
Abstract
Background
Though appropriate image acquisition parameters allow an effective dose below 1 mSv for CT coronary angiography (CTCA) performed with the latest dual-source CT scanners, a single-source 64-detector CT procedure results in a significant radiation dose due to its technical limitations. Therefore, estimating the radiation doses absorbed by an organ during 64-detector CTCA is important.
Purpose
To estimate the radiation doses absorbed by organs located in the chest region during 64-detector CTCA using different acquisition techniques and heart rates.
Material and Methods
Absorbed doses for breast, heart, lung, red bone marrow, thymus, and skin were evaluated using an anthropomorphic phantom and radiophotoluminescence glass dosimeters (RPLDs). Electrocardiogram (ECG)-gated helical and ECG-triggered non-helical acquisitions were performed by applying a simulated heart rate of 60 beats per minute (bpm) and ECG-gated helical acquisitions using ECG modulation (ECGM) of the tube current were performed by applying simulated heart rates of 40, 60, and 90 bpm after placing RPLDs on the anatomic location of each organ. The absorbed dose for each organ was calculated by multiplying the calibrated mean dose values of RPLDs with the mass energy coefficient ratio.
Results
For all acquisitions, the highest absorbed dose was observed for the heart. When the helical and non-helical acquisitions were performed by applying a simulated heart rate of 60 bpm, the absorbed doses for heart were 215.5, 202.2, and 66.8 mGy for helical, helical with ECGM, and non-helical acquisitions, respectively. When the helical acquisitions using ECGM were performed by applying simulated heart rates of 40, 60, and 90 bpm, the absorbed doses for heart were 178.6, 139.1, and 159.3 mGy, respectively.
Conclusion
ECG-triggered non-helical acquisition is recommended to reduce the radiation dose. Also, controlling the patients’ heart rate appropriately during ECG-gated helical acquisition with ECGM is crucial.
Keywords
Sixty-four-detector CT coronary angiography (CTCA) provides a high diagnostic accuracy in assessing coronary artery diseases (1). However, perceptions concerning cancer risks associated with CTCA persist (2). Though appropriate image acquisition parameters may allow an effective dose below 1 mSv for CTCA performed with the latest dual-source CT scanners (3), a single-source 64-detector CT needs a significant radiation dose due to its technical limitations (overlap acquisition, limited temporal resolution, and using low pitch factor).
CTCA is classified into three acquisition techniques: retrospective electrocardiogram (ECG)-gated helical acquisition; retrospective ECG-gated helical acquisition with ECG modulation (ECGM) of the tube current; and prospective ECG-triggered non-helical acquisition (4). In retrospective ECG-gated helical acquisition, the radiation doses differ between patients because appropriate acquisition parameters (pitch factor and tube rotation speed particularly) differ between these patients depending on their heart rates. Radiation doses during ECGM also differ for every patient as the duration acquired with full tube current depends on individual heart rates and differs slightly each time, provided all acquisition parameters are identical. In a previous study, prospective ECG-triggered non-helical acquisition was associated with a lower volumetric CT dose index (CTDIvol) and an equivalent image quality compared with ECG-gated helical acquisition with ECGM (5). The CTDIvol is the most common parameter used to estimate the approximate radiation doses received by organs in clinical situations (6), but specific values of the doses absorbed by organs during CTCAs cannot be estimated.
This study aimed to estimate the radiation doses absorbed by organs located in the chest region during CTCAs with different acquisition techniques and heart rates by using an anthropomorphic phantom and small radiophotoluminescent glass dosimeters (RPLDs).
Material and Methods
CT system and phantom
A 64-detector CT LightSpeed VCT (GE Healthcare, Milwaukee, WI, USA) was used. The effective energy at 120-kV tube voltage was 49.3 keV as measured using the aluminum absorption method.
The RAN-110 (Phantom Laboratory, Salem, NY, USA) anthropomorphic female thoracic phantom on to which two breast sections were mounted was used (Fig. 1). The assembly has an embedded natural skeleton, an epoxy resin-based lung substitute, and an isocyanate rubber-based muscle substitute (7).
