
Abstract
Background
New or worsening bone lesions in patients responding to treatment, known as the flare phenomenon is well described on 99mTc-MDP bone scintigraphy, but to our knowledge has not previously been described on CT. The appearance of new or worsening bone sclerosis on CT in patients with prostate cancer may therefore be erroneously classified as disease progression.
Purpose
To assess the incidence of osteoblastic healing flare response at 3-month CT assessment in patients with castrate-resistant prostate cancer and to identify associated features that enable differentiation from progressive metastatic bone disease at 3 months.
Material and Methods
CT scans of 67 patients with castrate-resistant prostate cancer undergoing treatment were reviewed by a radiologist blinded to clinical outcome. Changes in number, size, and density of metastatic bone lesions were documented and Response Evaluation Criteria in Solid Tumours (RECIST) in soft tissue lesions, alkaline phosphatase, prostate specific antigen, and 99mTc-MDP bone scans were used for correlation.
Results
Of the 39 patients who had 3- and 6-month follow-up, eight patients (21%) demonstrated an increase in number, size, or density of sclerotic lesions on the 3-month CT scan despite improvement in PSA and soft tissue lesions. Three out of eight patients (8%) maintained partial response/remained stable at follow-up and were defined as showing a flare response: in this group bone metastases evident on CT showed a qualitative and quantitative increase in density and no lesions faded at 3 months. In contrast, in all patients who progressed at 3 months by PSA/RECIST criteria (n = 8) bone lesions showed a mixed pattern with some lesions increasing and others decreasing in density.
Conclusion
The incidence of flare response of metastatic bone disease evident at 3-month post-treatment CT in patients with prostate cancer undergoing systemic treatment is 8%. In patients with falling PSA and stable/responding soft tissue disease at 3 months an increase in bone sclerosis in the absence of fading bone metastases can be interpreted as flare and is likely to represent a response.
In castrate-resistant prostate cancer (CRPC) bone is the first site of relapse in more than 80% of cases when biochemical progression occurs (1). CT is routinely used in clinical trials to assess disease response although updated Response Evaluation Criteria in Solid Tumours (RECIST) guidelines classify osteoblastic metastases as non-measurable (2). Also, the appearance of a new osteoblastic lesion on conventional imaging at 3 months may result in disease being classified as unequivocal progression even though this may represent the flare phenomenon, i.e. ‘healing’ of a previously occult metastasis. Flare has been described on 99mTc-MDP bone scintigraphy (3, 4), and when the possibility of flare at 3-month 99mTc-MDP bone scintigraphy is raised, a 6-month follow-up is used to confirm this finding. For this reason, the first post-therapy assessment by 99mTc-MDP bone scintigraphy is often delayed to 6 months. However, as CT is the primary modality in clinical trials, development of robust CT interpretation of bone lesions at 3 months in patients with CRPC would facilitate assessment of time to progression and progression free survival. Therefore, the aim of this study was to assess the incidence of osteoblastic healing flare response at 3-month CT assessment in patients with CRPC, and to identify features that enable differentiation of flare from progressive metastatic bone disease.
Material and Methods
Study subjects
This single institution study was approved by the local research ethics review committee. All patients with castrate- resistant prostate cancer entering into a phase II clinical trial of a CYP17 inhibitor were included (n = 67; mean age 70 years; range 49–88 years).
Imaging technique
Contrast-enhanced CT of the chest, abdomen and pelvis was done at baseline and at 3-month intervals until discontinuation of treatment. CT scans were performed on a 16-slice GE Lightspeed (GE Healthcare Technologies, Waukesha, WI, USA). Images were obtained at portovenous phase using 100 mL Omnipaque® 300 mg/mL at 3 mL/s (GE Healthcare, Cork, Ireland). We used Smartprep technique, slice thickness of 1.25 mm with 5 mm reconstructions. Whole body 99mTc MDP bone scans were performed at baseline and at 6-month intervals until discontinuation of treatment. Scans were performed 3 h following intravenous injection of 600MBq 99mTc-MDP using dual-headed gamma cameras with high resolution collimators and a scan table speed of 10 cm per minute (energy peak was 140 keV with a 20% window). Images were reviewed on dedicated workstations.
