
Abstract
Background
Leptomeningeal high signal intensity (ivy sign) on fluid-attenuated inversion-recovery (FLAIR) MR imaging is one of the features of Moyamoya disease. However, the correlation between ivy sign and cerebral perfusion status has not been fully evaluated.
Purpose
To characterize ivy sign on FLAIR images in Moyamoya disease and compare this finding with hemodynamic alterations on perfusion single-photon emission CT (SPECT) obtained before and after bypass surgery.
Material and Methods
Sixteen patients with angiographically confirmed Moyamoya disease who underwent superficial temporal artery-middle cerebral artery (STA-MCA) anastomosis were included in the study. The presence of ivy sign on FLAIR images was classified as ‘negative’, ‘minimal’ and ‘positive’. We evaluated the relationship between ivy sign and findings of SPECT, including cerebral vascular reserve (CVR) before and after surgery.
Results
Minimal or positive ivy sign was seen in 13 (81%) of 16 patients, and 21 (66%) of 32 hemispheres. CVR in the areas with positive or minimal ivy sign was lower than that in the areas with negative ivy sign. After STA-MCA anastomosis, ivy sign disappeared or decreased in all 21 hemispheres demonstrating ivy sign. SPECT demonstrated apparent hemodynamic improvement in areas demonstrating disappearance or decrease of ivy sign.
Conclusion
Ivy sign on FLAIR image is seen in areas with decreased cerebral perfusion. The sign is useful for non-invasive assessment of cerebral hemodynamic status before and after surgery.
Moyamoya disease is a rare progressive cerebrovascular occlusive disease of the internal carotid arteries and their branches that causes compensatory development of a fine collateral vascular network at the base of the brain (moyamoya vessels) (1). The characteristic clinical symptoms include serious neurological deficits due to cerebral ischemia and/or brain hemorrhages. There are no effective medical therapies for Moyamoya disease, and therefore, surgical re-vascularization via superficial temporal artery–middle cerebral artery (STA–MCA) anastomosis with or without an indirect bypass is the standard surgical treatment for Moyamoya disease (2).
Cerebral angiography and MR imaging are indicated for the diagnosis and grading of Moyamoya disease. Perfusion single-photon emission computed tomography (SPECT) has also been used to evaluate cerebral blood-flow (CBF). SPECT after acetazolamide challenge allows the cerebral vascular reserve (CVR) to be measured during preoperative and postoperative assessments. A low CVR, which is a risk factor for ischemic stroke, can be used as one of the criteria for determining which side(s) of the brain requires bypass surgery (3, 4). CVR is also useful for predicting the efficacy of surgical re-vascularization and the clinical outcome after bypass surgery (5).
The classical MR imaging features of Moyamoya disease include new and/or old infarcts or hemorrhages, brain atrophy with ventricular dilatation, loss of flow voids in the supraclinoid internnal carotid arteries, and the appearance of numerous collateral vessels, which appear as small flow voids, at the base of the brain (moyamoya vessels) (6–8). In addition to these classical features, diffuse leptomeningeal enhancement on post-contrast MR images can be seen. Ohta et al. first reported this finding and called it the ‘ivy sign’ because the pattern of contrast enhancement resembled ivy creeping across stones (9). Although the mechanism of the ivy sign is unclear, it is speculated that the slow retrograde flow of engorged pial collateral arteries, the thickening of the leptomeninges due to congestion, and maximally dilated pial vessels are associated with its presence (10–12). This finding is not only useful as an indirect sign of Moyamoya disease, but also for the assessment of the postoperative outcome with regard to the cerebrovascular status, as it disappears or decreases after successful bypass surgery (9, 13). The ivy sign can also be demonstrated on fluid-attenuated inversion-recovery (FLAIR) images (10, 11, 14). However, to the best of our knowledge, little is known about whether the appearance of the ivy sign on FLAIR images accurately represents the hemodynamic status of the brain in Moyamoya disease.
The purpose of this study is to evaluate the clinical significance of the appearance of the ivy sign on FLAIR images in patients with Moyamoya disease by comparing its distribution with the hemodynamic findings of perfusion SPECT before and after bypass surgery.