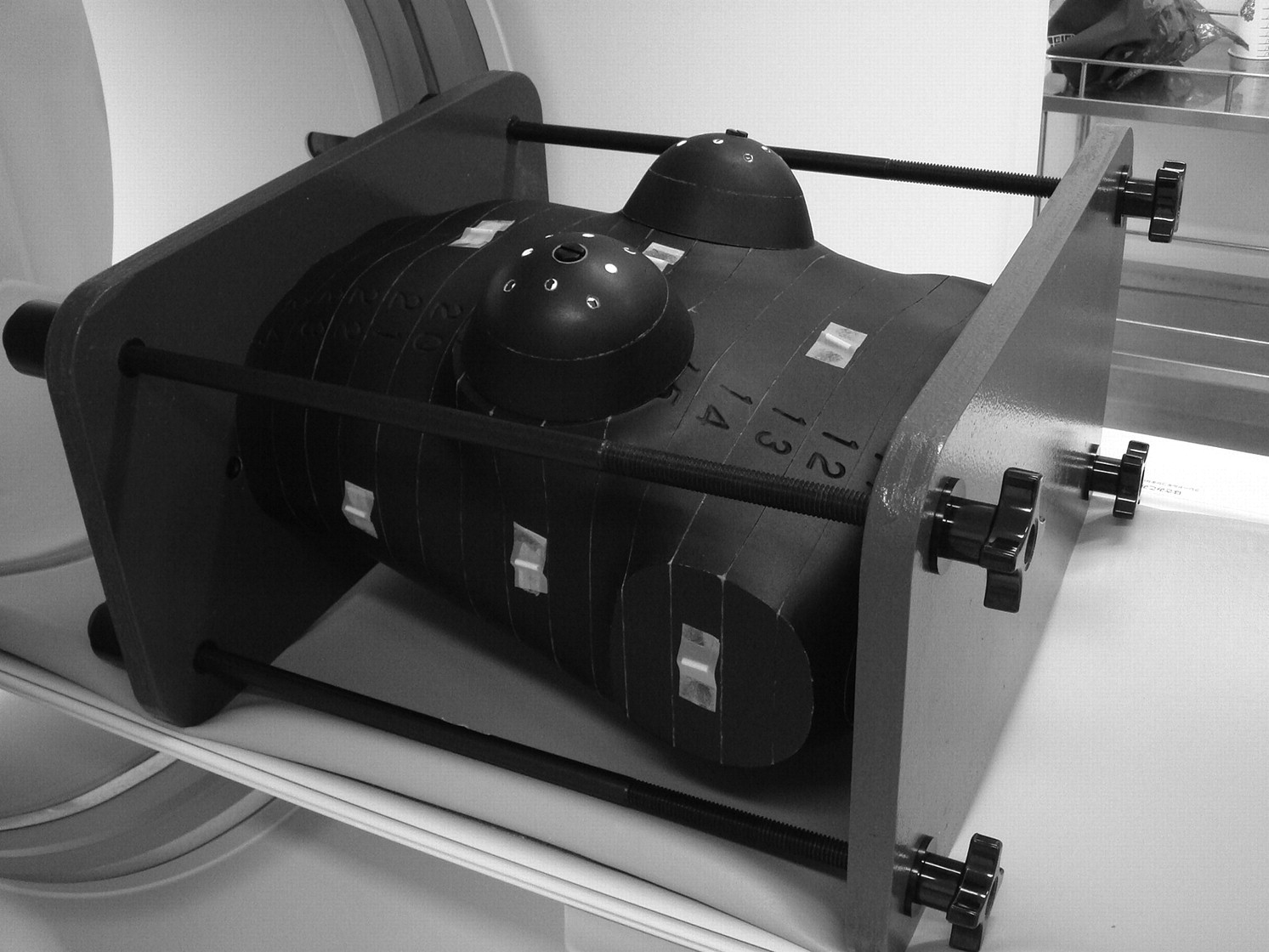
The anthropomorphic female thoracic phantom used in this study. The entire phantom is cut into thin transverse sections with grids of holes for placing small dosimeters
Dosimeters and dose calibration
RPLDs (GD-302M; Chiyoda Technol, Tokyo, Japan) were used in this study to estimate the radiation dose absorbed by the organs. The RPLDs had 1.5 mm diameter and 12 mm length. According to the basic characteristic data of RPLDs provided by the manufacturer (8), the variation in sensitivity between RPLDs is approximately ≤2% with ≥1 mGy of 137Cs-gamma irradiation, and the reproducibility of RPLDs is ≤1% with ≥0.1 mGy when the same RPLD is read out 10 times at the same readout position. However, the scatter from RPLDs may possibly cause over-estimation of radiation doses. Dose calibration was performed against an ionizing dosimeter (Ramtec 1500B; Toyo Medic, Tokyo, Japan) with a 3-cm3 ion chamber adjusted to a 120-kVp (effective energy 50 keV) diagnostic X-ray beam. The chamber and RPLDs were placed side by side at the same distance from the X-ray focus in an irradiated field. The ionizing dosimeter had been calibrated at a laboratory accredited by the Japan Quality Assurance Organization. The RPLDs were annealed at 400°C for 30 min before each exposure. After each exposure, the RPLDs were further heated to 70°C for 30 min and read using a FGD-1000 reader (Chiyoda Technol, Tokyo, Japan) in accordance with the manufacturer's recommended protocol.
Measurement of absorbed dose
After obtaining localizer radiographs, the relative positions of the four corners of the phantom were marked on the bed using tape and a felt-tip pen to maintain the phantom in the same position for subsequent CTCA acquisitions, and the phantom was taken off the bed. Then 48 RPLDs were placed at locations corresponding to the breast (six RPLDs), heart (eight RPLDs), lungs (eight RPLDs), red bone marrow within the ribs, sternum, thoracic vertebrae (six, two, and four RPLDs, respectively), thymus (two RPLDs), and skin (12 RPLDs). Thereafter, the phantom was replaced on the bed using the reference marks previously made. These procedures were performed to exclude the dose of localizer radiographs from the results. Two RPLDs were used to measure background radiation.