Data analysis
Baseline, 3- and 6-month CTs were assessed by a radiologist with 9 years of experience of oncologic imaging. He/she was blinded to other investigations and outcome: RECIST assessment of soft tissue disease (5) and presence or changes in number, size or density (qualitative) of metastatic bone disease were documented at 3 months and RECIST assessment of soft tissue disease was repeated at 6 months. In addition to this at baseline and 3 months, regions-of-interest were drawn around up to six lesions per patient and mean Hounsfield Unit (HU) documented: 1 in T4, T7, T10, L1, L4 and in the pelvis where possible. The presence of metastatic bone disease at baseline was confirmed by assessing baseline CT and 99mTc-MDP bone scans. Following blinded CT assessment, monthly Prostate Specific Antigen (PSA) and 6-month 99mTc-MDP bone scans were used for correlation. Flare response at 3-month CT scan was defined as new bone sclerosis or sclerotic lesions increasing in size or density together with stable or responding soft tissue disease, a PSA decline confirmed at PSA measurement one month later (6) and no evidence of progression at the following 6-month CT or 99mTc-MDP bone scan.
Changes in number, size, or density (qualitative and quantitative, Hounsfield Units of up to six lesions per patient) of bone metastases in the flare group at 3-month CT were compared to those in patients who progressed at 3 months (by PSA/RECIST criteria) to identify associated features which enable differentiation of flare from progressive metastatic bone disease at this time point.
In patients with worsening bone sclerosis but also showing PSA/RECIST response at 3 months or soft tissue response (by RECIST), changes in number/size/density of sclerotic lesions and alkaline phosphatase (ALP) were measured and compared in order to identify discriminating features between those who showed a continued PSA and soft tissue response at 6 months, i.e. flare, and those that progressed at next assessment.
Statistical methods
The data were tested for normality using the Kolmogorov-Smirnov test and changes in the density of bone metastases were tested for significance using paired t tests.
Results
Eighty-two percent (55/67) of patients had metastatic bone disease and 28% (19/67) of patients had bone as the only site of disease. Sixty-one of 67 patients had a baseline and 3-month CT scan; 39 of 67 patients had CT at both 3 and 6 months and therefore were eligible for assessment of flare response. For the remaining 28 patients, 22 had CT scans at 3 months, eight of whom clearly progressed by PSA/RECIST criteria and therefore did not continue on study. The remainder of patients were unable to continue on study due to toxicity or concurrent medical conditions, i.e. ischaemic heart disease.
Of the 39 patients who had baseline, 3- and 6- month CT scans, eight (21%) demonstrated new sclerotic lesions or sclerotic lesions increasing in size or density on the 3-month CT scan discordant to PSA/RECIST response. Of the eight patients with imaging/biochemical discordance, three maintained partial response/remained stable at follow-up by PSA and RECIST criteria and were defined as showing a flare response (Figs. 1 and 2). The remaining five patients had signs of progression at the next assessment and therefore it was difficult to determine whether the bone changes at 3 months represented flare or an early sign of progression. New sclerotic lesions were seen both in flare (2/3, 67%) and progressing patients (3/8, 38%).

