
Abstract
Backround
Detection of myocardial infarction has been the focus of considerable research over the past few decades. Recently developed dual source computed tomography (DSCT) scanners with dual energy mode have been used to detect myocardial infarction, but the studies on this topic are few.
Purpose
To evaluate the feasibility and performance of dual energy CT (DECT) during arterial phase in coronary CT angiography for the detection of chronic infarction compared with late enhancement MRI (LE-MRI) and histopathology in a porcine model of reperfused myocardial infarction.
Material and Methods
Myocardial infarctions were induced by 30 min occlusion of the proximal left anterior descending coronary artery in eight minipigs. DECT, post-contrast LE-MRI and histopathology were performed 60 days after infarct induction. The CT scan was performed in dual energy mode using a dedicated protocol. Myocardial iodine distribution was superimposed as color maps on grey scale multiplanar reformats of the heart. Two radiologists in consensus interpreted all imaging studies for presence of gadolinium uptake at LE-MRI reduced iodine content at DECT and hypoenhanced areas in the initial 100 kV coronary CT angiography images that were acquired during the DECT-acquisition. Results were compared with histopathology.
Results
Based on evaluable segments, DECT showed a sensitivity and specificity of 0.72 and 0.88; LE-MRI showed a sensitivity and specificity of 0.78 and 0.92; and the 100 kV data-set of the DECT scan showed a sensitivity and specificity of 0.60 and 0.93, respectively, for the detection of histological proved ischemia.
Conclusion
DECT during arterial phase coronary CT angiography, which is ordinarily used for coronary artery evaluation, is feasible for the detection of a chronic reperfused myocardial infarction.
Coronary artery disease (CAD) remains one of the most important causes of morbidity in Western societies (1, 2). Therefore it is crucial to develop a diagnostic technique that is fast, accurate and easy to use for the detection of myocardial infarction. Due to the delayed enhancement of the contrast agent gadolinium diethylenetriaminepentaacetic acid, late enhancement has been successfully imaged with MRI to identify location and extent of myocardial infarction. Late enhancement MRI (LE-MRI) has been clinically used to detect occult infarcts, to identify risk for future cardiac events and to predict functional recovery after revascularization (3–8).
Lately, coronary CT angiography has been shown to be a non-invasive imaging modality for the detection of myocardial infarction in arterial phase coronary CT angiography (9–13) However, it proved surprisingly difficult to predict hemodynamic significance of stenosis based on anatomical data (14–16). One step towards imaging myocardial malperfusion is perfusion CT what is temporally limited due to the limited volume coverage and high radiation dose (17–19).
With the introduction of dual energy CT (DECT) recent research has demonstrated the potential of this technique for the characterization of tissue composition and organ perfusion (20). While early evidence shows that DECT may successfully be applied to contrast-enhanced retrospectively ECG-gated coronary CT angiography (cCTA) for analyzing the iodine signature within the myocardial blood pool, these studies do not include pathological proof of myocardial ischemia as the reference standard (21, 22).
Therefore, the purpose of our study was to evaluate the feasibility and accuracy of in vivo DECT, the initial 100 kV coronary CT angiography images that were acquired during the DECT acquisition and LE-MRI for the assessment of chronic reperfused myocardial infarction using postmortem histopathology as standard of reference.
Material and Methods
Animal model
The study complied with the regulations of the animal care committee of our hospital and the National Institutes of Health publication “Guide for the Care and Use of Laboratory Animals” (1996).
Eight minipigs (Ellegaard, Dalmose, Denmark, 19 months old, 25–34 kg) were included in this study. All examinations were performed under general anesthesia and during continuous ECG monitoring. Pigs were sedated with an intramuscular injection consisting of 33 mg/kg ketamine (Ketavet, Pfizer, Karlsruhe, Germany), 10 mg/kg xylazine (Rompun, Provet AG, Lyssach b. Burgdorf, Germany) and 1.5 mg/kg midazolam (Dormicum, ratiopharm GmbH, Ulm, Germany). Anesthesia was maintained by continuous intravenous injection of 0.75 mg/kg/h midazolam (Midazolam, Ratiopharm, Ulm, Germany) and 10 mg/kg/h ketamine (Ketanest, Pfister, Berlin, Germany). All pigs received an intramuscular injection of 0.01 mg/kg buprenorphine (Temgesic, Essex Pharma, Munich, Germany) for analgesia and four litres of oxygen during all procedures. This protocol was used for the cardiac interventions, final CT and MRI examinations as well.