Thereafter, ECG-gated helical acquisitions with and without ECGM (ECG mA Modulation, GE Healthcare, Milwaukee, WI, USA) and ECG-triggered non-helical acquisition (SnapShot Pulse, GE Healthcare, Milwaukee, WI, USA) at a simulated heart rate of 60 beats per minute (bpm) were performed. Exposure parameters using the lowest pitch factor or the longest padding time are indicated in Table 1. A cardiac trigger monitor model 3100 (IVY Biomedical Systems, Branford, CT, USA) was used to simulate an arbitrary heart rate. ECG-gated helical acquisitions were then performed using ECGM at simulated heart rates of 40, 60, and 90 bpm. Exposure parameters (Table 2) were chosen in accordance with manufacturer recommendations. Each measurement was performed twice with two separate sets of RPLDs to achieve accurate RPLD readings.
Acquisition parameters using the lowest pitch factor or the longest padding time when electrocardiogram (ECG)-gated helical acquisitions with and without ECG modulation and ECG-triggered non-helical acquisition at a simulated heart rate of 60 bpm were performed for measurement of absorbed dose
*The ratio of the distance the table travels per X-ray tube rotation to the X-ray beam width
†Extra active tube current time to acquire image data during additional cardiac phases ECGM = electrocardiogram-gated modulation; kV = kilovolt; N/A = not applicable; mA = milliampere; FOV = field of view; CTDIvol = volumetric CT dose index
Acquisition parameters in accordance with manufacturer recommendation when electrocardiogram (ECG)-gated helical acquisitions with ECG modulation were performed at simulated heart rates of 40, 60, and 90 bpm for measurement of absorbed dose
*The ratio of the distance the table travels per X-ray tube rotation to the X-ray beam width Bpm = beats per minute; kV = kilovolt; mA = milliampere; FOV = field of view; CTDIvol = volumetric CT dose index
Subsequently, the absorbed dose for each organ was calculated by multiplying the calibrated mean dose values obtained from the reader with the mass energy coefficient ratio of each organ to air (9). The coefficient of lymph nodes was substituted for that of the thymus.