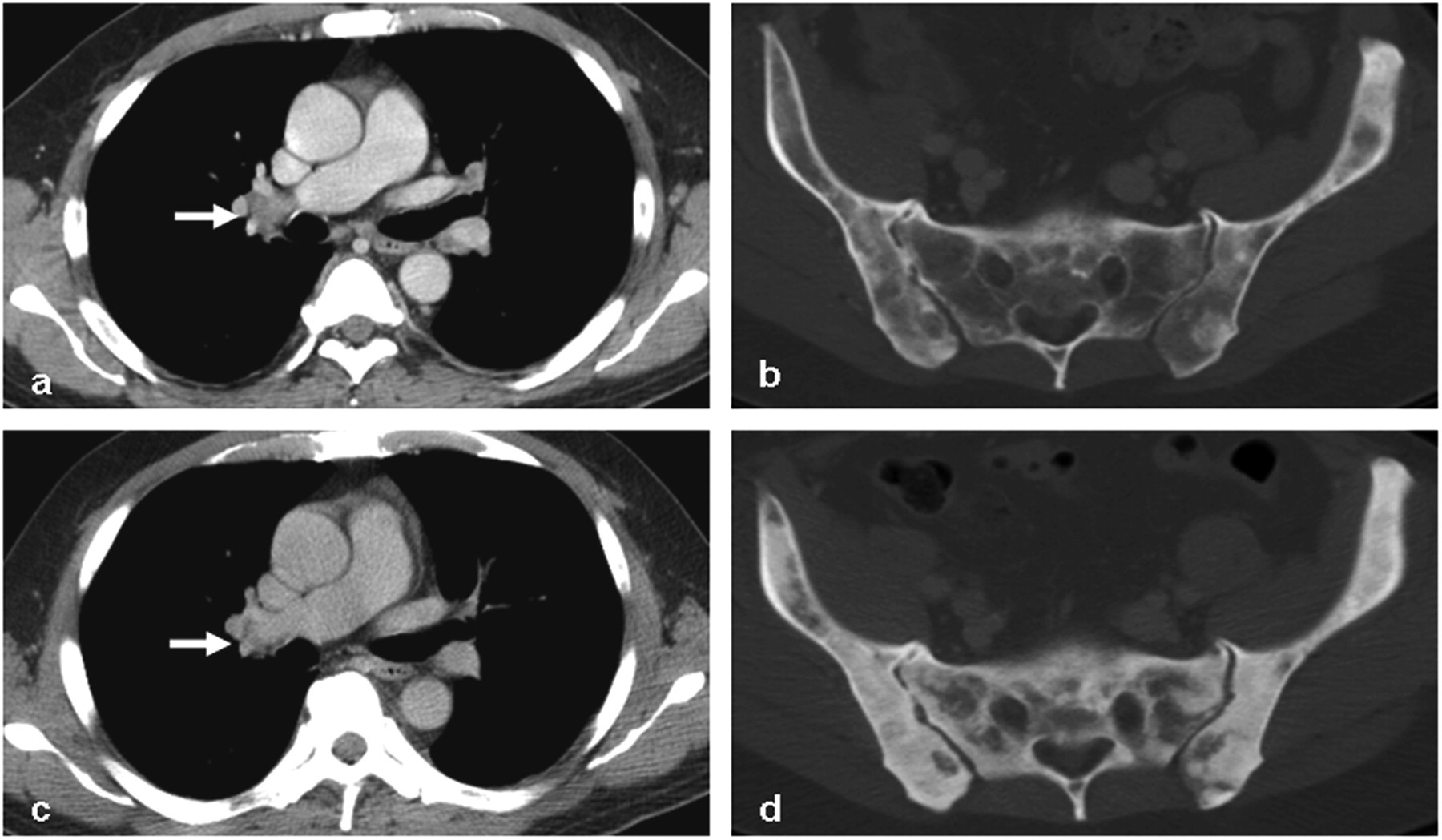
A 73-year-old man with CRPC and CT flare response. Axial CT through chest (a) and pelvis (b) before and 3 months after (d and e, respectively) treatment with corresponding 99mTc-MDP bone scan before (c) and 6 months after (f) treatment. Left axillary lymphadenopathy (a) reduced after treatment (b, arrows) and PSA fell from 271 to 58 ng/mL. Bone windows in B and E demonstrate an increase in bone sclerosis (arrows) with corresponding reduction in osteoblastic activity (f, arrows)
A 48-year-old man with CRPC and flare response on CT. Axial CT through mid chest (a) and pelvis (b) before and 3 months after (c and d, respectively) treatment show a soft tissue response of lymphadenopathy at the right hilum (arrows). PSA fell from 37.6 to 3.9 ng/mL. A diffuse increase in bone sclerosis is seen in (d)
In the flare group (n = 3) all bone metastases evident on CT showed a qualitative and quantitative increase in density and none of the lesions decreased in density at 3 months: HU of 16 bone metastases were measured and mean HU increased from 471 to 643 HU (P < 0.001). In the five patients with bone metastases increasing in size/number/density at 3 months in context of falling PSA/RECIST response but subsequent progression at 6 months, the Hounsfield units of 14 lesions at 3 months increased from 404 to 586 HU (P < 0.001). In contrast, in those who clearly progressed at 3 months by PSA/RECIST criteria (n = 8), bone metastases showed a mixed pattern with some lesions increasing (Fig. 3) and others decreasing in density (Fig. 4) at 3 months: Mean HU of 37 lesions fell from 596.7 to 578.1HU (P = 0.081).
