocyst into a large pseudoaneurysm.
Other causes of splenic artery pseudoaneurysm other than pancreatitis include iatrogenic and postoperative causes, trauma, neoplasm, and peptic ulcer disease (18) (Fig. 4). Splenic artery pseudoaneurysms are usually larger than SAA (the mean diameter of pseudoaneurysms is 4.8 cm, with a range of 0.3 to 17 cm). Compared to SAA, splenic artery pseudoaneurysms are rare. In a large series published by Tessier et al. (18), 10 splenic artery pseudoaneurysms were compiled over 18 years. To date, fewer than 200 cases have been reported in the English-language literature (8).
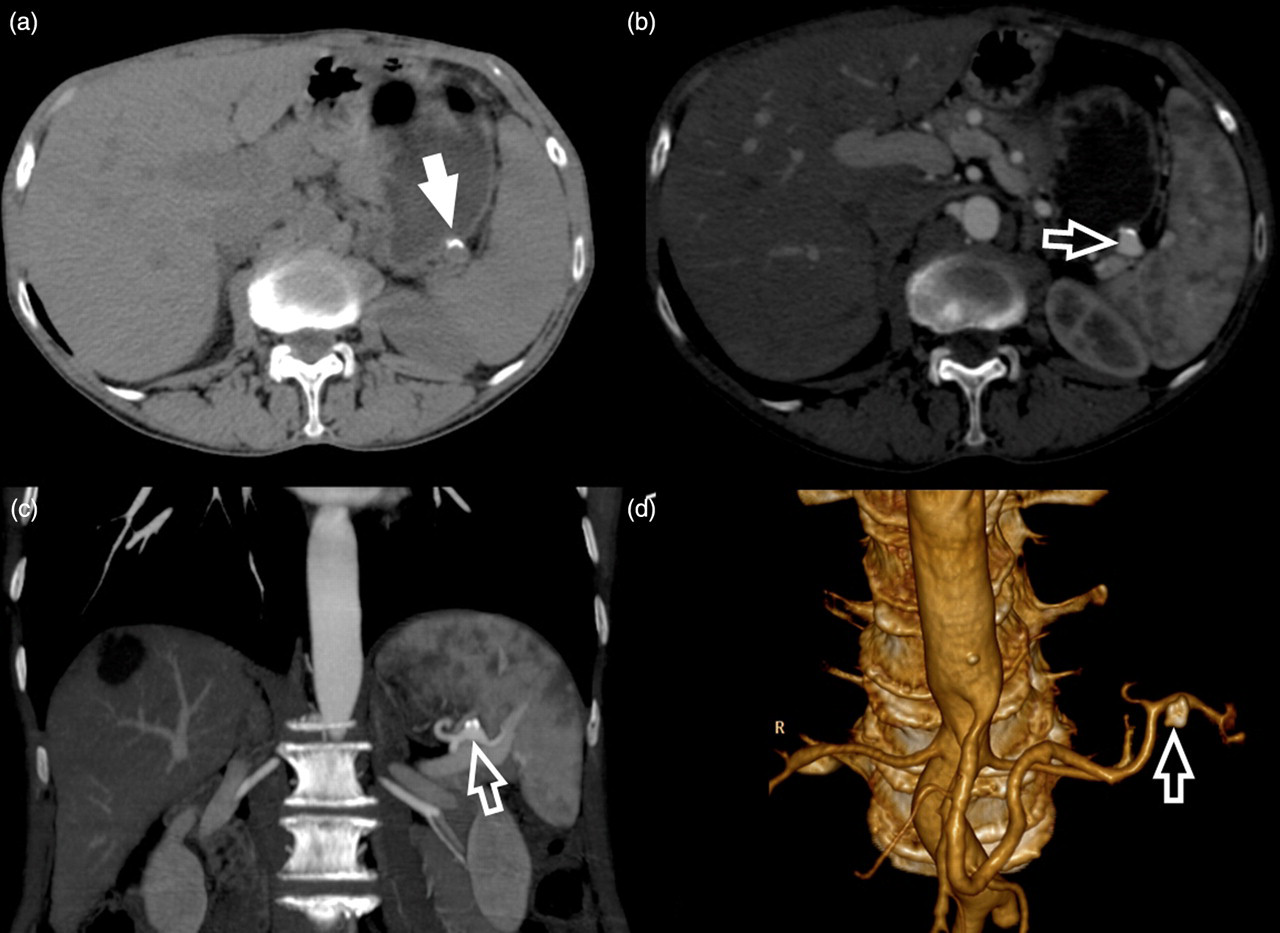
A 61-year-old man with a small (1.5 cm) splenic artery aneurysm detected 5 years previously who is being evaluated for stability. A peripheral calcification (white arrow) is visible in the basal scan (a). After administration of contrast material, the aneurysm (white open arrow) and the calcification are visible in (b) the axial image, (c) the MIP postprocessed image according to the coronal plane, and (d) the VR postprocessed image
Symptoms
The principal complication of a SAA >2 cm is rupture (1, 9, 11, 19). The reported risk varies from 2% to 9.6% (11, 19). Rupture sometimes occurs in the splenic vein and often in the peritoneal cavity causing cataclysmic bleeding. In 30% of all cases, rupture occurs in a visceral organ (19) such as the pancreas, the colon or the stomach (9), causing a digestive bleed. To date, out of more than 3000 reported digestive artery aneurysms, fewer than 100 intragastric ruptures have been reported (20). The rupture of a SAA was first reported by Beaussier in 1770 (21). Rupture of a SAA is rare; however, the rupture of splenic artery aneurysms that are left untreated is associated with a high mortality rate. SAA rupture results in an average mortality of 25% (10, 11), increasing to about 70% during pregnancy with 95% fetal mortality (1).
Initially, the rupture may be tamponaded in the lesser omental sac with apparent clinical stabilization. Eventually, the blood escapes into the free peritoneal cavity, either through the foramen of Winslow or through rupture of the pars flaccida, which is part of the omentum. Very few patients (5%) present with symptoms before their SAA ruptures (22, 23). Other complications have been described such as ruptures into a hollow viscus or the pancreatic duct, and development of splenic arteriovenous