Absorbed dose distribution within a single section
ECGM is independent of the individual body shape and depends on the cardiac cycle of each patient. Therefore, the timing of modulation between multiple acquisitions is different, and may influence the dose distribution of each acquisition. The absorbed dose distribution within one section (section no. 20; Fig. 2) was examined when ECG-gated helical acquisitions were performed.

The section where absorbed dose distribution was examined: (a) the location of the section (arrow) in the frontal localizer radiograph; (b) photograph of the section
After obtaining localizer radiographs, 31 RPLDs were placed within all holes of the section and 12 RPLDs were pasted around the section. Thereafter, the ECG-gated helical acquisition with ECGM was performed with the parameters indicated in Table 1. Simulated heart rate of 60 bpm was applied and distribution measurement was performed three times with three separate sets of RPLDs. ECG-gated helical acquisition without ECGM was then performed once using the parameters indicated in Table 1. The heart rate was simulated at 60 bpm in this case as well.
Absorbed doses within the phantom were calculated by multiplying the calibrated dose values that were obtained from the reader by the mass energy coefficient ratio of soft tissue to air; surface-absorbed doses were calculated by the mass energy coefficient ratio of skin to air (9, 10). A graph of each absorbed dose distribution was drawn using graph-creating software (ORIGIN 8.1; OriginLab, Northampton, MA, USA).
Results
Difference in organ absorbed-radiation doses according to each acquisition type