Material and Methods
Patients
Between 2003 and 2008, 23 patients with idiopathic Moyamoya disease underwent STA-MCA anastomosis in our hospital. Among these patients, 16 patients who underwent MR imaging including FLAIR imaging before and after bypass surgery were enrolled in this study. Four of the 16 patients were male and 12 were female, and their ages ranged from 1 to 45 years (median 24 years). Seven patients underwent bilateral STA- MCA anastomosis, and the remaining nine patients underwent unilateral STA-MCA anastomosis. The diagnosis was established from clinical findings, MR imaging, and MR angiography, in addition to conventional angiography. The initial clinical symptoms were a transient ischemic attack in 13 patients, convulsions in two, and hemorrhaging in one (Table 1). Surgical indications were determined according to the treatment guidelines recommended by the research committee on Moyamoya disease of the Ministry of Health and Welfare, Japan; a bypass surgery is indicated when there are repeated clinical symptoms due to apparent cerebral ischemia as well as decreased regional cerebral bloodflow, vascular response, and perfusion reserve (15).
Clinical data of the 16 patients
TIA = transient ischemic attack, ASD = atrial septal defect, HT = hypertension, DM = diabetes mellitus
*Angiographic stages of Moyamoya disease described by Suzuki and Takaku (22)
Imaging protocols
MR imaging was performed using a 1.5 T scanner (Signa LX, and Signa HDx; GEHealthcare, Milwaukee, WI, USA). FLAIR images were obtained with the following parameters: TR: 8000 ms, TE: 105 ms, inversion time: 2000 ms, thickness: 6 mm, gap: 2 mm, matrix: 256 × 160, number of excitations: 2.0.
Brain perfusion SPECT imaging was performed using a triple-head gamma camera (PRISM 3000; Picker, Cleveland, OH, USA) equipped with a high resolution, fan-beam collimator. We performed the SPECT procedures according to the split-dose method protocol of Hashikawa et al. (16). The data acquisition protocol involved a 1208 rotation separated into 38 steps and an acquisition time of 30 s per step. All images were re-constructed by filtered back-projection using a ramp filter, and attenuation correction was applied using Chang's method. A 64×64 image matrix was used for the data acquisition and display. During the dynamic SPECT, which involved 24 frames (2 min 30 s per frame), 111 MBq 123I-IMP (Nihon Mediphysics, Tokyo, Japan) was intravenously injected at the start of imaging. Twenty mg/kg (more than 50 kg: 1 g, under 50 kg: 20 mg/BWkg) acetazolamide (Diamox; Sanwa Kagaku Kenkyusho Co, Nagoya, Japan) was then slowly intravenously injected over a 1-min period during the fourth frame (9 min after the initial 123I-IMP injection) in all patients over the age of 22 years. An additional 111 MBq 123I-IMP was injected during the 10th frame (25 min after the start of imaging). Continuous arterial sampling of the octanol fraction at a constant speed of 1 mL/min for 5 min was started at 30 s before the first frame, and it was stopped at 30 s after the second frame. CVR was calculated using the following formula:
(ACZ challenge SPECT count − resting SPECT count)/ resting SPECT count (%)
Perfusion SPECT images were obtained in 12 patients before and after bypass surgery. The CVR induced by acetazolamide challenge was measured in 10 patients: before and after surgery in eight patients, and before surgery alone in two patients. The two remaining patients (who were under the age of 22 years) did not undergo acetazolamide SPECT.