For cardiac interventions an introducer sheath (Radiofocus Introducer II Fr. 5, Terumo, Tokyo, Japan) was inserted in one of the common carotid arteries. All pigs received 300 mg amiodarone (Cordarex, Sanofi aventis, Gentilly, France) to lower the risk of ventricular fibrillation during cardiac intervention and 5000 IU of heparin (Heparin-Natrium-25000-ratiopharm, Ratiopharm GmbH, Ulm, Germany). In two pigs ventricular fibrillation occurred during cardiac intervention and immediate defibrillation was performed.
Via the introducer sheath a 4-French guiding catheter (Launcher Guiding Catheter .058” JR4.0 100cm, Medtronic GmbH, Meerbusch, Germany) was used to perform a coronary angiogram for visualization of the anatomy of the left coronary artery. A 3-French balloon catheter (Semicompliant Balloon 3.0 × 20 mm, Medtronic GmbH, Meerbusch, Germany) was then placed in the left anterior descending branch (LAD) of the left coronary artery between the first and second diagonal branch. In all animals the balloon was deflated after 30 min of total occlusion. Reperfusion of the vessel was proved by a coronary angiogram. After the cardiac intervention, the pigs were fed with a special diet (Sniff Spezialdiaeten GmbH, Soest, Germany) containing 20% fat and 2% cholesterol.
Immediately after the imaging procedures, the pigs were transported to the dissecting room and euthanized. Following median thoracotomy, the heart was removed along with the pericardium and the adjacent part of the aortic arch in continuity. Subsequently, the pericardium was incised, opened up and removed, and the aortic arch was cut off 5 cm above the aortic valve level. The coronary arteries were dissected in continuity with the aorta and placed in a buffered 4.5% formalin solution. In order to simplify the further processing, the hearts were then wrapped in plastic bags and cooled down for one hour in a –20°C freezer. Afterwards, parallel consecutive short axis cuts were performed with a large-bladed knife using a spacer to obtain uniform 10 mm thick slices. To obtain a viability staining, every 1st, 3rd, 5th, et cetera slice was embedded in a 1% 2,3,5-triphenyltetrazolium chloride (TTC) solution (Sigma Aldrich, St Louis, MO, USA) at 37°C for 15 min (12), followed by fixation in a buffered 4.5% formalin solution for 20 min. Every 2nd, 4th, 6th, et cetera slice was put in a buffered 4.5% formalin solution. All slices were photographed immediately after the respective exposure times to ensure good delineation of TTC-negative areas.
Histological tissue samples were taken from areas with definable or conspicuous TTC-negativity as well as defined areas (right ventricle, anterior and posterior wall of the left ventricle, septum) of each heart. Samples were analyzed using a light microscope (magnification up to 1000×). Presence of fibrous tissue was examined semi-quantitatively with three categories (absent, obvious, scar tissue). Distribution of fibrous tissue was marked in an anatomical as well as radiological segment model of the heart.
Scan protocols and image reconstruction
DECT
All pigs were examined using a retrospective ECG-gated dual source CT system (Somatom Definition, Siemens, Forchheim, Germany). Arterial phase dual energy mode CT acquisition was obtained with the following characteristics: 330 ms gantry rotation time, pitch 0.2, 32 × 2 × 0.6 mm collimation with z-flying focal spot technique and 165 ms temporal resolution (23). One tube of the dual source CT system was operated with 95mAs/rot at 140 kV, the second tube with 165 mAs/rot at 100 kV. A total of 1.5 mL/kg contrast agent iomeprol (Imeron 400, Altana, Konstanz, Germany) was intravenously injected at 4 mL/s and followed by a 40 mL saline chaser bolus. Estimation of individual circulation time was based on the test bolus technique using a 10 mL contrast bolus at a flow rate of 4 mL/s and subsequent injection of a 30 mL saline chaser bolus using dedicated software (DynEva, Siemens, Forchheim, Germany). The peak time of test bolus enhancement as measured by repetitive scanning at the level of the aortic root was used as the delay time.
Angiographic images were reconstructed using retrospective ECG-gating and single-segment reconstruction in best diastolic phase (BestPhase, Siemens, Forchheim, Germany) with a temporal resolution of 165 ms, a slice thickness of 0.75 mm with an increment of 0.4 mm and a medium-soft convolution kernel (B26f).