fistulas. The overall mortality rate from a ruptured SAA justifies its management. Indications for treatment of a SAA or pseudoaneurysm include specific symptoms (e.g. left upper quadrant pain, epigastric pain, and back pain), female gender and childbearing age, the presence of portal hypertension, planned liver transplantation, a pseudoaneurysm of any size, and an aneurysm with a diameter of more than 2.5 cm.
Management
SAA can be managed by interventional radiological techniques (arterial stent or percutaneous angiographic embolization) (3, 24) or by surgery (operative occlusion, resection or arterial bypass) (3, 20). However, SAA that are distally located, near the spleen hilum, may require a splenectomy (3). Historically, open surgical excision of the aneurysm, with or without splenectomy, is the conventional treatment, and is both efficient and durable (25–27). Surgery for SAA is associated with a mortality rate of approximately 1%, but mortality is increased in patients with pancreatitis, in whom it is 16% for those with aneurysms in the pancreatic head and 50% for those with pancreatic body aneurysms (7). Laparoscopic ligation has also recently been described with good results, but has rarely been used (28). Endovascular treatment (such as transcatheter embolization, placement of a covered stentgraft) (Figs. 5 and 6) to exclude the aneurysm is an emerging therapy for SAA and other visceral aneurysms, with constantly improving results. These minimally-invasive endoluminal techniques may offer a distinct advantage over conventional repair. Transcatheter embolization is associated with significantly lower morbidity and mortality compared to surgical procedures (29, 30). Precise selection of the occlusion site is necessary to preserve collateral blood flow to the spleen via the gastric, omental, and pancreatic vessels. Embolization of intrasplenic lesions may be performed with microcatheter-based techniques, with a success rate of 80–90% for percutaneous transcatheter embolization. Percutaneous needle placement followed by administration of thrombin directly into the aneurysm has also been successfully used to treat splenic artery aneurysms when transcatheter embolization is not possible or has failed. Endovascular treatment offers the potential benefit of maintaining splenic perfusion while excluding the aneurysm, thereby eliminating the risk of rupture or infarction (31, 32).