Image analysis
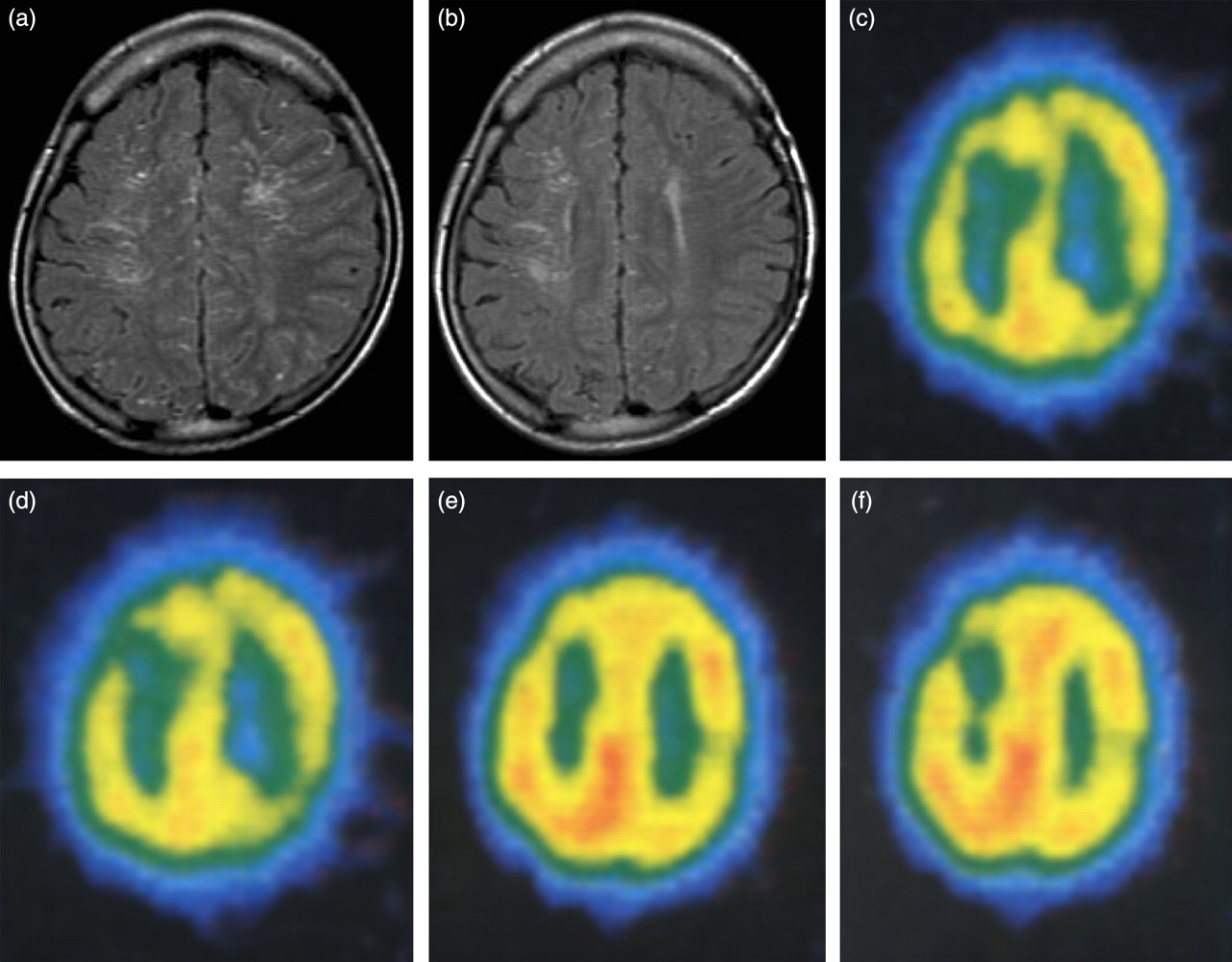
We analyzed the preoperative MR images at 1–270 days (median 14 days) before surgery and the postoperative MR images at 3–20 months (median 165 days) after surgery. The ivy sign was defined as continuous linear or punctate high signal intensity along the cortical sulci and subarachnoid space (9–11, 13, 14). The corticosubcortical region of each cerebral hemisphere was divided into the following four regions according to the method described in a previous report (17): the anterior cerebral artery (ACA) region, the anterior half of the MCA region (ant-MCA), the posterior half of the MCA region (post-MCA), and the posterior cerebral artery (PCA) region. The ant-MCA and post-MCA regions were separated by the central sulcus, with the temporal lobe belonging to the post-MCA (12). We also evaluated cerebellum and brainstem. Two neuroradiologists blinded to the clinical information reviewed the FLAIR images and rated the presence of the ivy sign as ‘negative’, ‘minimal’, or ‘positive’ in each region by consensus. Minimal ivy sign was defined as subtle and equivocal high signal intensity along the cortical sulci, whereas positive ivy sign was defined as obvious linear and punctate high signal intensity (11) (Figs. 1a and 2a)

A 43-year-old woman with Moyamoya disease. FLAIR images (a, b) before and (c,d) after right STA-MCA anastomosis. Preoperative FLAIR images showed positive ivy sign (arrows) in right ACA and posterior MCA regions, and showed minimal ivy sign (arrowhead) in anterior MCA and PCA regions. Postoperative FLAIR images obtained 5 months after re-vascularization surgery revealed disappeared ivy sign in the right hemisphere. The ivy signs in the left hemisphere were also decreased after bypass surgery (e, f). Preoperative SPECT showed a decreased CVR in both hemispheres (g, h). Postoperative SPECT after right STA-MCA anastomosis demonstrated hemodynamic improvement in the areas in which the ivy signs disappeared or decreased
A 9-year-old girl with Moyamoya disease. FLAIR images (a) before and (b) after left STA-MCA anastomosis. Preoperative FLAIR images showed positive ivy sign in bilateral hemispheres. The ivy signs in both hemispheres decreased after bypass surgery. Resting SPECT images (c, d) before and (e, f) after surgery. SPECT demonstrated hemodynamic improvement in both hemispheres
The improvement of blood flow after surgery was visually evaluated on perfusion SPECT in each region and was compared with the change in the appearance of the ivy sign on FLAIR.
