
Abstract
Background
Hypertrophic cardiomyopathy (HCM) is reported to show patchy midwall myocardial hyperenhancement on delayed-enhancement magnetic resonance imaging (DE-MRI). The intramural distribution of myocardial hyperenhancement and its correlation with clinical symptoms, ventricular arrhythmias, and cardiac function have not been described forsymptomatic apical HCM.
Purpose
To evaluate the features and significance of myocardial hyperenhancement on DE-MRI insymptomatic apical HCM.
Material and Methods
Thirteen patients with symptomatic apical HCM and their 65 apical segments were investigated. Myocardial hyperenhancement and regional and global functional parameters were determined with MRI. We investigated the intramural distribution and frequencies of this myocardial hyperenhancement and compared them with the patients' clinical symptoms, the presence of ventricular arrhythmias, and cine MRI.
Results
Eight (61.5%) patients with symptomatic apical HCM displayed apical myocardial hyperenhancement, and 22 (33.8%) of the 65 apical segments examined showed myocardial hyperenhancement. Of the myocardial hyperenhancement observed, 81.8% showed a subendocardial pattern.The hyperenhanced apical myocardium had a lower percentage of systolic myocardial thickening, and was associated with serious symptoms (e.g. syncope) and ventricular arrhythmias.
Conclusion
Patients with symptomatic apical HCMshowed myocardial hyperenhancement involving the subendocardial layer, which might be related to regional systolic dysfunction, serious clinical symptoms, and ventricular arrhythmias.
Keywords
Apical hypertrophic cardiomyopathy (HCM) was first described as a unique phenotype of HCM with localized myocardial hypertrophy of the left ventricular (LV) apex and a ‘spade-like’ configuration of the LV cavity (1). This entity is a common type of HCM in Japan, accounting for about 15% of all HCM, whereas it is less common in the US where it accounts for 3% of HCM (2). Apical HCM is characterized by giant negative T-waves on ECG and a better prognosis than those for other types of HCM, such as asymmetrical septal hypertrophy (ASH) (1–5). However, one-third of patients with apical HCM present with a history of myocardial infarction, congestive heart failure, and ventricular arrhythmias (5).
The LV apex is often difficult to image by echocardiography because of its narrow view (6). Cardiac magnetic resonance imaging (MRI) is a valuable tool for the evaluation of regional and global LV function and the myocardial fibrosis associated with HCM (6–12). Delayed-enhancement MRI (DE-MRI) can detect the myocardial fibrosis associated with the regional and global deterioration of LV function, serious clinical symptoms such as syncope and cardiac arrest, and ventricular arrhythmias (8–10, 12–14). Therefore, DE-MRI can predict the clinical outcome of HCM (7, 9, 12, 13). However, the intramural distribution of myocardial hyperenhancement in apical HCM has not been described in detail, whereas patchy mid-wall myocardial hyperenhancement has been reported in ASH (8–10, 15). A previous study has denied a relationship between apical myocardial hyperenhancement and ventricular arrhythmias in apical HCM, but the study did not analyze the patients' clinical symptoms in detail (15). Therefore, the aim of this study was to investigate the imaging features and the significance of myocardial hyperenhancement in symptomatic apical HCM, by assessing the intramural distribution and frequency of myocardial hyperenhancement and by comparing them with the patients' clinical symptoms, the presence of ventricular arrhythmias, and cine MRI data.
Material and Methods
Study population
Cardiac MRI was performed in 113 consecutive patients with symptomatic HCM between January 2001 and April 2010. Of these patients, 14 patients (12.3%) had apical HCM, but one patient was excluded from further analysis because no informed consent for the use of gadolinium was given. Therefore, the final population consisted of 13 patients with symptomatic apical HCM (seven men and six women, mean age 66.4 years, age range 60–75 years). Their clinical symptoms that preceded the MRI studies were shortness of breath during daily exercises (n = 5), chest pain (n = 4), syncope (n = 2), pre-syncope (n = 1), and cardiac arrest (n = 1). Three patients had family histories of HCM. Four patients showed ventricular tachycardia on ambulatory ECG and one showed ventricular fibrillation on resting ECG. In all 13 patients, cine MRI at end-diastole showed a maximum apical myocardial thickness of >15 mm, a ratio of the maximal apical wall thickness to the basal anterior wall thickness of >1.3, and a spade-like configuration of the LV cavity (Fig. 1a) (3, 6, 15, 16). Patients with an LV apical aneurysm or a history of coronary artery diseases were not included in this study. The imaging studies were approved by our IRB, and informed consent was given by all the patients.