A 65-year-old female patient. (a) VR postprocessed image shows a 3.4 cm splenic artery (white arrow) aneurysm that was treated using (b and c) an endovascular procedure with stent placement (white arrows). MDCTA was performed after the procedure and the VR postprocessing image (d) demonstrates the stent localization whereas the MPR (e) shows the patency of the stent (white open arrows)

A 69-year-old-male patient. Example of coil embolization of a SAA. (a) The splenic artery that was injected with contrast material to demonstrate the SAA; (b, c, d) the coils are deployed to fill the aneurysm
Imaging and MDCTA
Although SAA were once thought to be uncommon, they are being diagnosed with increasing frequency with the wider use of cross-sectional techniques (8). Most SAA are detected incidentally during diagnostic imaging performed for other indications. Various imaging modalities including plain radiographs, sonography, CT, and angiography have been used to identify SAA (9). An abdominal radiograph rarely shows a prevertebral calcification or a calcified rim nodule in the splenic hilum (33). Therefore, this imaging technique cannot be considered reliable. Sonography has also been used to study SAA (34). On sonograms, a SAA typically manifests as a left hypochondrial pulsatile cystic lesion if not obliterated by overlying stomach gas (33). However sonography suffers some important limitations in the diagnosis of SAA, including poor interobserver agreement (33) and particular conditions such as shadowing from the bowel gas, obesity, and arteriosclerosis, which may markedly reduce the diagnostic sensitivity. Magnetic resonance angiography (MRA) plays a role in the diagnosis of SAA and gives an improvement in spatial resolution compared to sonography. However, MRA is not always available for emergency procedures (33, 35). Other limitations of MRA include its contraindication in patients with pacemakers, and in those patients who are unable to hold their breath or suffer from claustrophobia. In recent years digital subtraction angiography (DSA) has been the gold standard for identification of SAA, since its high temporal and spatial resolution allows optimal analysis of arterial vascular structures. However, DSA also has some important limitations: cost, procedural risk, and biological risk (in particular, radiation dose).
MDCTA is an important imaging modality for non-invasive assessment of the vascular system and represents an excellent tool for diagnosing SAA. MDCTA has been established as the method of choice for the diagnosis, treatment planning, and follow-up of most diseases of the abdominal arteries, including the aorta, visceral arteries, and the splenic artery. In these anatomical regions, digital subtraction angiography has recently been replaced by CT angiography. Following the introduction of MDCTA technology patients can now be imaged quickly during the arterial phase with exquisite spatial resolution. The shorter scanning time required for MDCT scanners permits better visualization of the blood vessels and has improved the contrast material enhancement of the adjacent organ parenchyma. Besides being able to assess the location and size of the SAA, MDCTA may also reveal ruptured aneurysms, intra-abdominal hemorrhage, and associated underlying diseases. When MDCTA reveals an intra-abdominal hemorrhage, the site of bleeding or the origin of active extravasation of the contrast material should be identified. The differential diagnoses of intra-abdominal hemorrhage include traumatic solid visceral or mesenteric injuries, intra-abdominal tumor bleeding, abdominal aortic aneurysm rupture, and visceral aneurysm rupture. Moreover, all necessary data for endovascular treatment can be obtained by MDCTA by measuring the size of the neck of the aneurysm, the calibre of the artery immediately before and after the aneurysm and the length of the covered stent (Fig. 5).