Perfusion SPECT images performed at 3–9 months after the last re-vascularization surgery was analyzed because neovascularization is expected to peak several months after the operation (5). In addition, the correlation between CVR values and the presence of the ivy sign was examined in each region. Two patients suffered cortical infarctions, and the two regions containing the infarctions were excluded from the analysis.
Statistical analysis
The distribution of the ivy sign was compared between ACA, MCA, and PCA regions using the Mantel-extension test. We also examined the relationship between the appearance of the ivy sign and CVR findings on SPECT before and after surgery. For statistical analysis, the Kruskal-Wallis test combined with the post-hoc test and the Wilcoxon signed rank test were employed, and all analyses were performed using the GraphPad Prism version 5.0 software (GraphPad Software, San Diego, CA, USA), with p < 0.05 considered statistically significant.
Results
Preoperative evaluation
Before bypass surgery, FLAIR images revealed the presence of the ivy sign in 13 (81%) of 16 patients and 21 (66%) of 32 hemispheres. The ivy sign findings were positive or minimal in 14 ACA regions, 16 ant-MCA regions, 17 post-MCA regions, and nine PCA regions. The ivy sign was thus more prominent in the ACA and MCA regions than in the PCA region, but a comparison showed no significant statistical difference in its distribution between the four regions (p = 0.092) (Table 2). The ivy sign was not seen over the brainstem or cerebellum.
Presence and distribution of the ivy sign on FLAIR images in 32 hemispheres of 16 patients with Moyamoya disease. The numbers indicate the number of regions. One region in the left ACA and another region in the ant-MCA were excluded from the analysis because they contained cortical infarcts
Perfusion SPECT revealed focal or global decreases in CBF in all 24 hemispheres of the 12 patients. CVR was significantly decreased in the areas demonstrating positive or minimal ivy sign findings compared with the areas that were negative for the ivy sign (p < 0.05) (Fig. 3). Nine (47%) of 19 areas that demonstrated positive ivy sign findings exhibited negative CVR values, suggesting the occurrence of the steal phenomenon.