For the evaluation of myocardial perfusion, images from the same raw data-set were reconstructed with 1.5 mm slice thickness, 1.0 mm increment, a dedicated dual energy convolution kernel (D30f) and information of the full gantry rotation (gantry rotation time of 330 ms). By default, the image reconstruction system generated three stacks of axial images, that is, 140 kV images for the optimization of the spatial resolution, 100 kV images for the optimization of the contrast in the images, and weighted-average images (M_0.3) merging 70% from the 140 kV data and 30% from the 100 kV data to achieve image quality and a signal-to-noise-ratio similar to those of single-energy 120 kV scans. Each image stack (DICOM) could be managed like regular single source single energy images and be loaded into any postprocessing modality.
MRI
MR imaging was always performed subsequent to CT examinations on a 1.5 T whole body MR scanner (Magnetom Avanto, Siemens, Erlangen, Germany) using a phased-array body coil. For assessment of myocardial viability, 5 mm short axis slices without gap were obtained 15 min post injectionem of 0.2 mmol/kg Gd-DTPA (Dotarem, Guerbet, Sulzbach, Germany) using a ECG-triggered, segmented inversion recovery prepared turbo FLASH sequence (TR 9.56 ms, TE 4.38 ms, flip angle 25°, two averages, 25 lines per segment, voxel size 1.25 × 2.5 × 5.0 mm).
Image postprocessing and analysis
The dual energy image series that were specially reconstructed for myocardial evaluation were transferred to a workstation (Syngo MMWP, Siemens, Forchheim, Germany) equipped with dedicated commercially available software (syngo Dual Energy, version VA21 2008G, Siemens, Forchheim, Germany) for the evaluation of myocardial iodine content and distribution and therefore blood perfusion (heart perfused blood volume [heart PBV]). Both, the 100 kV and 140 kV series were loaded simultaneously into the application and were displayed as multiplanar reformats in axial, sagittal, and coronal plane per default. The software uses a three-material-decomposition algorithm based on typical attenuation of iodine, fat, and soft tissue at two different energy levels, i.e. 100 kV and 140 kV. Myocardial iodine content and distribution is displayed as a color map and superimposed onto the gray scale MPR images in the three planes. MPRs and color map can be blended in steps of 1% between MPR gray scale images only and color-coded iodine map only for the simultaneous assessment of morphology and perfusion. Planes were adjusted so that the typical short and long axis views were present. Images were analyzed with a 60% overlay of the iodine map on the MPRs with a slice thickness of 5 mm. Contrast defects on DECT iodine maps were defined as contiguous, circumscribed areas of decreased or absent iodine content within the left ventricular wall, relative to the remainder of the myocardium.
Because in routine cCTA data acquisition is being performed using 100 kV the information on myocardial malperfusion of the 100 kV image stack that was acquired in the dual energy scan was assessed for the presence of enhancement deficits (ED), namely hypoenhanced areas, defined as regions of decreased signal intensity compared with normal myocardium using the typical short and long axis views and a slice thickness of 5 mm. Images were displayed by using a default narrow window-level display (width 150 HU, level 100 HU). However, window center and width were freely adjustable by the observers to better delineate areas of hypoenhanced myocardium.
MR images were examined for the presence of late enhancement, i.e. regions with increased signal compared to normal myocardium.
All images were analyzed by two radiologists in consensus using the AHA 17-segment model of the left ventricle in a random order (24). The observers were experienced in the field of cardiac imaging and blinded to the artery of the induced occlusion and the results of the corresponding imaging data.
Results
A total of 61 ± 4 days after the induction of ischemia all animals underwent DECT with LE-MRI following 50 ± 12 min later. In eight pigs, 136 myocardial segments were evaluated. DECT and MRI scans were conducted without any complications. All studies were diagnostic. Using histology as the reference standard, eight pigs had proven myocardial ischemia in 27 segments. Because of motion or band-like artifacts a median of four segments had to be excluded from analysis of the various CT imaging series (Table 1). In MRI, no myocardial segments had to be excluded due to artifacts.
Results displayed for myocardial segments which were excluded from analysis due to artifacts, and results for positive myocardial segments in DECT heart PBV analysis
Mean weight of the pigs was 42 ± 4 kg. The average radiation dose equivalent that subjects received from the dual-source CT scan in dual energy mode was 5.4 ± 0.8 mSv. The average heart rate in DECT and LE-MRI was 82 ± 8 bpm.
