
Abstract
Background
Ductal carcinoma in situ of the breast (DCIS) represents a challenge in mammographic screening due to its unknown progression into invasive cancer. The majority of the DCIS is detected due to signs of calcifications on the mammograms.
Purpose
To analyze the combinations of mammographic morphology and distribution of calcifications by Van Nuys nuclear grade (grade).
Material and Methods
A total of 217 DCIS diagnosed in women aged 50–69 years old who participated in the Norwegian Breast Cancer Screening Program in the period November 1995 to December 2007 were reviewed by four breast imaging specialists. The mammograms were classified according to the morphology and distribution of the calcifications, using BI-RADS nomenclature. Chi square test was used to compare the groups of morphology and distribution by grade.
Results
Calcifications were identified in 93% (202/217) of the cases, 15% (30/202) as grade 1 and 74% (149/202) as grade 3. Fine pleomorphic calcifications were seen in 38% (77/202) of the lesions and fine linear and fine linear branching in 31% (62/202). Sixty-nine percent (53/77) of the fine pleomorphic and 84% (52/62) of the fine linear and fine linear branching calcifications were high grade lesions. Grouped distribution was seen in about half of all the cases (104/202). Among the high grade lesions with fine pleomorphic or fine linear and fine linear branching calcifications, 75% (40/53) and 69% (36/52), respectively, had grouped or segmental distribution.
Conclusion
DCIS presented overlapping groups of morphology and distribution of calcification by grade, but fine pleomorphic and fine linear and fine linear branching calcifications with grouped and segmental distributions were associated with high grade DCIS. Seeking for further knowledge that allows separation of non-high grade from high grade DCIS has to continue to improve the quality of mammographic screening.
The incidence rate of ductal carcinoma in situ of the breast (DCIS) has increased in Norway, from 4 to 11 per 100,000 women years in the period 1993 to 2007 (1). Today DCIS represents 10–30% of all breast cancers diagnosed in civilized countries, with the highest percentage found in screen-detected cancers (1–4).
DCIS presents a spectrum of diseases with biological heterogeneity, and the natural history of the disease is poorly understood as it cannot be observed directly. However, there is a general consensus that in the vast majority of the cases, DCIS represents an intermediate step between normal breast tissue and invasive cancer (5–8). The lack of knowledge has led to uncertainty and discussions about the efficacy of detecting DCIS, particularly in screening (9, 10). The controversies have further led to concern about the treatment of the disease, which is claimed to be extensive because of the uncertain progression (11).
The Van Nuys prognostic index is developed to aid the complex treatment selection process for DCIS (12). The index combines tumor size, margin width, nuclear grade, and the presence or absence of comedonecrosis. Van Nuys prognostic classification combines high nuclear grade and comedo-type necrosis to predict clinical recurrence and is usually referred to as grade (hereafter referred as grade). Grade 1 is non-high-grade DCIS without comedo-type necrosis, grade 2 is non-high-grade with comedo-type necrosis, and grade 3 represents high-grade DCIS with or without comedo-type necrosis (12). Distinguishing non-high grade DCIS from high grade is thus important because of the likelihood of developing into invasive cancer.
The majority of the DCIS lesions are diagnosed as calcifications at mammographic screening (13–18). Calcifications are considered easy to perceive, but challenging to interpret and differentiate into benign and malignant. Different classifications groups indicating the probability of malignancy have thus been suggested (19–21). The Breast Imaging-Reporting and Data System (BI-RADS®) nomenclature includes amorphous and coarse heterogenic calcifications in the group of intermediate concern, while fine pleomorphic and fine linear and fine linear branching calcifications are comprised in the group with higher probability of malignancy (21). Bilateral, large, smooth, and dense calcifications scattered over a large area are usually considered benign, while clustered or linear are considered suspect for malignancy.
To increase the radiologic sensitivity of detecting high grade DCIS lesions, we retrospectively reviewed all screening mammograms showing pure DCIS and classified the mammographic morphology and distribution of calcifications according to BI-RADS® nomenclature. The study was aimed at identify combinations of morphology and distribution of the calcifications by grade.