MDCTA technique
MDCTA acquisition parameters such as section thickness, increment, pitch, kV and mAs can differ markedly depending on the CT scanner employed and the number of detectors. For this reason these aspects will not be described specifically in this article (Table 1). With existing MDCT scanners, up to 320 simultaneous helices are acquired and the performance of the system has greatly improved compared to CT scanners used in previous decades. Table 2 shows the technical parameters of MDCT used in our hospital to produce the images of the cases presented in this paper. We use two multidetector-row CT scanners (a 16-detector-row scanner [Philips Brilliance, Best, The Netherlands] and a 64-detector-row scanner [Sensation Cardiac 64, Siemens Medical System, Erlangen, Germany]).
General acquisition parameters of MDCTA
*Over a length of 50 cm
MDCTA parameters used in our hospitals
The first step in the study of abdominal arteries using MDCTA is usually the acquisition of a lateral scout image in order to define the correct field of view (FOV). Some authors suggest performing a basal acquisition (36) and in our opinion if a MDCT examination is performed when intra-abdominal bleeding is suspected basal acquisition is always recommended. Arterial enhancement is provided by the intravenous administration of 70–100 mL non-ionic iodinated contrast material, at a variable injection speed of 3–6 mL/sec (37, 38); we usually use a flow rate of 5 or 6 mL/sec. In fact, by using high flow rates it is possible to achieve higher and faster opacification of the splenic artery.
After contrast medium is administered, the degree of splenic artery luminal enhancement, defined by the change in Hounsfield units (HU), is dependent on delivering a sufficient amount of iodine (iodine dose) at an appropriate rate (iodine flux). Fleischmann indicated that each milligram of iodine per mL of blood produces an increase of 25 HU (39). For most diagnostic quality CTA studies, arterial enhancement of at least 250–300 HU is required. However, this may vary depending on the patient's body weight and the level of image noise. The recommended minimum iodine dose is 400–600 mg I/kg (1.1–1.7 mL/kg of 350 mg I/mL) with a suggested iodine flux of 1.2–1.5 g I/sec (i.e. 3.4–4.3 mL/sec for 350 mg I/mL) (39, 40). Therefore, we usually use 370 mg I/mL because this results in higher HU hepatic artery values than the use of 300 mg I/mL. By analyzing renal and hepatic arteries, Saba et al. (41, 42) demonstrated that optimal image quality is obtained when the intra-luminal HU value is >300 HU. A contrast material bolus may be followed by a saline bolus in order to reduce streak artifacts due to beam hardening. The acquisition delay time is individually determined for each patient using a bolus-tracking system (Sure Start, Smart Prep, CARE bolus) or even by using personal observation to empirically calculate the delay, which usually ranges from 15 to 21 seconds (43, 44).
MDCTA postprocessing techniques
The development of multidetector-row CT, in combination with advances in computer hardware, software, and display technology, has facilitated three-dimensional (3D) image reconstruction. Curved planar reconstruction (CPR), maximum intensity projection (MIP), and volume rendering (VR) are the three most commonly used 3D reconstruction techniques (Figs. 1–5).
CPR
Curved planar reconstruction is a 2D, flexible multiplanar re-formatting method that works along the course of the target artery and can be performed by using an axial image as a reference to define the course of the desired re-formatting (Fig. 7). This method is useful for displaying arteries (45–47). Depending on the available software, CPR can be rotated around the central path through the vessel and thus is able to optimally display mural thrombi and calcifications in their longitudinal extent. One important drawback of CPR is that measurements are not possible.