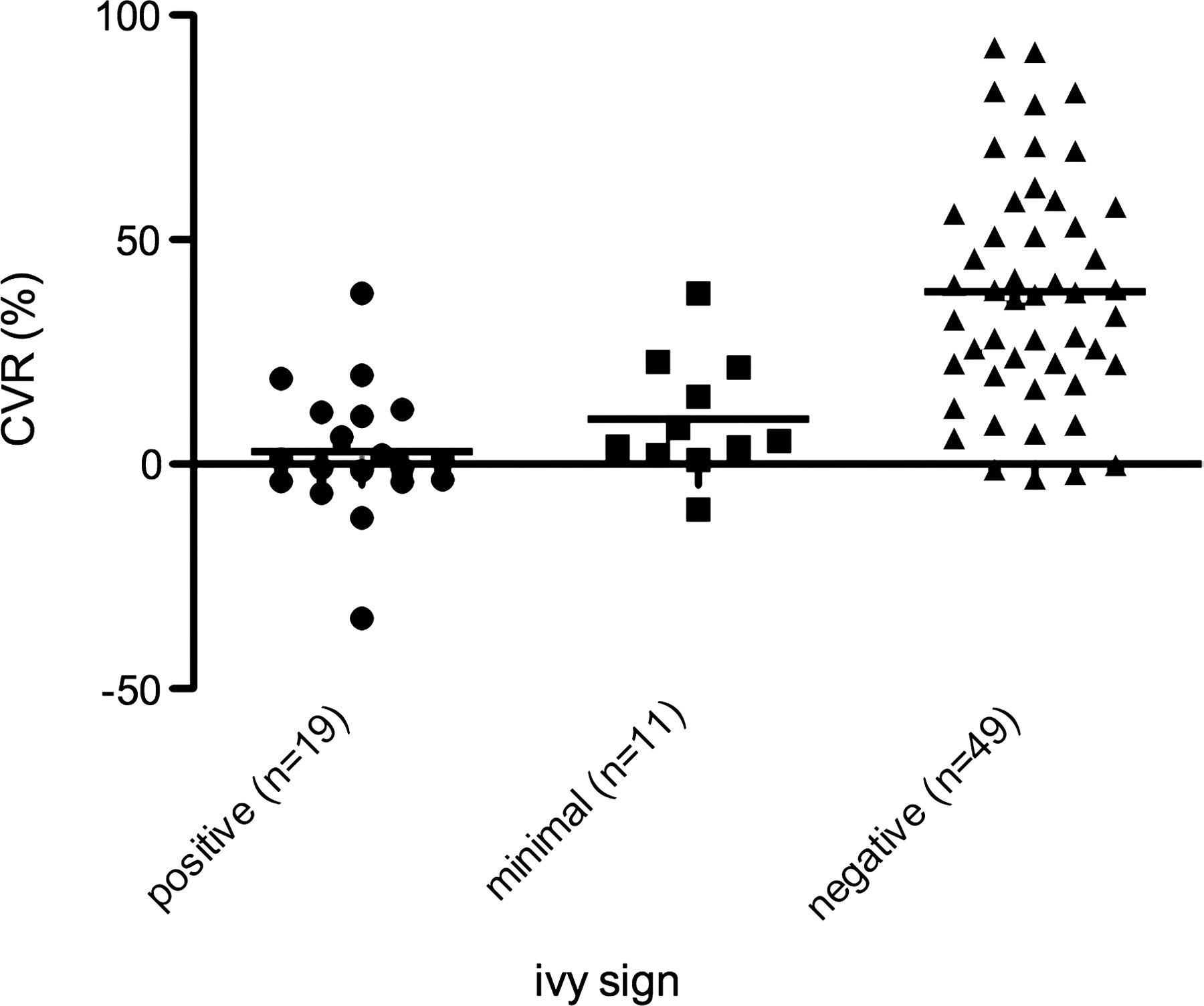
Correlation of ivy sign distribution with CVR before surgery (n = 79). The CVR was significantly lower in the areas with positive or minimal ivy signs than in the areas with no ivy signs (p < 0.05)
Postoperative evaluation
The distribution of the ivy sign before and after STA-MCA anastomosis was compared in 23 hemispheres of 16 patients. Seven patients underwent bilateral STA-MCA anastomosis, and the remaining nine patients underwent unilateral STA-MCA anastomosis. The ivy sign was positive in 14 hemispheres (33 regions) before surgery, and it had disappeared from 11 hemispheres (25 regions) and decreased in three hemispheres (eight regions) after surgery. The ivy sign was minimal in three hemispheres (12 regions) before surgery, and it had disappeared in all of these hemispheres after surgery. No ivy sign was seen in the remaining six hemispheres (45 regions) before and after surgery.
In 12 untreated hemispheres of 12 patients, the ivy sign was positive or minimal in six hemispheres (16 regions) before surgery and had disappeared in one (four regions) and decreased in five hemispheres (three regions).
Of the 12 patients who underwent perfusion SPECT before and after surgery, seven patients underwent bilateral STA-MCA anastomosis, and the remaining five patients underwent unilateral STA-MCA anastomosis. Perfusion SPECT demonstrated hemodynamic improvement in the areas in which the ivy sign had disappeared or decreased after surgery.