Material and Methods
This study included pure DCIS only; DCIS with microinfiltration was excluded. The diagnosis was based on histological specimens. The study was approved by the Norwegian Social Science Data Services.
Study population
A total of 269 DCIS were diagnosed in Rogaland County, among women aged 50–69 years during the study period November 1995 to December 2007. Among those, 248 cases were diagnosed as a part of the Norwegian Breast Cancer Screening Program (22, 23). These cases were object for a retrospective review according to histologic morphology and grade. The histopathologic review resulted in an invasive or benign diagnosis in 26 cases, of which 222 cases were available for the radiological review. Mammograms were not available for five of these cases whereas 217 cases were left for a retrospective radiologic review. The review identified calcifications in 202 mammograms, which were the basis for the analyses. The 202 cases represented women with a mean age of 58.3 years (median 57.8 years, range 49.3–71.2).
Pathological review
The breast pathologist knew that all cases had a diagnosis of DCIS before reviewing the cases, but did not know the grading. If the reviewer did not agree with the previous statement of DCIS morphology, an arbitration of two or three experienced pathologists was reached. The review resulted in upward revision into invasive breast cancer in nine cases (3.6%) and downward revision into atypical ductal hyperplasia or intraductal hyperplasia in 17 cases (6.9%).
Radiological review
Four breast radiologists reviewed the mammograms; three had read screening mammograms since the start-up of the screening program in the county (1995). The fourth radiologist had six years' experience with mammography including five years of experience in daily work with the BI-RADS® nomenclature. The radiological review was divided into two parts; independent individual, and consensus. All four radiologists did both the individual review and took part in the consensus. The radiologists were aware of the presence of a pure DCIS, but blinded to side, site, size, clinical findings, and further histologic information. The screen film mammograms (n = 197) were analyzed using a light box (Rotolux/Planilux 400; Siemens, Erlangen Germany), while a dedicated work station (Advanced Workstation 4.4; GE Healthcare, London, U K) was used for the full-field digital mammograms (n = 20).
The BI-RADS® classifies calcifications into typically benign (skin, vascular, coarse, large rod like, round, lucent center, eggshell or rim, milk or calcium, suture, dystrophic, and punctated calcifications), of intermediate concern (amorphous or indistinct, or coarse heterogeneous), and with a higher probability of malignancy (fine pleomorphic or fine linear and fine linear branching calcifications) (21). This study classified mammographic features in following morphology, which is a modification of the BI-RADS:
Punctated – round or oval calcifications, <0.5 mm, with well-defined margins; Amorphous – usually rounding or ‘flaking’ shaped calcifications, sufficiently small or hazy in appearance of which a specific morphologic classification cannot be determined; Coarse heterogeneous – irregular, conspicuous calcifications generally >0.5 mm, tending to coalesce but not of a size of irregular dystrophic calcifications; Fine pleomorphic – usually more conspicuous than the amorphous forms of calcifications. Neither typically benign nor typically malignant irregular calcifications with varying sizes and shapes. Usually <0.5 mm in diameter; Fine linear and fine linear branching – thin, irregular linear calcifications, discontinuous and <0.5 mm in width. Grouped or clustered – at least five calcifications occupying a small volume (<1 cc) of tissue; Segmental – calcifications depositing in a duct and its branches, raising the possibility of multifocal breast cancer in a lobe or segment of the breast; Regional – calcifications scattered in a large volume (>2 cc) of breast tissue not necessarily conforming to a duct distribution that are likely benign, but are not everywhere in the breast, and do not fit the other more suspicious categories; Linear – calcifications arrayed in a line that may have branch points; Diffuse or scattered – calcifications distributed randomly throughout the breast.