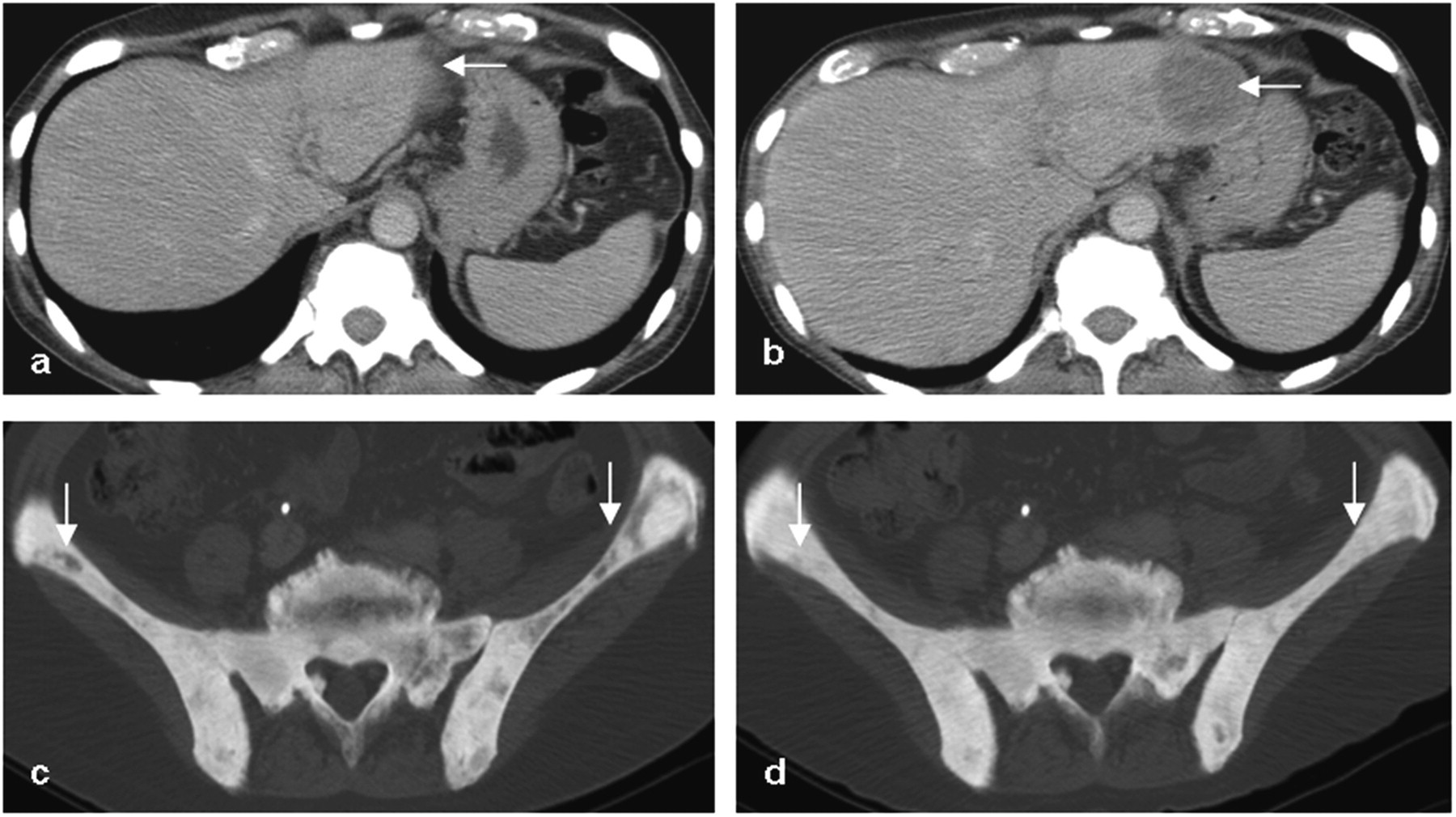
A 65-year-old man with CRPC and osteoblastic progressive bone lesions. Axial CT through the upper abdomen pelvis before (a, c) and 3 months after (b, d) treatment showing increased sclerosis within the iliac bones (arrows, c, d) with a progressing hepatic metastasis (arrows, a, b). PSA rose to 1314 from 728 ng/mL indicating progressive disease
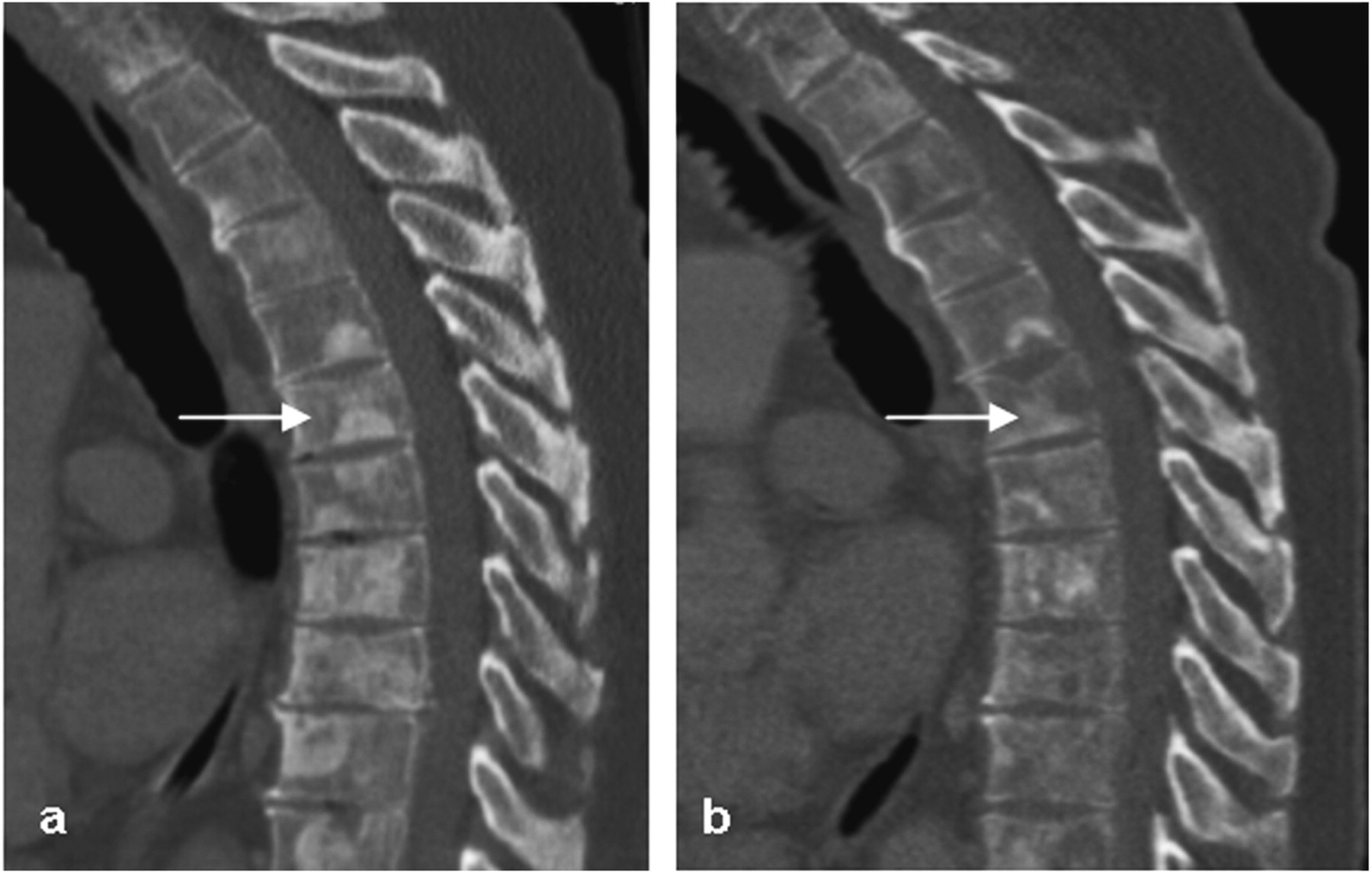
A 70-year-old man with CRPC and lytic progressive bone disease. Sagittal CT reconstructions through the dorsal spine before (a) and 3 months after (b) treatment showing fading of sclerosis within vertebral bodies despite treatment (arrows). PSA rose from 776 to 972 ng/mL
Seven out of eight patients with new bone sclerosis or sclerotic lesions increasing in density or size discordant to PSA/RECIST response showed a transient rise in ALP at one month (one patient's ALP fell by only one U/l). At 6 months the ALP of all patients in the flare group (n = 3) fell to below baseline. The remaining five patients who progressed at 6 months showed little further change or a continually rising ALP.