CVR significantly improved after surgery in the areas demonstrating positive or minimal ivy signs before surgery (p = 0.0001 and p = 0.0010, respectively) (Fig. 4). The median CVR rose from 2.84 to 24.2 in the areas with positive ivy signs and from 10.1 to 26.0 in the areas with minimal ivy signs.
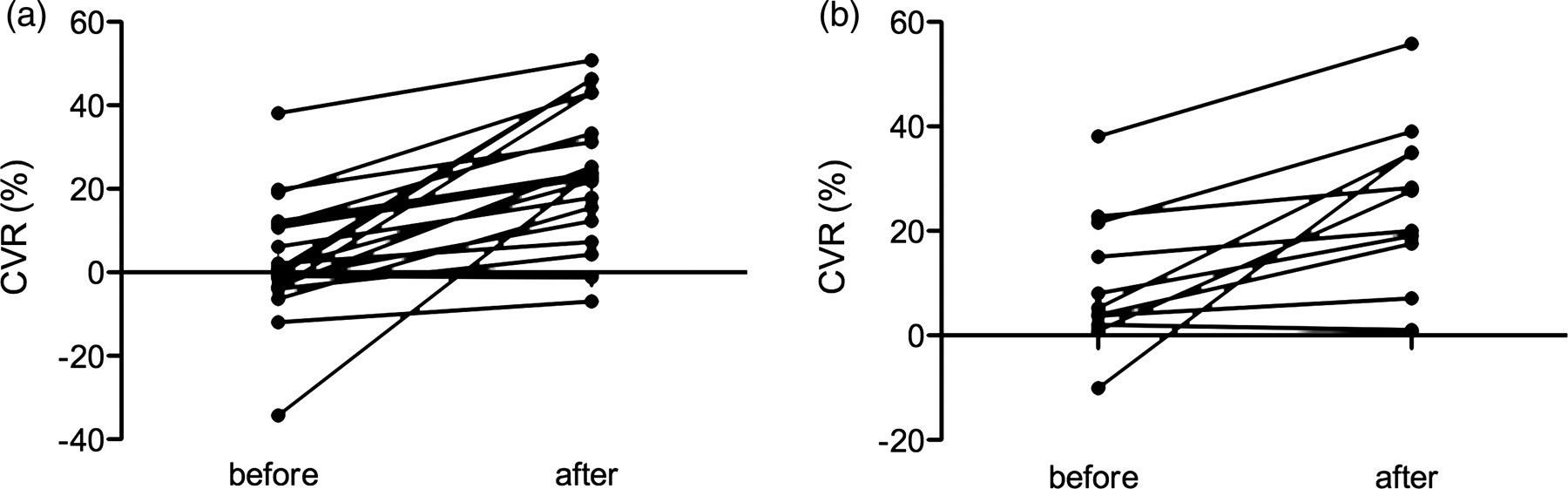
CVR before and after bypass surgery in the areas with positive or minimal ivy signs. The CVR was significantly improved in the areas with (a) positive or (b) minimal ivy signs after surgery (p < 0.05). The median CVR in the areas with positive ivy signs rose from 2.84 to 24.2 and that in the areas with minimal ivy signs rose from 10.1 to 26.0. (a) Cases with positive ivy signs (n = 19), (b) cases with minimal ivy signs (n = 11)
Discussion
The ivy sign was first reported as an indirect sign of Moyamoya disease seen on post-contrast T1-weighted MR images (6). Recent studies have shown that it can also be demonstrated on FLAIR images (10, 11, 14). We evaluated the change in ivy sign appearance on FLAIR images before and after surgery and compared it with the results of SPECT studies.
This study showed that the ivy sign is seen more frequently in the ACA and MCA regions than in the PCA region on FLAIR images. Previous studies have also shown a similar ivy sign distribution pattern on FLAIR images; it was predominantly seen in the frontal and parietal lobes compared to the temporal and occipital lobes, and no ivy sign was seen over the cerebellum or brain stem (11, 13). This ivy sign distribution pattern corresponds to the distribution of leptomeningeal collateral vessels in Moyamoya disease, which are less common in the PCA area, reflecting the fact that the posterior circulation is relatively well maintained in most patients with Moyamoya disease (8, 11, 13).