The distribution of the calcifications was used as a modifier of the basic morphologic description and the arrangement was classified as following (21):
Statistical analysis
The study material is presented as number and percentages by grade, age at diagnosis (Table 1), and time (Fig. 1). Van Nuys nucleus grade 1 and 2 are referred to as non-high grade and grade 3 as high grade. All analyses are based on the outcome of the radiologic consensus review. Morphology and distribution of calcifications are given by non-high and high grade DCIS lesions. Chi-square test is used for tests of statistical significance between groups. A P value equal to or less than 0.05 is considered statistically significant. All tests are two-sided. Kappa values of the four readers' agreement are calculated for all six combinations of readers (KDK:LE; KDK:BFI; KDK:BMS; LE:BFI; LE:BMS; BFI:BMS) and for each of the readers versus consensus. Kappa value <0.20 is considered poor, 0.21–0.40 is fair, 0.41–0.60 is moderate, 0.61–0.80 is good and kappa value >0.81 is very good observer agreement (24). The analyses were conducted using SPSS (SPSS, version 17.0.1 for Windows, SPSS Inc, Chicago, IL, USA).
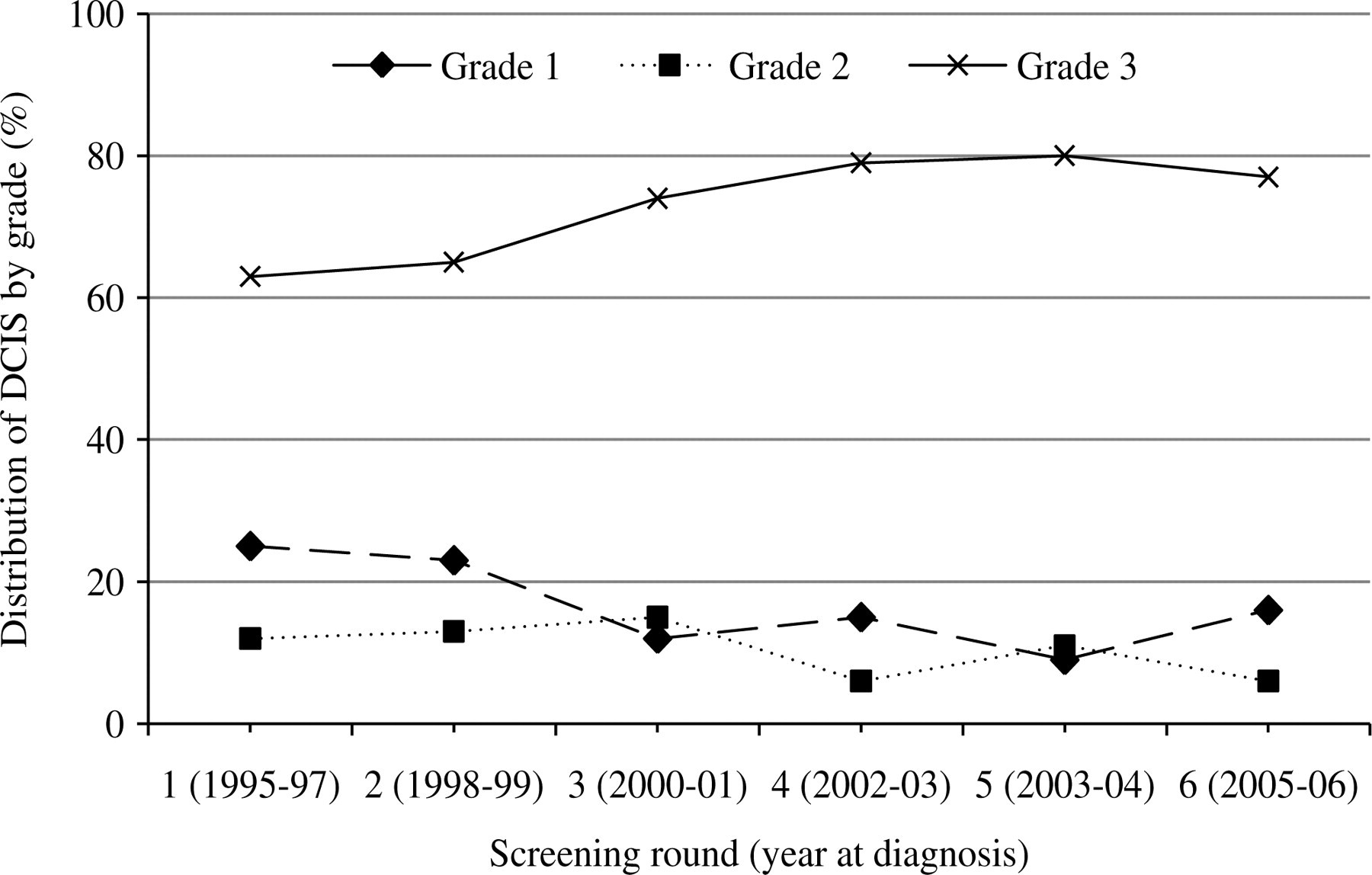
Ductal carcinoma in situ by grade and screening round in 217 women diagnosed in Rogaland County, as a part of the Norwegian Breast Cancer Screening Program, 1995–2007
Van Neuys nuclear grade distribution of ductal carcinoma in situ diagnosed in Rogaland County, as a part of the Norwegian Breast Cancer Screening Program, 1995–2007
*Chi square test for trend
Results
Among all DCIS diagnosed in the study period, 17% (37/217) were grade 1, 11% (23/217) grade 2, and 72% (157/217) grade 3 (Table 1). Grade distribution was not influenced by age at diagnosis (Chi square = 0.134). Grade distribution varied by time after start-up of screening (Fig. 1), but the differences did not reach statistical significantly differences (P = 0.348 for grade 1 and P = 0.381 for grade 3). The distribution of grade in analogue versus digital mammography were 16% (31/197) versus 30% (6/20) for grade 1, 12% (23/197) versus 0% for grade 2 and 73% (143/197) versus 70% (14/20) for grade 3. None of the differences reached statistical significant level. Among the 202 DCIS showing calcifications on the mammograms, 15% (30/202) were grade 1, 11% (23/202) grade 2, and 74% (149/202) grade 3.
Morphology