In DECT iodine map analysis, a blood pool deficit was diagnosed in 28 myocardial segments in seven animals. These deficits were located within the left anterior descending coronary artery (LAD) territory.
DECT and LE-MRI showed a sensitivity and specificity of 0.72 vs. 0.78 and 0.88 vs. 0.92, respectively, for the detection of pathological proven ischemia (Table 2). On regular 100 kV grayscale images we observed a sensitivity of 0.60 and a specificity of 0.93 for signs of myocardial ischemia compared to TTC staining (Table 2, Figs. 1 and 2).
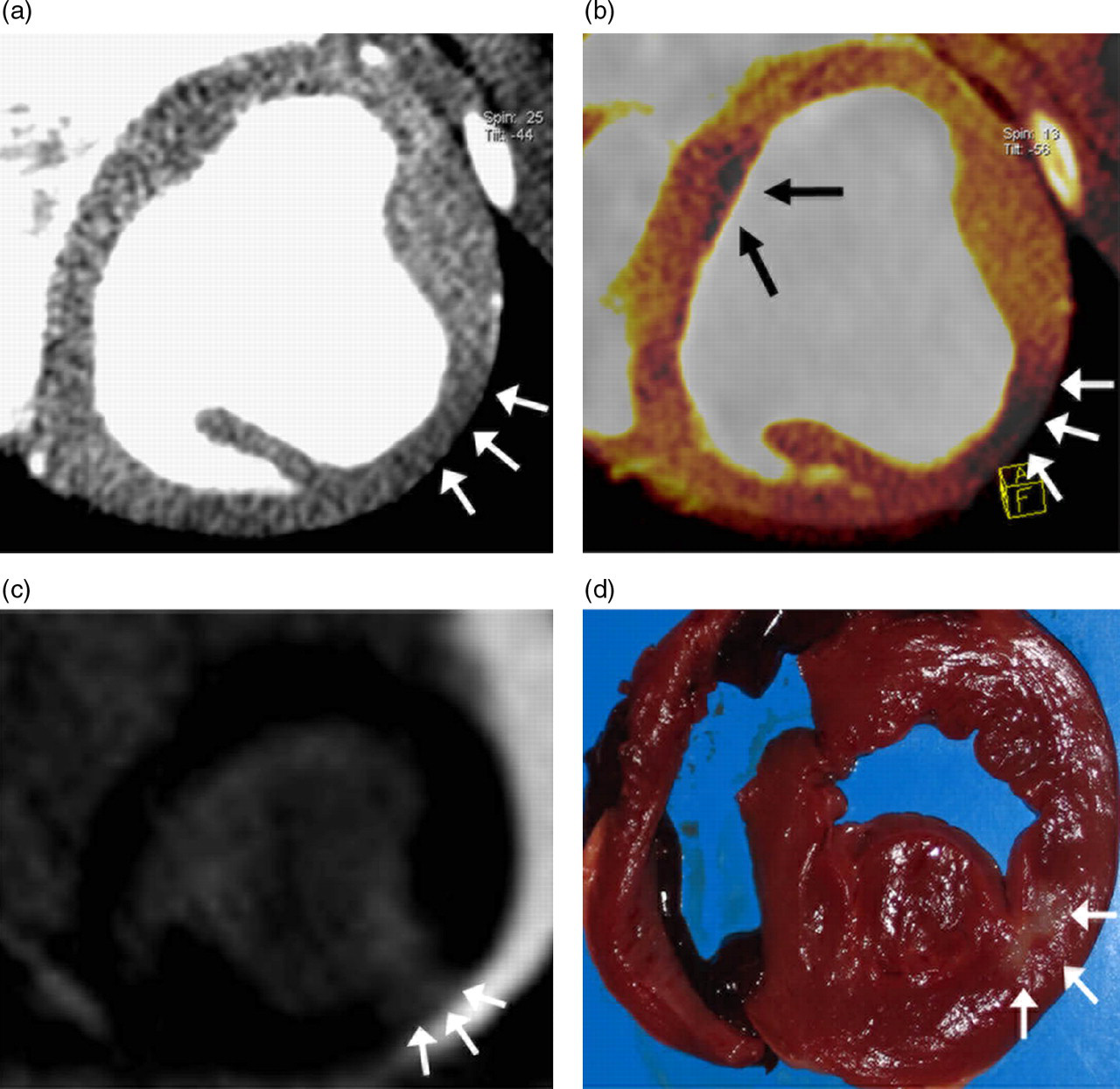
Chronic reperfused myocardial infarction: (a) 100 kV image, (b) DECT heart PBV with a blood pool deficit in the lateral wall (white arrows), (c) delayed enhancement magnetic resonance imaging and (d) ost mortem triphenyltetrazolium chloride (TTC) pathology. Additionally