A 60-year-old woman with symptomatic apical hypertrophic cardiomyopathy. (a) Cine MRI shows typical spade-like configuration. The maximum apical wall thickness is 24.2 mm. (b) Delayed-enhancement MRI shows subendocardial myocardial hyperenhancement at the inferior wall (arrow). This patient has no ventricular arrhythmias
Imaging procedure
Cardiac MRI examinations were performed using a 3.0T unit (n = 7) or a 1.5 T unit (n = 6) (Philips Medical Systems, Best, The Netherlands). Breath-hold two-dimensional (2D) cine steady-state free precession (SSFP) imaging was performed on the short axis, and in two-, three- and four-chamber view planes. A breath-hold 2D DE-MRI was also performed on the short axis and two-chamber view planes 10 min after a slow injection of 0.15 mmol/kg gadolinium (gadodiamide or gadoteridol). The imaging parameters of the cine SSFP MRI and DE-MRI are shown in Table 1. The inversion time nullifying the normal myocardium was determined in each patient based on Look-Locker T1-weighted scout MRI.
Cardiac MRI parameters
Sensitivity encoding with a reduction factor of 1.3–2.0 was employed in the y-direction for both imaging sequences
Cine = cine steady-state free precession MRI with 20 cardiac phases, DE = delayed-enhancement inversion-recovery T1-weighted gradient-echo MRI
Image analysis
The LV myocardium was divided into 17 segments according to the AHA statement (17). A total of 221 LV myocardial segments including 65 apical segments were investigated in the 13 patients with symptomatic apical HCM on DE-MRI. The regional wall thickness and the percentage of systolic thickening of 52 apical segments were evaluated by short-axis cine MRI and DE-MRI. The segment 17 (i.e. the apical tip segment) was excluded from this analysis, because its wall thickness could not be estimated by the short-axis cine images. Myocardial hyperenhancement was defined as the myocardium with signal intensity 2SD greater than the remote normal myocardial signal (8).
Evaluation of myocardial hyperenhancement on DE-MRI
The myocardial segment numbers showing myocardial hyperenhancement (i.e. segment numbers 13–17) were noted. The patterns of apical myocardial hyperenhancement were classified as subendocardial myocardial hyperenhancement with transmurality of ≤50%, subendocardial myocardial hyperenhancement with transmurality of >50%, and patchy mid-wall hyperenhancement (7, 9, 10, 12, 18).
Relationships between regional function and DE-MRI
The apical wall thickness at end-diastole and the percentage of systolic wall thickening were estimated in segments 13–16 by short-axis cine MRI. We assessed the differences in these regional parameters between the hyperenhanced and normal myocardium in the apical segments. The differences between the normal myocardium, the hyperenhanced myocardium with transmurality of ≤50% or a patchy mid-wall pattern, and the hyperenhanced myocardium with transmurality of >50% were also assessed.
Relationship between ventricular arrhythmias and DE-MRI
The differences in the numbers of hyperenhanced myocardial segments and the percentage of hyperenhanced myocardial mass (i.e. the apical myocardial mass showing hyperenhancement/the myocardial mass of the apex) were statistically assessed between those patients with and without ventricular arrhythmias.
Correlation between global LV function and DE-MRI
The LV ejection fraction and the LV myocardial mass were estimated using cine MRI. The correlation between the total numbers of LV segments showing myocardial hyperenhancement and the LV ejection fraction or LV myocardial mass was assessed statistically.
Statistical methods
An unpaired t test, Mann-Whitney test, or Welch's t test was used to evaluate the differences in the quantitative data between two groups. The differences between the three groups in apical wall thickness at end-diastole and the percentage of systolic wall thickening were assessed using a factorial analysis of variance (ANOVA), followed by Holm's post hoc test. The correlation between the total numbers of LV segments showing hyperenhancement and the LV ejection fraction or myocardial mass was assessed with Spearman's correlation analysis. For all statistical analyses, a P value of less than 0.05 was defined as statistically significant, and the r value was noted when the correlation was significant.