For non-high grade and high grade lesions combined, fine pleomorphic was the most frequent morphology of the calcifications (38%, 77/202) (Table 2). Fine linear and fine linear branching was found in 31% (62/202) and amorphous in 27% (55/202) of the cases. The fine pleomorphic contributed with 45% (24/53) of the non-high grade and 36% (53/149) of the high grade lesions (P = 0.278). Fine linear and fine linear branching was presented in 19% (10/53) of the non-high grade and 35% (52/149, P = 0.045) of the high grade lesions, while amorphous contributed with 32% (17/53) of the non-high grade and 26% (38/149, P = 0.457) of the high grade lesions.
Mammographic morphology of calcifications by grade in 202 screening mammograms* showing ductal carcinoma in situ
*Screening mammograms in women aged 50–69 years who participated in a population-based screening program
† P value (Chi-square test) between non-high (Van Nuys nuclear grade 1 and 2) and high grade (Van Nuys nuclear grade 3) lesions
Distribution
Grouped distribution was present in 51% (104/202) of all the cases; segmental in 22% (44/202) and regional in 19% (38/202) (Table 3). Grouped distribution contributed to 53% (28/53) of the non-high grade and 51% (76/149) of the high grade lesions, segmental 21% (11/53) and 22% (33/149), regional 23% (12/53) and 17% (26/149), and linear in 3% (1/53) and 9% (14/149), in non-high and high grade lesions, respectively. None of the differences reached statistically significant level.
Distribution of calcifications by grade in 202 screening mammograms* showing ductal carcinoma in situ
*Screening mammograms in women aged 50–69 years who participated in a population-based screening program
† P value (Chi-square test) between non-high (Van Nuys nuclear grade 1 and 2) and high grade lesions (Van Nuys nuclear grade 3)
Morphology and distribution
The distribution of correlating morphology and distribution as a percentage of non-high (n = 53) and high grade lesions (n = 149) did not differ statistically significant for any of the combinations (Table 4). High grade lesions with fine pleomorphic morphology was identified in combination with grouped or segmental distribution in 75% (40/53) of the cases, while 70% (36/52) of the high grade fine linear and fine linear branching calcifications had that distribution. Fine linear and fine linear branching morphology with segmental distribution was shown in 14% (20/149) of the high grade lesions while this combination was not identified in non-high grade lesions. One single high grade case showed punctuated morphology with regional distribution.