to the blood pool deficit in the lateral wall on (b) a band like artifact is visible in the septal part of the left ventricular myocardium (black arrows)
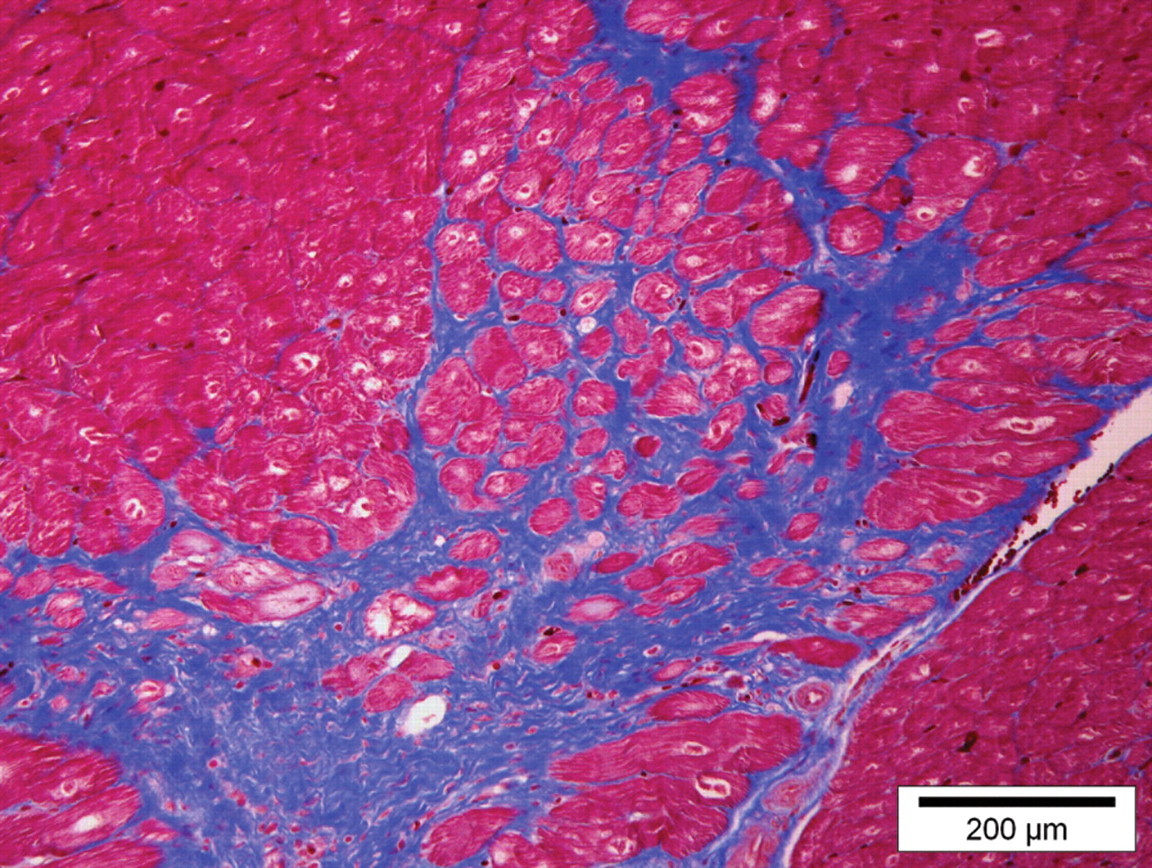
Azan stained tissue sample with scar tissue of the corresponding chronic reperfused myocardial infarction presented in Fig. 1
Results displayed for analysis of the 100 kV images, dual energy myocardial iodine distribution map, i.e. heart PBV and MRI late enhancement for the detection of myocardial scar compared to TTC staining and histopathology per segment
Discussion
Our results demonstrate that a single contrast-enhanced dual energy CT scan is superior to a 100 kV greyscale CT data-set for the assessment of chronic reperfused myocardial infarction with good concurrence to LE-MRI and pathology serving as the reference standard.