Discussion
This study demonstrated an 8% incidence of osteoblastic healing bone flare at 3-month post-treatment CT in patients with CRPC undergoing systemic treatment. Flare is well described on 99mTc-MDP bone scans and an incidence of 6% has been reported (7). It is also seen on 18FDG-PET (8). However, to the authors' knowledge the incidence of flare on CT has not previously been reported.
The flare response at 3 months on 99mTc-MDP bone scans and radiation dose considerations (3mSv) often limit its use to every 6 months in clinical trials. CT is therefore the first imaging assessment to be performed. The Prostate Cancer Clinical Trials Working Group (PCWG2) does not recommend follow-up 99mTc-MDP bone scintigraphy before 3 months of treatment unless clinically indicated and defining disease progression requires a confirmatory scan 6 or more weeks later (9). These recommendations are based on 99mTc-MDP bone scintigraphy flare response and our cases demonstrate that this phenomenon is also seen on CT.
In the current study, apparent progression of sclerotic metastases on CT discordant to a PSA/RECIST response was common at 3 months post-treatment (20.5%) and could not be used to discriminate progression from flare response. Most commonly these patients met progression criteria (PSA/RECIST) at the next assessment. However, just over one-third of this discordant group continued to show measurable signs of PSA/RECIST response or stable disease which highlights the necessity of follow-up in this group to avoid an incorrect diagnosis of progression. It should be noted that CT detected subjective fading and a reduction in HU of some lesions at 3 months in the patients who were clearly progressing by PSA/RECIST criteria. This critically important feature is an important indicator of early disease progression. Appearances on both CT and 99mTc-MDP bone scintigraphy can be misleading at 3 months, but post-treatment CT at 3 months offers additional information in patients with prostate carcinoma who show an increase in the number/size/density of sclerotic bone metastases with apparent improvement in other clinical parameters. In this group the absence of fading bone lesions increases confidence in the diagnosis of flare response as fading of sclerotic bone metastases is a well-recognized sign of lytic progression (10).
A transient rise in ALP followed by a decline has been described in patients responding to treatment and this was also evident in the flare group in our study (11, 12). However at 3 months ALP also rose in the progressing patients.
The lack of a histological gold standard is a limitation of both this and many other studies of metatastatic bone disease. Our next best approach is to use PSA, RECIST assessments of soft tissue disease and follow-up as markers of overall disease activity. The incidence of flare may be underestimated in this study as some of the patients excluded from the flare category by showing signs of progression at follow-up may in fact have been responding to treatment at the 3-month time-point. Incidence of the flare response may also be dependent upon treatment type/efficacy as it has been reported to be associated with a favourable response to treatment (13).
This study highlights the difficulties in assessing metastatic bone disease in CRPC trials. Less than one-third of patients had bone as the only site of disease at baseline. We have confirmed that healing flare response is a phenomenon demonstrated by CT at 3 months but that there may be features on imaging alone that support a diagnosis of flare rather than osteoblastic progression. None of the patients with flare at 3 months had fading of a bone metastasis; conversely all patients who progressed at 3 months had at least one lesion that faded in addition to lesions that increased in density.
In conclusion, flare response of metastatic bone occurs with an incidence of 8% at 3-month post-treatment CT in patients with prostate cancer undergoing systemic treatment. In patients with falling PSA and stable/responding soft tissue disease at 3 months, an increase in bone sclerosis in the absence of fading bone metastases can be interpreted as flare and is likely to represent a response.
Footnotes
ACKNOWLEDGEMENTS
We acknowledge the support received for the CRUK and EPSRC Cancer Imaging Centre in association with the MRC and department of Health (England) grant C1060/A10334 and also NHS funding to the NIHR Biomedical Research Centre.