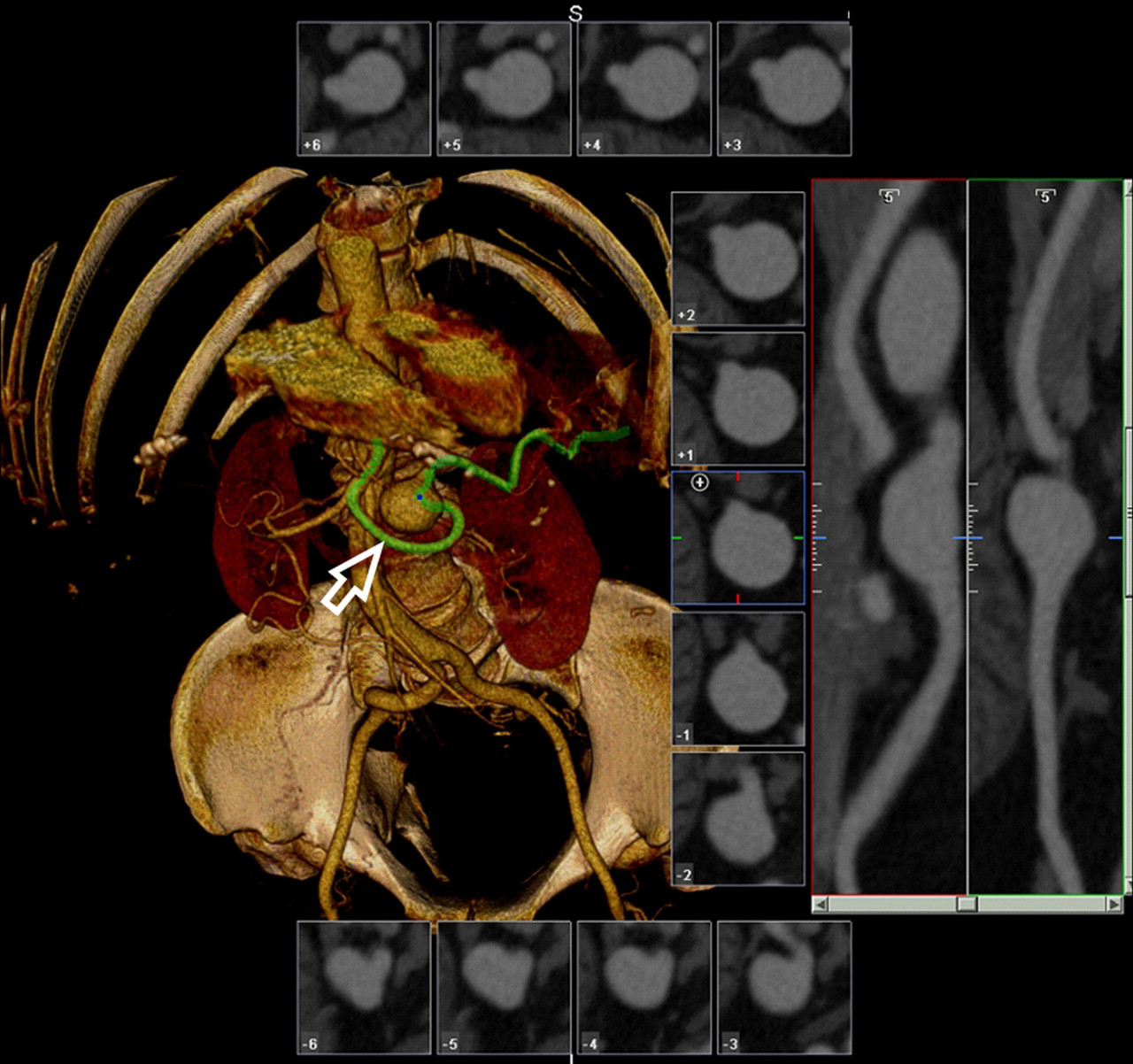
A 61- year-old female patient. Image from workstation that demonstrates the VR and CPR techniques. The VR postprocessed image shows a 2.9 cm splenic artery aneurysm and the green line indicates the splenic artery; the other panels show CPR postprocessing images based on the course of the target artery
MIP
In MIP, the highest CT value along any viewing ray from the desired direction is extracted and projected onto the image. The role of MIP in multidetector-row CT angiography is to generate a DSA-like image and provide an overview of the target vessel (48, 49). In MIP image generation, a viewing angle is chosen to define the projection plane, and then parallel rays are cast from the projection plane through the stack of reconstructed sections that make up the data volume. The maximum intensity encountered along each ray is then placed in the projection plane to create the MIP. A limit in the use of MIP is that mural calcification can obscure the lumen of the splenic artery and aneurysm and hinder the evaluation of mural thrombi.
