
Abstract
Background
Periportal edema (PPE) can be seen in different clinical settings, including in patients following trauma. However, the underlying mechanisms and clinical significance in trauma patients still remain unclear.
Purpose
To determine the incidence of PPE in CT scans of trauma patients and to correlate PPE with trauma severity and different patterns of injury.
Material and Methods
We retrospectively analyzed contrast-enhanced spiral CT scans of 127 trauma patients that were referred to our Trauma Center Level I between January 2006 and June 2007. According to the Injury Severity Score (ISS), 70 patients with an ISS < 16 (minor trauma) were assigned to group 1 and 57 patients with an ISS ≥16 (major trauma) to group 2.
Results
The presence of PPE was significantly (p < 0.01) higher in group 2 (22 of 57 patients [38.6%]) than in group 1 (10 of 70 patients [14.3%]). In 29 patients PPE presented with a diffuse pattern and in three patients with a focal pattern, affecting only one liver lobe. In 14 patients PPE was found in absence of abdominal injuries. In addition, PPE was present in five patients with abdominal injuries but without liver injury.
Conclusion
PPE is seen significantly more often on abdominal CT scans following major traumas (ISS ≥ 16), but is not necessarily associated with liver injury.
Keywords
Periportal edema (PPE) is defined as a circumferential zone of low attenuation around subsegmental portal venous branches seen on contrast-enhanced computed tomography (CT) scans (1). These low attenuation zones may represent fluid, either blood or edema, or dilated lymphatic vessels (2, 3). Periportal edema can be seen in different clinical settings, for example following liver or bone marrow transplantation, malignancies, or cardiac failure (3–5). It has been described in patients following trauma (6–11). However, the underlying mechanisms and clinical significance of periportal edema in trauma patients still remain unclear. The purpose of this study was to compare the frequency of PPE in patients with minor and major trauma and to correlate these data with distribution of injuries.
Material and Methods
One hundred and twenty-seven patients with blunt or penetrating injuries who were admitted to our Trauma Centre Level I and underwent major trauma management between January 2006 and June 2007 were enrolled in this retrospective study. All patients were initially assessed upon admission to the emergency department (ED) and immediately categorized using the ISS. Standardized trauma management included shock room diagnostic followed by a whole-body CT scan, which included scans of the brain, cervical spine, chest, and abdomen on a multislice CT (MSCT) with 6-detector rows (Emotion 6; Siemens, Erlangen, Germany). The base of the skull was scanned sequentially at 130 kV and 260 mAs and the neurocranium was scanned sequentially at 130 kV and 300 mAs with a collimation of 1 mm. The midface and cervical spine was scanned at 130 kV and 120 mAs with a collimation of 1 mm and a pitch factor of 1.5. The thorax and abdomen were scanned at 110 kV and 180 mAs with a collimation of 2 mm and a pitch factor of 1.5. Primary reconstructions were performed in the axial plane with a slice thickness of 2.5 mm and 5 mm for the thorax and abdomen and with a slice thickness of 1.25 mm and 2 mm for the midface and cervical spine. In addition, secondary sagittal and coronal multiplanar reconstructions (MPR) were performed for all regions. Thoracic-abdominal imaging was performed 60 s after administration of 120 mL of a CT contrast medium (Accupaque 300; GE Healthcare, Munich, Germany) in adults. In children, the contrast medium was administered according to the patient's weight (1.5 mL/kg).
CT scans were retrospectively reviewed by two radiologists (both with 3 years of experience in emergency radiology) blinded to clinical data in consensus mode on a PACS workstation. For assessment of PPE on abdominal scans both the 2.5 mm and 5 mm thick axial images as well as the sagittal and coronal MPRs were evaluated. PPE was diagnosed when circumferential zones of low attenuation were seen around a second rank portal vein branch. PPE was further characterized by distribution within the liver. PPE in one lobe was differentiated from involvement of both lobes (12).
In addition, the underlying traumatic injuries were analyzed. Abdominal injury was defined as damage of abdominal parenchymatous organs. In addition, we differentiated whether liver damage was present or not in patients with abdominal injury. Thoracic-abdominal fractures were defined as osseous lesions of the ribs and vertebral spine excluding pelvic fractures, which were analyzed separately. Cephalic fractures were defined as osseous lesions of the neurocranium, base of the skull and midface. Intracranial bleeding was analyzed separately.
The severity of injury was assessed by the Injury Severity Score (ISS), based on the Abbreviated Injury Scale (AIS) on admission to the emergency department (13, 14). Patients were assigned to two groups according to their Injury Severity Score. Patients with an ISS < 16 were assigned to group 1. Patients with an ISS ≥ 16 were classified as major trauma and assigned to group 2. The incidence of PPE and the distribution of injuries in both groups were compared.
Mean values and standard deviations as well as statistical analysis were tabulated and analyzed using the Statistical Package for Social Sciences (SPSS for Windows Package 15.0, Chicago, IL, USA). Results are depicted as mean ± SEM. Fisher's exact test was used to analyze differences between specific groups.