Results
Evaluation of myocardial hyperenhancement on DE-MRI
Eight (61.5%) of the 13 patients with symptomatic apical HCM had apical myocardial hyperenhancement, and 22 (33.8%) of the 65 apical segments examined showed myocardial hyperenhancement (Figs. 1b and 2). Myocardial hyperenhancement was observed in six mid-ventricular segments, four of which were continuous with hyperenhanced apical segments. No basal myocardial segments showed hyperenhancement (Fig. 2). The anterior and inferior apical segments frequently showed myocardial hyperenhancement (Table 2). Of the 22 hyperenhanced apical segments, 18 (81.8%) showed a subendocardial pattern of myocardial hyperenhancement (Table 3).
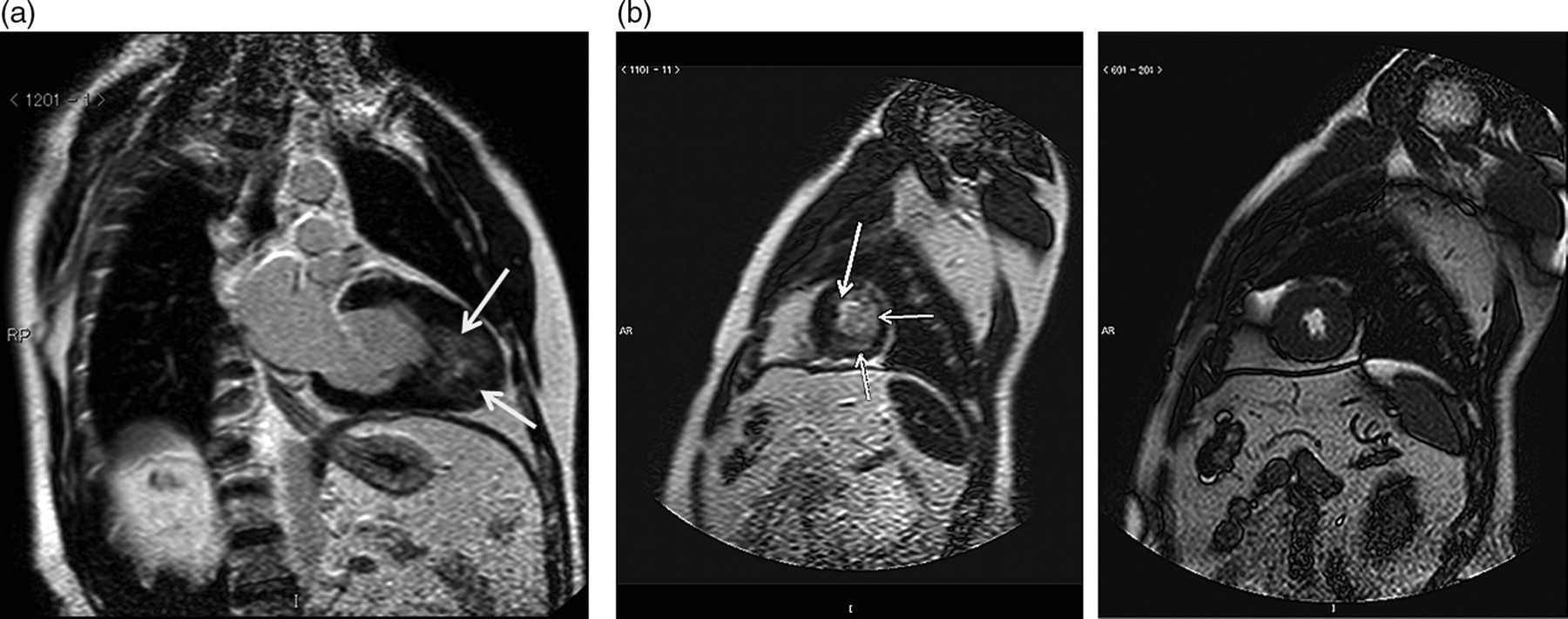
A 63-year-old man with apical hypertrophic cardiomyopathy showing syncope resulting from ventricular tachycardia. (a and b) Delayed-enhancement MRI shows wider hyperenhancement of the apical myocardium (arrow). (a) No myocardial hyperenhancement is seen in basal or midventricular myocardium. (b) Delayed-enhancement (left) and cine MRI (right) of the left ventricular apex are shown. The myocardial hyperenhancement shows a subendocardidal pattern (arrow). The percentage of systolic thickening is reduced at the apical anterior (2.8%) and lateral walls (1.9%). This patient underwent an ICD implantation
Apical segments with myocardial hyperenhancement detected by delayed-enhancement MRI in symptomatic apical hypertrophic cardiomyopathy
The numbers of patient with symptomatic apical hypertrophic cardiomyopathy were 13. The 60% of myocardial hyperenhancement was located in the anterior (no. 13 on AHA classification) and inferior apical segments (no. 15)
Patterns of apical myocardial hyperenhancement in symptomatic apical hypertrophic cardiomyopathy
The 65 apical myocardial segments in 13 patients with symptomatic apical hypertrophic cardiomyopathy were investigated. The 22 segments (33.8%) had myocardial hyperenhancement, 18 of which (81.8%) showed subendocardial patterns
Relationships between regional function and myocardial hyperenhancement on DE-MRI (Table 4)
There was no significant difference in the regional wall thickness of the normal and hyperenhanced myocardial segments. The percentage of systolic thickening in the apical myocardium was significantly lower in the hyperenhanced apical segments than in the normal apical segments on DE-MRI (P < 0.01). There were also significant differences in the percentage of systolic thickening between the normal myocardium, the hyperenhanced