Fig. 3 indicates the differences in organ absorbed-radiation doses between ECG-gated helical acquisitions with and without ECGM, and ECG-triggered non-helical acquisition at a simulated heart rate of 60 bpm. ECG-gated helical acquisition with ECGM could reduce 6.4% (3.4–9.2%) of doses absorbed by the thoracic organs compared with ECG-gated helical acquisition without ECGM, and ECG-triggered non-helical acquisition could reduce 68.1% (66.1–71.0%) of doses absorbed by the thoracic organs compared with ECG-gated helical acquisition with ECGM. The standard deviations of absorbed doses for the lungs, red bone marrow, and skin were relatively high because these organs have a large volume, and the whole of these organs were not included within the acquisition range.
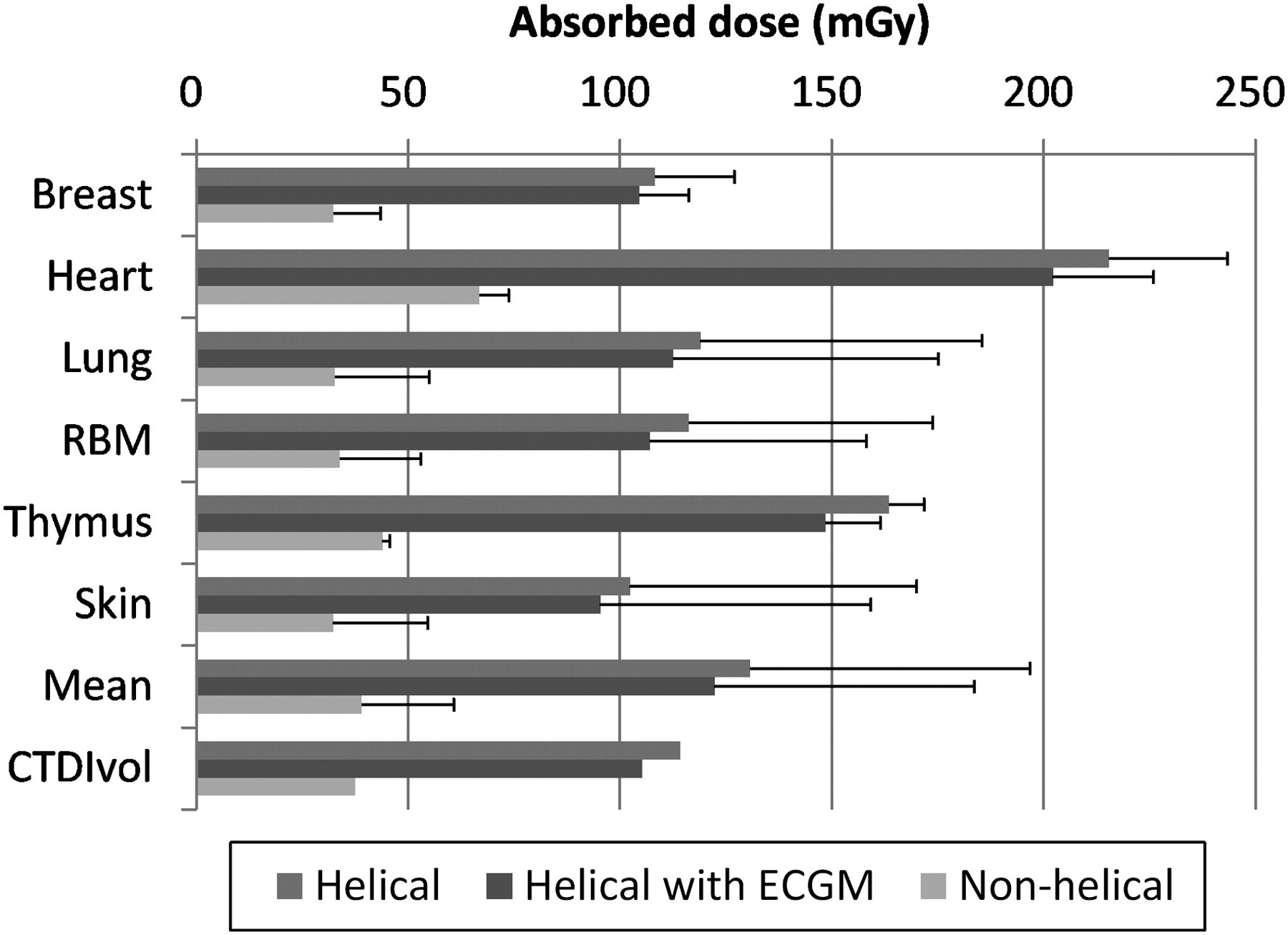
The organ absorbed-radiation doses using electrocardiogram (ECG)-gated helical acquisitions with and without ECG modulation (ECGM) and ECG-triggered non-helical acquisition at a simulated heart rate of 60 bpm. Each bar represents the average dose of multiple radiophotoluminescent glass dosimeters (RPLDs) in two acquisitions. Error bars are 2 × the standard deviation
Difference of organ absorbed-radiation doses according to each heart rate
Fig. 4 indicates organ absorbed-radiation doses when ECG-gated helical acquisitions were performed using ECGM at simulated heart rates of 40, 60, and 90 bpm. The radiation doses absorbed by thoracic organs were 30.2% (27.8–34.8%) and 10.6% (2.2–14.5%) for acquisitions performed at 40 and 90 bpm, respectively, which were higher than those at 60 bpm.