Results
Seventy patients (53 men and 17 women, mean age 46.8 years ± 19.0) had an ISS < 16 (group 1) and 57 patients (38 men and 19 women, mean age 42.6 years ± 21.2) an ISS ≥ 16 (group 2). Three patients (4.3%) in group 1 and five patients (8.8%) in group 2 were aged 18 years or younger.
PPE was present in 10 of 70 patients (14.3%) in group 1 in 22 of 57 patients (38.6%) in group 2 (p < 0.01) (Figs. 1 and 2). In 29 patients PPE presented with a diffuse pattern and in three patients, all assigned to group 2, with a focal pattern, affecting only one liver lobe.

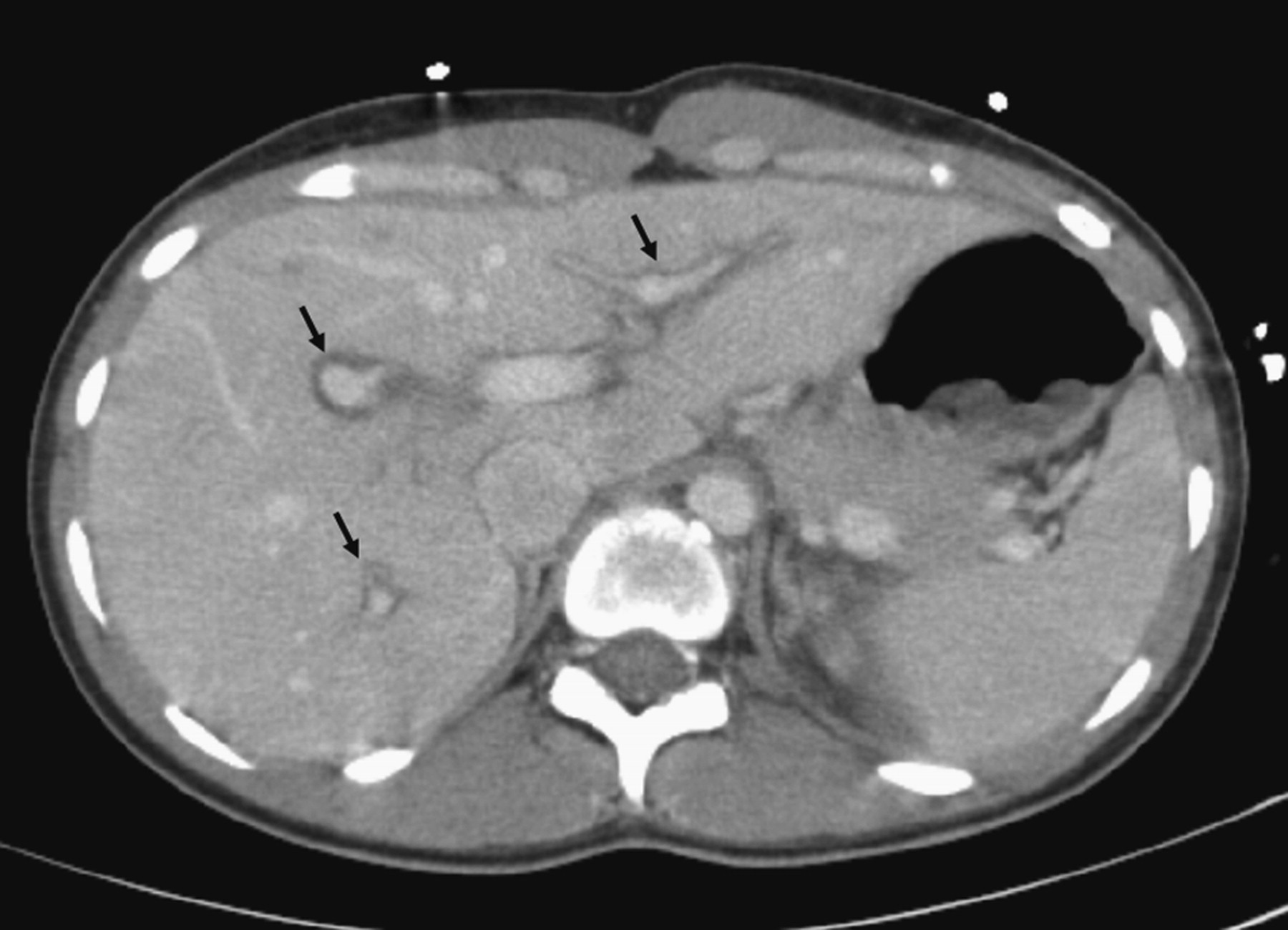
CT scan of a 42-year-old male patient following impact trauma shows diffuse collars of low density surrounding central and peripheral portal vein branches (see arrow heads) at the level of the coeliac trunc without evidence of abdominal injury
A 33-year-old female patient following a motor vehicle accident. Diffuse periportal low density is detected around peripheral portal vein branches (see arrow heads)
None of the patients assigned to group 1, but three patients (5.3%) in group 2 exhibited PPE in combination with abdominal injury including liver damage. PPE joined to abdominal injury without liver damage was not detected in group 1 but in five patients (8.8%) assigned to group 2. In both patterns of injury, no statistical correlation between trauma severity and PPE was found.