The differentiation of viable from infarcted myocardium is important to predict an improvement in the left ventricular function, detect occult infarcts and to identify the risk for future cardiac events (3–6, 8). Given the proven potentials of MDCT to visualize coronary arteries and accurately measure ventricular function, an additional assessment of myocardial viability using MDCT seems to be very attractive in terms of achieving a comprehensive cardiac imaging modality (9, 10, 13, 25).
Previously, Hoffmann et al. reported that MDCT permits the detection and further characterization of acute myocardial infarction in a porcine model (26). Brodoefel et al. also reported about the evaluation of myocardial viability in a reperfused porcine model in acute and subacute infarct stages (27). They both found hypoenhancement in infarcted myocardium during the early-phase scan using contrast-enhanced single source MDCT. However, in the past, studies were concentrating on the myocardial perfusion in acute myocardial infarction only. Recently, Yim et al. investigated the value of a color coded perfusion map in reperfused chronic myocardial infarction. Though, in the investigation of Yim et al. in comparison to our study single energy CT was used to detect reperfused chronic myocardial infarction.
DSCT operated in DECT mode means that the tube voltages are typically set to 140 kV on system A and to 100 kV on system B for cCTA (28). This tube setting comes along with the benefit to generate different energy spectra in dual energy mode (29). Using these two energy spectra DECT exploits the fact that tissues in the human body and the intravascular iodine-based contrast material could be used to enable the mapping of iodine (and thus blood) distribution within the myocardium as a stand-in of myocardial blood volume. DECT therefore uses the opportunity of material differentiation of DSCT in dual energy mode to show myocardial areas of decreased contrast material content (20, 30).
However, our results using DECT were within the range reported by other studies that focused on the detection of healed infarction from a single-phase scan. On a segment-based analysis we calculated a 72% sensitivity, 88% specificity, 62% PPV, and 92% NPV. Ruzsics et al. investigated DECT in humans in comparison to SPECT and found a sensitivity of 92%, specificity of 93%, and accuracy of 93% (22). Another study by Yim et al. reported an accuracy of 94% for the use of a color-coded perfusion map superimposed on a cCTA in a porcine model of reperfused chronic myocardial infarction (31).
Since in DECT routinely a 100 kV image data-set is acquired, we analyzed this data-set for signs of myocardial malperfusion. We found a sensitivity of 60% accompanied by a PPV of 67% for the detection of myocardial malperfusion. In comparison to our results, Kachenoura et al. found a 79% sensitivity, but only 28% PPV (32). They compared myocardial hypoenhancement on first-pass angiographic phase to the results of MPI using SPECT in 89 patients with chronic ischemic heart disease with a regular 120 kV protocol on a 64-slice scanner. This phenomenon might be explained by the relatively short time of ischemia in our subject group, resulting in a smaller area of myocardial minor perfusion compared to this investigation and the relatively high prevalence in the investigated study population. However, in our small subject population we observed a significant improvement of sensitivity and specificity comparing DECT to 100 kV images.
The study has several limitations. Heart rate of pigs is higher than the heart rate of humans and is normally around 95 bpm, which can influence the image quality of the coronary arteries as well as of the myocardium. Due to this high heart rate we had to exclude in median of four out of 17 myocardial segments per piglet because of motion and band like artifacts. In future investigations it therefore might be more appropriate to investigate animals with lower heart rates to avoid motion artifacts. Another limitation of this feasibility study is the relatively small number of piglets and the use of a consensus reading instead of a blinded double reading. Finally we did not perform a comparison analysis for the sizes of the infarcted myocardium for DECT, LE-MRI and TTC staining in this study. However, previous studies demonstrated a good correlation for the size of infarcted myocardium measured by TTC staining and MDCT (12, 26).
In conclusion, our experimental study demonstrates that dual energy CT of the heart is feasible and a promising single imaging modality to assess both vascular obstruction and myocardial ischemia, for the comprehensive diagnosis of coronary artery stenosis and myocardial ischemia. However, future research towards infarct seizes and the systematic determination of the exact performance of DECT compared with the pertinent, respective clinical reference standards is needed to see the actual value of DECT imaging of the myocardium.