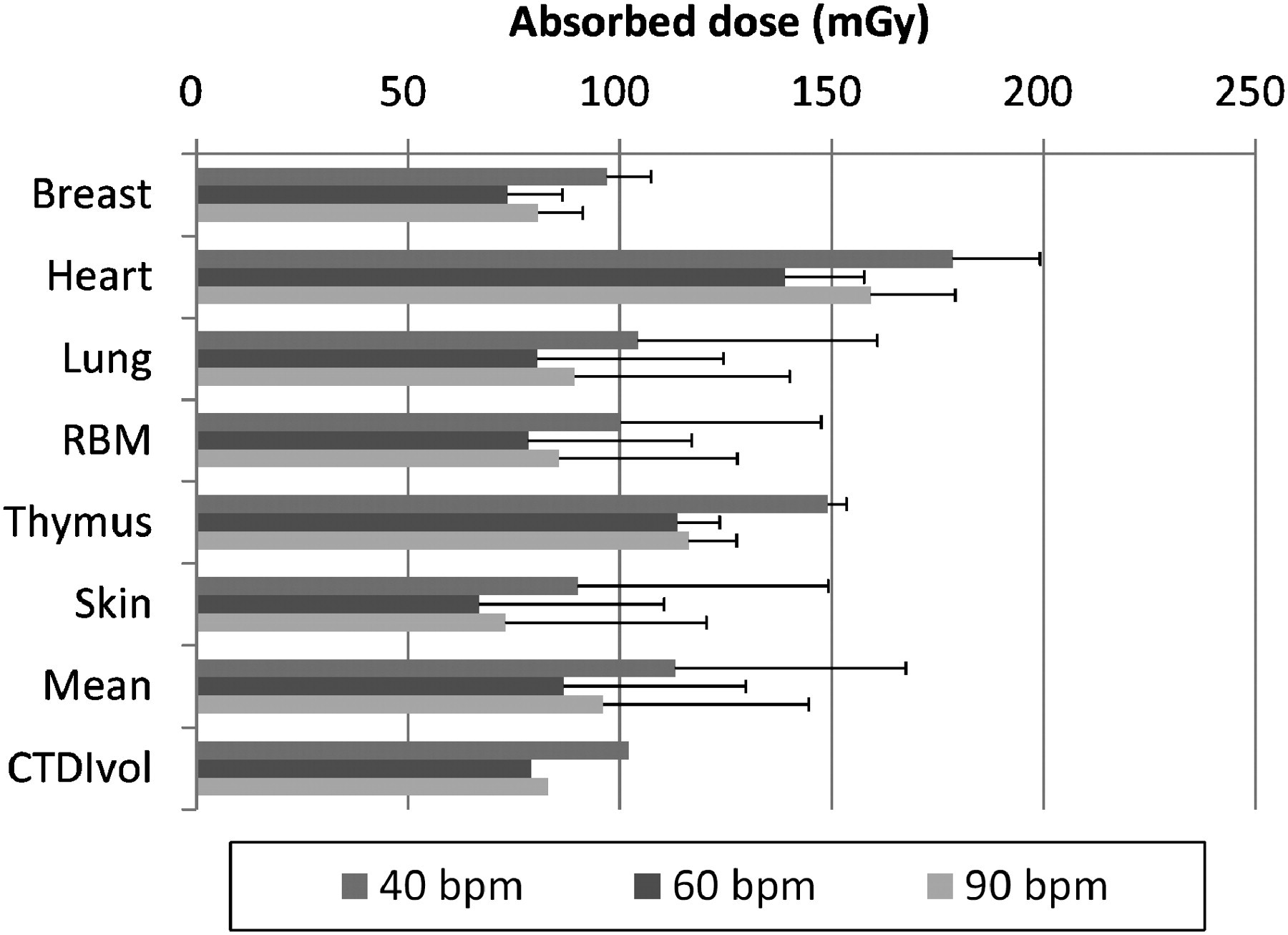
The organ absorbed-radiation doses using electrocardiogram (ECG)-gated helical acquisitions with ECG modulation (ECGM) at simulated heart rates of 40, 60, and 90 bpm. Each bar represents the average dose of multiple radiophotoluminescent glass dosimeters (RPLDs) in two acquisitions. Error bars are 2 × the standard deviation
Absorbed dose distribution of the section investigated
Fig. 5 shows absorbed dose distribution within a single section when ECG-gated helical acquisitions were performed with and without ECGM. The absorbed dose distribution differed among the acquisitions, especially during the second acquisition. The tendency of absorbed dose distribution averaged from the first to third acquisitions with ECGM was almost similar to that without ECGM. For acquisition without ECGM, absorbed doses for all measured points ranged from 1.8 to 30.8 mGy greater than those with ECGM.