VR
VR came into use in the late 1980s, and is an advanced computer-intensive rendering algorithm that incorporates all the raw data from MDCT to produce high quality 3D pictures (50–52). VR enables optimum opaque or semi-transparent rendering of the vessels and the surrounding structures and always accurately depicts 3D relationships. This technique is superior to most other 3D rendering and involves the appropriate selection of an opacity curve, which determines how the various contrast-enhanced tissues (depending on their HU value) contribute to the image. A VR reconstruction algorithm can also be adapted in order to segment different tissues based on the attenuation threshold; in addition to conventional anatomic VR algorithms, some vendors offer the option to perform angioscopy-like (virtual angioscopy) VR reconstruction, which generates endoluminal views of the affected vascular segments, allowing useful visualization of the relationship between the arterial lumen and the neck of the aneurysm that can be employed to plan endovascular coiling (Fig. 8).
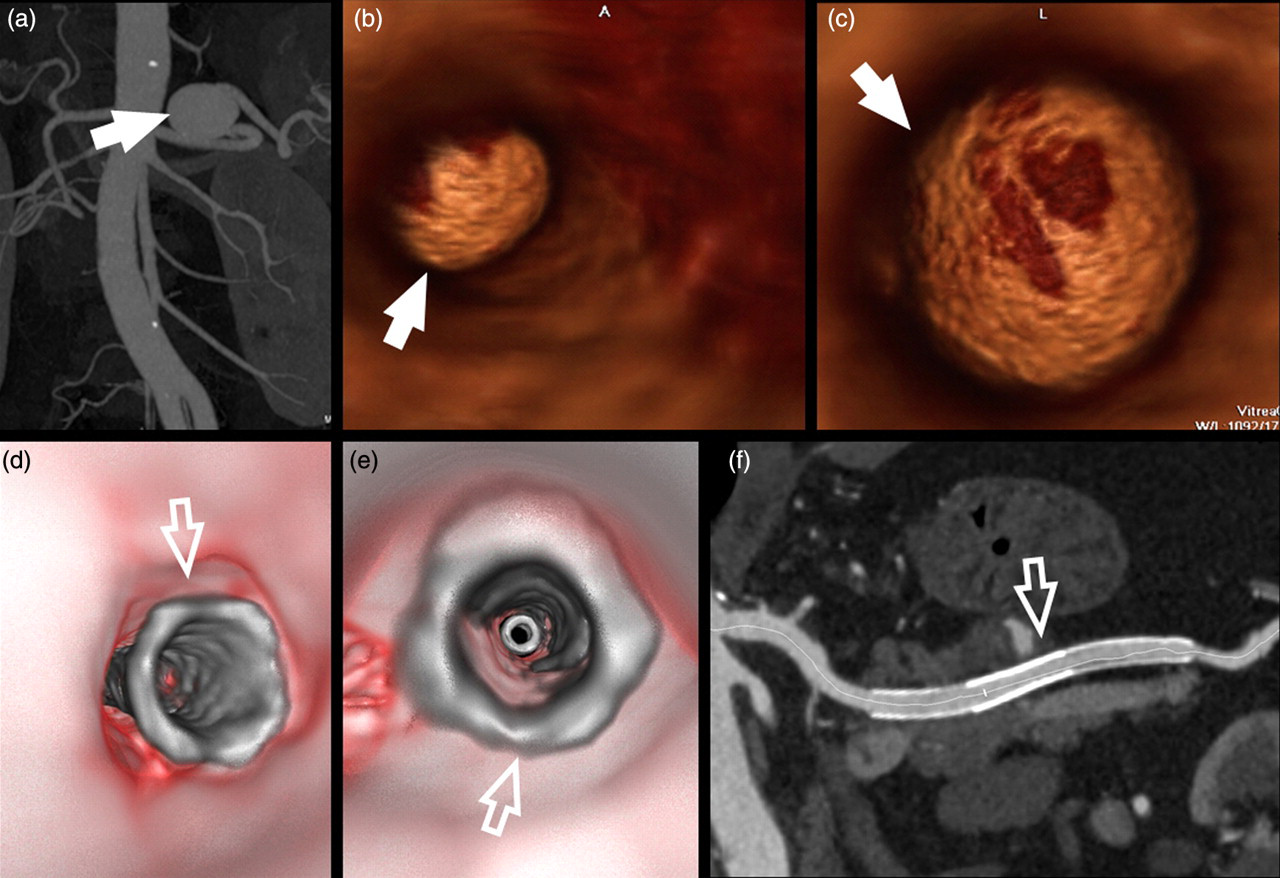
A 57-year-old male patient. The MIP postprocessed image (a) demonstrates a 3.8 cm SAA (white arrow) and VA postprocessed images (b and c) show an endoluminal view of the SAA, allowing visualization of the neck of the aneurysm (white arrow). After the procedure, VA (d and e) showed the stent and its patency, which was confirmed by CPR reconstruction (f) (white open arrows)
In recent years, the use of three-dimensional rotational angiography (3D-RA) has enabled CT-like performance to be obtained for the volumetric evaluation of various vascular regions, including the neck, brain, and abdominal vessels; the main advantage of this approach over conventional subtraction angiography is the ability to perform true multiplanar imaging, allowing VR, MIP, and MPR reconstruction with greater sensitivity for detecting arterial pathology and determining the spatial relationship of the affected segment with the surrounding structures. The use of 3D-RA in the splanchnic region with emphasis on visceral aneurysm intervention has been described previously (53).
MDCTA findings