myocardium with transmurality of ≤50% or a patchy mid-wall pattern, and the hyperenhanced myocardium with transmurality of >50% (P < 0.05 on ANOVA). The post hoc test showed that the percentage of systolic thickening was significantly lower in the normal myocardium than in the hyperenhanced myocardium with transmurality of ≤50% or a patchy mid-wall pattern (P < 0.05) and in the hyperenhanced myocardium with transmurality of >50% (P < 0.01).
Comparison between regional cardiac function on cine MRI and apical myocardial hyperenhancement in symptomatic apical hypertrophic cardiomyopathy
The 52 apical myocardial segments were evaluated with short-axis cine and delayed-enhancement MRI in 13 patients with symptomatic apical hypertrophic cardiomyopathy
*The apical segments with myocardial hyperenhancement showed significantly lower percentage of systolic wall thickening than those without hyperenhancement (P < 0.01)
†In addition, the percentage of systolic thickening was significantly lower in the normal myocardium than in the hyperenhanced myocardium with transmurality of ≤50% or a patchy mid-wall pattern (P < 0.05) and in the hyperenhanced myocardium with transmurality of >50% (P < 0.01)
Relationship between ventricular arrhythmias and the extent of apical myocardial hyperenhancement on DE-MRI
Five patients presented with ventricular tachycardia or fibrillation. Their clinical symptoms were syncope (n = 2), pre-syncope (n = 1), cardiac arrest (n = 1), and shortness of breath (n = 1), and three of them had a family history of HCM. These patients displayed three (n = 2) or four (n = 3) apical segments with myocardial hyperenhancement (Fig. 2), whereas the eight patients without arrhythmias had 0 (n = 5), one (n = 2), and two (n = 1) hyperenhanced apical segments (Figs. 1b and 3). The percentage of hyperenhanced myocardial mass was significantly greater in the patients with ventricular arrhythmias (6.35 +/– 3.19%, median 7.20%, range 1.1–10.8%) than those without arrhythmias (0.45 +/– 0.75%, median 0.00%, range 0–2.1%). Therefore, the patients with ventricular arrhythmias had greater numbers of hyperenhanced myocardial segments (P < 0.01) and larger percentages of hyperenhanced myocardial mass (P < 0.05) in the LV apex.
Correlation between global LV function and myocardial hyperenhancement on DE-MRI
There was no significant correlation between the total numbers of LV myocardial segments with hyperenhancement and the LV ejection fraction or the myocardial mass in patients with symptomatic apical HCM.