PPE in absence of abdominal injury was seen significantly more often (p < 0.001) in patients with an ISS ≥ 16 (14 patients; 24.6%) as compared to patients with an ISS < 16 (0 of 70). PPE in combination with thoracic-abdominal fractures and pelvic fractures was significantly more frequent in group 2 (14 patients; 24.6% and eight patients, 14.0%, respectively) than in group 1 (three patients; 4.3% and 0 patients, respectively) (p < 0.01, Table 1). In three patients (4.3%) with an ISS < 16 and in eight patients (14.0%) with an ISS ≥ 16 PPE was found in combination with cephalic fractures or in combination with intracranial bleeding. PPE and fractures of extremities were seen in two patients (2.9%) assigned to group 1 and in eight patients (14.0%) assigned to group 2 (Table 1).
Incidence of periportal edema (PPE) in combination with different patterns of injury in group 1 (ISS < 16) and group 2 (ISS ≥ 16)
In five of 32 (15.6%) trauma patients with PPE cephalic injuries were seen as the only trauma manifestation.
Age and gender did not differ significantly between group 1 and 2 in patients with PPE.
Discussion
Anatomically, the lymphatic drainage of the liver depends on two main systems consisting of an intrahepatic and an extrahepatic segment (15). These two systems are not separated strictly, as the intrahepatic lymphatic system, which is formed by the interlobar connective tissue surrounding the portal blood vessels and bile ducts, drains into the extrahepatic lymphatic system. The extrahepatic lymphatic system drains the hepatic lymph via collecting vessels running along the portal veins. A remaining small percentage is draining into lymphatic vessels accompanying the hepatic veins (8). Physiologically, the hepatic lymphatic system cannot be detected by computed tomography, but becomes visible when the drainages are obstructed or the lymph production is increased (8).
The circumferential zones of decreased attenuation around portal venous branches in contrast-enhanced computed tomography are described as morphologic correlate for fluids, like tracked blood due to liver injury or lymphedema or dilated lymphatic vessels (3).
The pathophysiological and clinical significance of PPE in trauma patients is still not fully understood. In our study PPE was found to be significantly more frequent following major trauma (38.6%) than minor trauma. Shanmuganathan et al. postulated that the diffuse low attenuation paralleling the portal veins in polytraumatic patients is caused by distension of periportal lymphatic vessels and accumulation of lymphedema (8).
Several studies indicate that diffuse PPE in trauma patients might be caused by the acute elevation of central venous pressure compressing the discharge of the hepatic lymphatic system (5, 8). It has been suggested that the incidence of PPE is associated with a high fluid load during the prehospital trauma life support (16). This assumption is supported by Patrick et al., who attributes periportal low attenuation rather to lymphatic dilatation than to periportal hemorrhage as they documented PPE in patients with no evidence of manifest liver injury (17).
In non-trauma patients, PPE has been described in connection with malignant lesions of the liver, such as juvenile chronic myelogenous leukemia or the undifferentiated hepatoblastoma causing lymphadenopathy or tumor manifestation in the porta hepatis, which leads to lymphatic obstruction and consecutive lymphatic dilatation and lymphedema (4). Furthermore, zones of PPE have been associated with hepatic disorders like hepatitis, bile duct proliferation, perivascular inflammation following bone marrow, or liver transplantation or congestive heart failure, which may lead to an increased venous pressure (3). Koslin et al. described intrahepatic perivascular hypodense zones in 12 patients suffering from cardiac decompensation and consecutive hepatomegaly causing an increased venous pressure engendering enhanced fluid formation in the hepatic interstitial compartment (9, 15).
The disruption of small trigonal vessels and laceration of adjacent hepatic parenchyma, which cause bleeding tracks along the low resistance connective tissue sheaths, may also play a role in the development of PPE in trauma patients. These sheaths surround portal triads and can easily be dissected by blood (11). Sivit et al. examined 400 children with blunt abdominal trauma. In the majority (79%) of the patients with hepatic injury they found PPE. However, Sivit el al. point out that most of the patients (62%) presenting PPE did not have a specific hepatic injury (12).
Our study has several limitations: one major drawback is that we did not analyze the amount of intravenous (i.v.) fluid application prior to the CT examination as these data were not available. However, the amount of i.v. fluid may play a role in the development of PPE as it influences central venous pressure, which is reported to be elevated in trauma patients with PPE (8). In addition, we were not able to evaluate the influence of PPE on the duration of hospitalization and clinical outcome, as a significant number of the examined patients were transferred to secondary hospitals.
In conclusion, periportal edema is seen significantly more often following major trauma (ISS ≥ 16) than minor trauma (ISS < 16). Its presence on abdominal CT scan might therefore be considered as an indicator of severe injury. However, PPE is not necessarily associated with abdominal or liver injury.