A true SAA usually appears in MDCTA (8) as a well-defined and homogeneous contrast-enhanced mass; peripheral calcifications or a mural thrombus may also be visible. Two potential pitfalls in the diagnosis of SAA have been reported. The first is misinterpreting a SAA as a solid pancreatic neoplasm (54–56). In fact, endocrine neoplasms of the pancreas can be markedly hyper-attenuating in the arterial phase and therefore SAA can mimic a pancreatic neoplasm. However, with the use of multidetector-row CT systems, and in particular the volume rendering method, this type of mistake can easily be avoided. The second pitfall is due to the marked tortuosity of the splenic artery, which sometimes mimics a SAA; but, even in this case, the use of VR as well as MIP techniques avoids this pitfall. Once a SAA is detected it is important to determine the exact location (proximal, middle of distal splenic artery), size, and potential indicators of rupture in order to plan the optimum therapeutic approach. The choice of surgical procedure is determined by the location of the aneurysm. Aneurysms located in the proximal third of the splenic artery can be removed without resecting the pancreas and/or spleen, providing that the short gastric vessels are also present and sufficient. Alternatively, when SAA are located in the middle third of the splenic artery, proximal and distal ligation of the splenic artery may be attempted. For aneurysms located at the splenic hilum or in the distal third of the artery, the aneurysm is resected with either the spleen or the spleen and left pancreas.
Clinical history can often help to distinguish true SAA from pseudoaneurysms. In the case of pseudoaneurysm of the splenic artery a hyperdense round lesion is typically visible (Yamaguchi et al. [17] reported a mean value of 40 HU), commonly in the pancreatic region, showing focal regions of strong enhancement after administration of contrast material, similar to that of blood vessels. This focal region of strong enhancement may be surrounded by a thrombus or hematoma (8). An intensely enhancing structure within or adjacent to a pseudocyst or contiguous with a pancreatic or peripancreatic artery is highly indicative of a pseudoaneurysm (57).