This study showed the clinical significance of the appearance of the ivy sign on FLAIR images before and after bypass surgery by comparing the ivy sign findings with those of perfusion SPECT imaging. Perfusion SPECT imaging is the standard procedure for measuring CBF and CVR during preoperative and postoperative assessments. However, because measuring CVR with SPECT is time-consuming and requires continuous arterial blood sampling, it is not a repeatable procedure. We investigated the role of non-contrast MR imaging as an alternative to SPECT imaging. Several studies have reported that the ivy sign was diminished on contrast-enhanced MR images after bypass surgery (9, 12–14). However, little is known about the significance of ivy sign appearance on FLAIR images after bypass surgery. In this study, CVR was significantly decreased in the areas with positive or minimal ivy signs compared with the areas that were negative for the ivy sign, a finding that was concordant with those of other studies (3, 12). This study also showed that the ivy signs detected on FLAIR images disappeared or decreased after surgery and that the distribution of the diminished ivy signs matched that of the areas showing hemodynamic improvement on SPECT, and we also found that the degree of CVR improvement in the areas demonstrating positive ivy signs before surgery was greater than that in the areas with minimal ivy signs. Thus, the presence of the ivy sign on FLAIR images was revealed to be an indicator of cerebral hemodynamic status before and after bypass surgery in Moyamoya disease.
According to the study by Yoon et al., the ivy sign is more commonly depicted on contrast-enhanced T1WI (CE-T1WI) than on FLAIR images; CE-T1WI revealed ivy signs in 71% of cases, whereas FLAIR images depicted them in 46% (14). The appearance of the ivy sign on CE-T1WI and FLAIR images may not reflect the exact same phenomenon. On CE-T1WI, the leptomeningeal enhancement observed in Moyamoya disease can be explained by the pial network being subjected to leptomeningeal anastomosis and the presence of pial vessels with thickened arachnoid membranes (10, 14). In our study, the ivy sign on FLAIR images disappeared or decreased after surgery in the areas with improved CBF or CVR. Fujiwara et al. reported that more prominent ivy signs were observed in hemispheres in which cortical branches of the middle cerebral arteries were poorly visualized on MR angiography (11). These findings support the hypothesis that the appearance of the ivy sign on FLAIR images largely reflects the status of the leptomeningeal collateral arteries rather than thickening of the leptomeninges. Further evaluation is necessary to prove the efficacy of FLAIR images compared with contrast enhancement MR images for evaluating cerebral hemodynamic status in Moyamoya disease.
The ivy sign on FLAIR disappeared or decreased not only on the operative side but also in the contralateral hemisphere after unilateral bypass surgery. Some investigators have demonstrated an increased CVR in both hemispheres after unilateral bypass surgery (18, 19), which is consistent with the results of our study. The mechanism of the hemodynamic improvement of untreated hemispheres is still uncertain. Honda et al. reported that regional CBF only significantly increased in the frontal lobe after surgery, which could have been due to collateral flow through the anterior communicating artery (18). Lim et al. found that the ACA steal phenomenon was occurring through the anterior communicating artery in 9% of patients with Moyamoya disease (20). After re-vascularization surgery, this steal phenomenon disappeared or diminished due to the development of new leptomeningeal collateral vessels on the treated side (20). Based on the results of these studies, we speculate that the circulation of the untreated hemisphere increases through improved collateral flow or regression of the steal phenomenon via the anterior communicating artery.
There are a couple of limitations in our study. We did not perform contrast enhanced MRI, and could not compare the distribution of the ivy sign on FLAIR images with that on contrast enhanced MRI. Second limitation is the field strength of the MR scanner. Although optimal field strength to visualize the ivy sign is uncertan, the frequency of the ivy sign may increase with use of higher magnetic field. Kawashima et al. reported that the frequency of ivy sign visualization on FLAIR images in Moyamoya disease was 97.1% (34/35 patients) using a 3.0T scanner (21).
In conclusion, FLAIR imaging is a non-invasive and useful technique for assessing the hemodynamic status of leptomeningeal collateral pathways in Moyamoya disease. The disappearance of the ivy sign indicates hemodynamic improvement after revascularization surgery.
Footnotes
Acknowledgements
We thank Dr S Honda (Department of Public Health, Nagasaki University Graduate School of Biomedical Sciences), for his contributions to the statistical analysis.