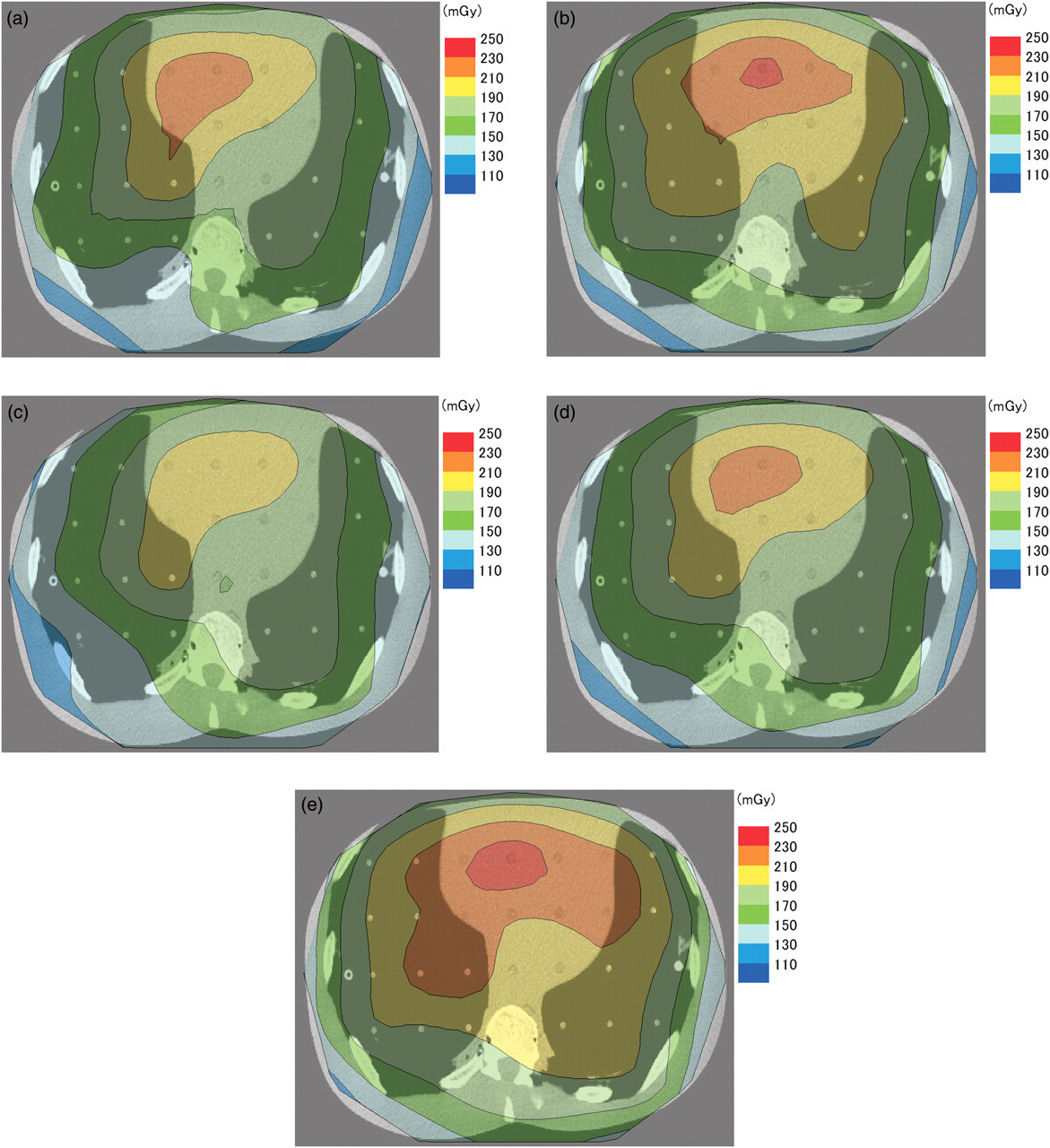
The absorbed dose distribution within the section using electrocardiogram (ECG)-gated helical acquisitions with (a–d) and without (e) ECG modulation (ECGM): (a) the first distribution with ECGM; (b) the second distribution with ECGM; (c) the third distribution with ECGM; (d) the distribution averaged from the first to third acquisitions with ECGM; (e) the distribution without ECGM
Discussion
Our study estimated the radiation doses absorbed by thoracic organs during 64-detector CTCA using different acquisition techniques and heart rates. Absorbed-radiation doses are different according to the acquisition technique and heart rate in CTCAs. Moreover, the absorbed dose distribution differed between each acquisition with ECG-gated helical acquisition with ECGM, even for the same acquisition parameters.