Discussion
This present study demonstrated that eight (61.5%) of 13 patients with symptomatic apical HCM had 22 hyperenhanced apical segments on DE-MRI, in which the percentage of systolic thickening was significantly reduced. This study also showed that 18 (81.8%) of the 22 hyperenhanced apical segments had a subendocardial pattern of myocardial hyperenhancement. The patients with ventricular arrhythmias had more widely distributed myocardial hyperenhancement in the LV apex.
Distribution and frequency of hyperenhanced myocardial segments on DE-MRI
Most apical myocardial hyperenhancement (60%) was localized in the anterior and inferior segments, which is consistent with a previous report (15). Notably, more than 80% of the hyperenhanced apical segments showed a subendocardial pattern, which differs from the patchy mid-wall pattern seen in ASH (7, 8, 10). This subendocardial pattern in apical HCM might be attributable to its vulnerability to chronic ischemia because its blood supply derives from the peripheral coronary arteries and the cavity pressure in the LV apex is increased (11, 19, 20), whereas the patchy mid-wall hyperenhancement in ASH may be induced by intramural coronary artery stenosis and dysfunction or a high-pressure gradient at the LV outflow tract (11, 12, 21, 22).
One previous report described no myocardial hyperenhancement at the basal and midventricular levels (15), whereas another described a wide extent of myocardial hyperenhancement in apical HCM (8). Our results seem to lie between these two studies: no basal segments and six of the 78 mid-ventricular segments showed myocardial hyperenhancement. This might be explained by the fact that our study population was symptomatic, but did not include patients with apical aneurysms with extensive myocardial fibrosis or a thinned apical myocardium, and that the myocardium that is continuous with the apical myocardial fibrosis might suffer from ischemia (8, 22, 23).
Relationships between regional or global wall functions and the presence or transmurality of apical myocardial hyperenhancement on DE-MRI
This study indicated that as apical myocardial hyperenhancement progresses, it may be associated with regional systolic dysfunction in symptomatic apical HCM. However, no significant correlation was found between the total numbers of LV myocardial segments with hyperenhancement and the LV ejection fraction or myocardial mass in symptomatic apical HCM, probably because only a few mid-ventricular and no basal segments showed myocardial hyperenhancement. Therefore, the presence of myocardial hyperenhancement may not be related to heart failure or myocardial stiffness in the whole LV in symptomatic apical HCM.
Relationship between ventricular arrhythmias and the extent of apical myocardial hyperenhancement on DE-MRI
The clinical symptoms of the patients with ventricular arrhythmias were serious and included syncope and cardiac arrest. This study has shown that patients presenting with ventricular arrhythmias had more than two hyperenhanced apical segments. The percentage of hyperenhanced myocardial mass was also larger in these patients. The results of this investigation indicate a close relationship between the extent of myocardial hyperenhancement and ventricular arrhythmias in HCM (9, 12–14, 24). Although the relationship between myocardial hyperenhancement and ventricular arrhythmias or clinical symptoms may be complex, patients with symptomatic apical HCM and widely distributed hyperenhanced myocardium should be followed up rigorously to avoid missing an opportunity for preventive ICD implantation.
The present study had some limitations. First, the study population was relatively small. We also only enrolled patients with symptomatic apical HCM, and our findings cannot necessarily be extrapolated to apical HCM without apparent clinical symptoms. However, cardiac MRI may be used for the diagnosis and assessment of disease severity in apical HCM in the current clinical situation, rather than HCM family screening. Next, no apical myocardial biopsy was performed to confirm the subendocardial fibrosis in patients with symptomatic apical HCM. Previous histological studies have shown subendocardial myocardial fibrosis in apical HCM (3, 25). Lastly, we used 1.5T and 3.0T MRI, and the image quality of DE-MRI may be better with 3.0T MRI (26). However, in this study, we did not find that DE-MRI at 3.0T visualized more myocardial hyperenhancement.
In conclusion, DE-MRI showed a subendocardial hyperenhancement pattern of the apical myocardium in patients with symptomatic apical HCM. Apical myocardial hyperenhancement was associated with regional systolic dysfunction and significant ventricular arrhythmias in patients with symptomatic apical HCM.