The correlation between distribution and morphology of calcifications by grade in 202 mammograms showing ductal carcinoma in situ in a population based breast cancer screening program including women aged 50–69 years at diagnosis
*Non-high grade lesion (Van Nuys nuclear grade 1 and 2)
†High grade lesion (Van Nuys nuclear grade 3)
Inter-reader variability
Kappa for the individual versus consensus review of calcification morphology ranged from 0.58 to 0.68, while the values ranged from 0.39 to 0.51 between the five readers (not in table). Kappa for the individual versus consensus review of calcifications distribution ranged between 0.49 and 0.68 for individual versus consensus review and from 0.44 to 0.55 for the individual reviews. All kappa values had a P value <0.001.
Discussion
Seventy-two percent of the DCIS diagnosed in a mammographic screening program targeted at women aged 50–69 years represented high grade lesions. Calcifications were identified in 93% of the 217 lesions. Neither morphology, nor distribution of the calcifications differed statistically significantly by grade, except for fine linear and fine linear branching morphology that showed borderline higher percentage of high compared to non-high grade lesions. However, fine pleomorphic and fine linear and fine linear branching morphologies, in combination with grouped or segmental distribution confirmed their clinical implications by representing the majority of the high-grade lesions. The results underscore that determination of distinctive characteristics of calcifications in high versus non-high grade DCIS lesions is challenging.
Two mechanisms are described to initiate calcifications in the breast: secretion and necrosis (25, 26). In secretion, tumor cells but also benign cells can produce fluid which is excreted in the extra-cellular matrix, and calcification arises. This type of calcification is most common in benign and non-high grade lesions and in many DCIS cases there are ‘benign calcifications’ present that might originate from a period prior to the induction of the tumor. Calcifications in high grade DCIS are usually related to the necrotic debris. Necrosis refers to cells that are dying and the simultaneous attraction of other chemicals, whereas comedo necrosis is formed out of residuals, and leftover dead cells. Comedo necrosis often attracts calcium from the blood and the calcium deposits that are formed are visible on the mammograms. These two mechanisms, secretion and necrosis, sometimes co-exist in the same DCIS. Necrosis is obviously a part of the grading used in this study and the choice of presenting the lesions by Van Nuys non-high and high grade does not make us able to discriminate between the lesions with and without comedo-type necroses. This might be considered a limitation of the study, but is the recommended way of merging the groups (12).
The fact that three out of four DCIS presenting calcifications in this study were high grade indicates that most of the lesions had a high probability of progressing into invasive cancer if left untreated (5–8). The rate is somewhat higher than reported in other studies (2, 18, 20, 27). The subjective grading system causes inter-reader variability by the pathologists (28) and different grading systems might be of influence for the different rates (29). Improved skills and techniques, including access to digital mammography, computed aided detection, high frequency ultrasound, MRI, and 3D studies might also be of influence, and do not seem mutually exclusive.
Calcifications were visible in 93% of the mammograms holding DCIS in this study. Other studies have reported visible calcifications in 60–90% of the DCIS (13–18). Use of digital mammography with higher contrast resolution than analogue mammography has the potential of increasing detection of DCIS by making the mammographic features easier to perceive and interpret (30). An increased detection rate of DCIS in the last part of the study period, where digital systems were taken into use, supports this statement. However, the majority of the cases in this study were diagnosed on screen film mammograms. Careful attention to calcification in the interpretation of the screening mammograms might thus be the explanation for the high rate of calcifications in this study.
Our study did not reveal amorphous and coarse heterogeneous morphology as the major contributor of non-high grade lesions (intermediate concern), as expected according to BI-RADS. However, fine pleomorphic and fine linear and fine linear branching represented the majority of the high grade lesions (high probability of malignancy). Classifying mammograms by features is a challenging task, since the distinction between morphologies is not obvious. Some cases may also include several morphologies (15, 16). The results in our study differed somewhat from the results shown by Tabar in his study of 207 DCIS diagnosed in Dalarne, Sweden, in the period 1977–1994 (20); 38% in this study versus 52% in Tabar's study were classified as fine pleomorphic (crushed stones by Tabar), 31% versus 30% were classified as fine linear and fine linear branching (casting by Tabar), and 27% versus 18% as amorphous (powdery by Tabar). The different distributions could be due to the radiological skill, perception and interpretation. Another aspect is the possibility of including DCIS with invasive components in Tabar's study. Our study included only pure DCIS.