Discussion
The identification of a SAA is extremely important because its rupture is associated with a high mortality rate (up to 25%) (10, 11, 58). Moreover the SAA should be characterized in order to correctly identify all the parameters required for endovascular treatment (i.e. the size of the neck of the aneurysm, the calibre of the artery immediately before and after the aneurysm). Therefore imaging should: (a) identify the SAA; and (b) characterize the SAA.
There are several imaging techniques that can be used to explore the vascular system: DSA, MRA, sonography, and MDCTA. In the past DSA was considered the gold standard for the identification of SAA since its high temporal and spatial resolution allows the optimal analysis of arterial vascular structures. However, it also suffers important limitations (cost, procedural risk, and biological risk) and thus nowadays the ‘non-invasive approach’ to the diagnosis of vascular pathologies is preferred; the introduction of 3D-RA has increased the potential of angiography but the procedure still remains invasive.
Currently, the gold standard for the non-invasive diagnostic imaging evaluation of SAA is MDCTA. However, MDCTA may not be indicated in the setting of renal failure or a previous anaphylactic reaction to contrast material. Sonography gives poor results in the diagnosis and characterization of SAA because shadowing from bowel gas, obesity and arteriosclerosis may markedly reduce its diagnostic sensitivity; moreover the SAA is sometimes obliterated by overlying stomach gas (33). Sonography detects SAA of large dimensions (>3 cm) with a good level of sensitivity but its sensitivity is suboptimal in the case of SAA <3 cm (59). MRA may play a role in the diagnosis of SAA, in particular for those patients in whom MDCTA may be contraindicated. In 2006 Pilleul et al. (60) compared the use of MRA and CTA for the analysis of splanchnic aneurysms (five SAA) and observed that MRA gave good results; however the number of SAA examined in this study was very small and the authors indicated that the sensitivity of MRA was suboptimal in the case of small aneurysms (<3 cm). Liu et al. (61) obtained very good results in the study of SAA using MRA with contrast material. Three-dimensional contrast-enhanced MR angiography clearly demonstrated the aneurysm's location, size, morphology, and visceral arterial variations, and was superior to DSA in terms of the 3D display of the aneurysm and its relationship with the surrounding vessels and organs (61). However, even in this study the mean diameter of the six aneurysms was large (3.9 cm) and the need to use contrast material was a limitation because of the risk of nephrogenic systemic fibrosis (62–64). MRA suffers several limitations; due to the long time required for the examination, this technique may not be possible in patients with aneurysm clips or pacemakers, in those unable to hold their breath or who suffer from claustrophobia, or in non-cooperative patients. Another drawback is that it is not possible to use MRA to follow up patients who have undergone endovascular treatment because it is not possible to evaluate the patency of the stent.
MDCTA represents an excellent tool for diagnosing SAA and has been established as the method of choice for the diagnosis, treatment planning and follow-up of SAA. In particular, with the introduction of multiple-detector row technology it is possible to obtain an in-plane resolution < 1 mm (Table 2) with the potential to detect even small SAA very easily. The shorter scanning time required for MDCT scanners even permits the study of non-cooperative patients, and besides assessing the location and size of the SAA, MDCTA may also reveal ruptured aneurysms, intra-abdominal hemorrhage, and associated underlying diseases. MDCTA enables collection of all the data necessary for endovascular treatment, and thanks to advanced postprocessing techniques such as VR, MIP, and CPR, it is possible to analyze the shape, dimension, and relationship of the SAA with an exquisite level of detail. Furthermore, this technique is also extremely useful for follow-up after endovascular therapy because MDCTA clearly depicts the stent and its patency (Fig. 5e).
Conclusion
SAA is a common form of visceral artery aneurysm and MDCTA is an extremely useful technique for its diagnosis, enabling differentiation between true SAA and pseudoaneurysms. The use of postprocessing techniques is important for distinguishing SAA from endocrine neoplasms of the pancreas or tortuous vessels.