In our study, the dose reduction rate was lower than those reported by other authors (28% and 47%) (11, 12) when ECGM was applied. However, absorbed doses can certainly be reduced by ECGM, and it should be applied unless the patient has existing severe arrhythmia. In addition, Wu et al. (5) reported that ECG-triggered non-helical acquisition could reduce 61.4% of the CTDIvol compared with ECG-gated helical acquisition with ECGM, and Ko et al. (13) reported that ECG-triggered non-helical acquisition could reduce 64.2% of the effective dose compared with ECG-gated helical acquisition with ECGM. These findings accompanied by those from our study recommend adopting ECG-triggered non-helical acquisition as the best technique for reducing absorbed-radiation doses. However, a low heart rate is crucial for obtaining optimum image quality.
Increasing pitch factor reduces the radiation dose when the other parameters remain the same. The pitch factor is recommended to increase when heart rate increases in order to avoid discontinuity in the anatomic coverage of the heart between images from consecutive cardiac cycles in most CT systems (14). Therefore, the highest absorbed dose for each organ of three heart rates examined was at 40 bpm. The recommended acquisition parameters were the same for 60 and 90 bpm except for the reconstruction mode in our study, but the absorbed dose for each organ at 90 bpm was higher than that at 60 bpm. As the frequency of modulation is believed to influence the radiation dose, controlling the heart rates of the patients is crucial to reduce the absorbed dose.
Conversion factors from the CTDIvol to the absorbed dose for each organ as calculated from our results are shown in Table 3. The conversion factors were calculated by dividing each CTDIvol by the absorbed dose for each organ, obtained with different acquisition techniques and heart rates. Huda et al. (15) showed the conversion factors from CTDIvol to absorbed dose for each organ when chest CT examinations were performed using a CT dosimetry phantom and simulation software. However, estimating accurate organ doses by using simulation software in CTCA examinations is difficult, because it needs specific beam-shaping filters and applications that are not built into the software.
Conversion factors from volumetric CT dose index to the absorbed dose for each organ calculated from our results (average ± standard deviation)
RBM = red bone marrow
Our study has several limitations. First, a specific CT system and a specific anthropomorphic phantom were used. Therefore, similar examinations using other CT systems as well as other anthropomorphic phantoms should be performed. Second, although a limited number of RPLDs were evenly distributed at a location that corresponded to each organ, the obtained and actual radiation doses absorbed by each organ could differ. Third, only limited heart rates were applied; hence, no data were available for other heart rates. Finally, image quality was not evaluated with each acquisition. Incidentally, Gerber et al. (12) reported that noise in images reconstructed during ventricular systole was double than that in images reconstructed during ventricular diastole when ECG-gated helical acquisition with ECGM was performed.
In conclusion, absorbed-radiation doses differ according to the acquisition techniques and heart rates in CTCAs. For reducing patient dose, ECG-triggered non-helical acquisition should be adopted first whenever possible, and the heart rate of the patient should be controlled appropriately if ECG-gated helical acquisition with ECGM is adopted.
Footnotes
Acknowledgment
This work was supported by MEXT KAKENHI (21791175).