About eight in 10 fine linear and fine linear branching calcifications represented high grade lesions in this study. Fine linear and fine linear branching morphology are comparable to the casting classification in Tabar's notation, in which the cases are shown to have poor survival (20). This is further supported in studies showing associations between fine linear and fine linear branching calcifications, poorly differentiated cells and high grade DCIS (26, 27). Fine linear and linear branching calcifications are often small and challenging to catch in a screening setting (15, 21, 31). However, the high probability of malignancy might do the interpretation of such calcification less challenging as cases presenting fine pleomorphic, coarse heterogeneous or amorphous calcifications. Fine pleomorphic calcifications represented the most common morphology, both in non-high grade and high grade lesions. Fine pleomorphic morphology is described as irregular calcifications which are neither typically benign nor typically malignant, while coarse heterogeneous calcifications are usually larger (16, 21, 31). Our findings indicate that all the types of lesions mentioned in this subsection should be removed by excision.
Grouped distribution was most commonly present, both for non-high grade and for high grade. The high proportion of grouped distribution is logic when assuming screen detected cancers as small in size. Grouped or clustered distributions usually raise suspicions; although only about one-quarter prove to be the result of a malignant process (20). The distribution represents a small volume (<1 cc), including at least five calcifications (21). Segmental distribution contributed with 22% of the distributions and raises the possibility of extensive or multifocal breast cancer in a lobe or segment of the breast and should always be analyzed in detail to ensure its malignancy. Regional distribution covers a wide area (>2 cc), in which malignancy is less likely. Diffuse and scattered distributions are often bilateral and considered a benign sign. These distributions are usually observed in punctated and amorphous calcifications. This study included too few cases for comparing the different morphologies in cases with punctuated distribution of calcifications.
The mammograms were reviewed to identify combinations of morphology and distribution that classified the non-high grade versus the high grade lesions. The small number in each category hampered the possibility of the statistical significant results. However, more than half of the high-grade lesions were fine pleomorphic, and three-quarters of these lesions showed grouped or segmental distribution of the calcifications, which makes this combination clinically important. The combination of fine linear and fine linear branching with grouped or segmental distribution is also of clinical importance. These two morphologies are found to be derived from extensive necrosis and is usually associated with high grade DCIS (15, 16, 26, 31). One high grade lesion showed powdered calcifications with regional distribution. Neither powdered calcifications nor regional distribution are suspect for malignancy. This finding was thus somewhat surprising, but might be related to tumor size (26). As small clusters of punctate or granular calcifications may represent high grade DCIS, an aggressive clinical approach to such lesions is recommended since adequate treatment of high grade DCIS will prevent the occurrence of potentially life-threatening high grade invasive disease.
The pathological review represents a limitation in this study, since it ideally should have been performed in consensus. However, observer variability in nuclear grading is well known (28), and a consensus review would probably not been of substantial influence for the distribution of non-high versus high grade lesions. There are also several aspects of the radiologic review we would have liked to improve. Registration of more than one morphology would have made us able to investigate possible combinations and their correlation with distribution. Further is mammographic soft tissue abnormality shown to be related to calcifications in 20–25% of all DCIS (31), particularly for fine pleomorphic, coarse heterogeneous and amorphous calcifications. Including a variable describing the soft tissue related to the calcifications could thus have brought valuable knowledge to our study. We also consider tumor size and the number of calcification flakes as important to review in our next study (26).
The radiologist's limited experience in using BI-RADS® classification of mammographic features might be considered as a limitation. Only one radiologist had profound experience in using this classification in daily routine. However, the radiologists read the BI-RADS® Breast Imaging Atlas, studied literature and discussed clinical cases before study start, in order to get the essential knowledge.
In conclusion, interpretation of calcifications is a great challenge in mammographic screening since the correlation between morphology, distribution and grading is not clear and some overlap between the categories exist. Further studies including a larger number of cases, both benign lesions, DCIS and invasive breast cancer, correlations of mammographic features by histologic findings, biomarkers and survival deem necessary in the understanding the progression of the disease, of which optimal detection and treatment of the disease might be possible.