
Abstract
Background
With the increasing use of multidetector computed tomography (MDCT), the number of incidentally detected ventricular septal aneurysms (VSAs) in adults has increased. However, to date, there are not sufficient well-organized data regarding VSAs in adults on MDCT.
Purpose
To evaluate the CT findings of ventricular septal aneurysms (VSAs) in adults and correlate the findings with clinical features.
Material and Methods
We performed a retrospective review of the cardiac CT reports in our electronic database of 3402 patients who underwent ECG-gated cardiac CT scans using a 64-slice multidetector CT or dual-source CT from October 2006 to December 2009 at our institute. Among them, eight patients were diagnosed with a VSA. We evaluated the location, size, and morphology of VSAs on cardiac CT angiographies (CCTAs) and correlated the findings with the clinical features of the patients.
Results
On CCTAs, all eight patients were found to have VSAs in the membranous portion of the interventricular septum and toward the right ventricle. The VSAs were 10–22 mm at their longest diameter and had wide necks. The VSAs were lobulated along the outer margin and were incidental findings in all patients. Four of the eight patients had a conduction abnormality such as first-degree atrio-ventricular block or incomplete right bundle branch block seen on ECG, whereas the other four patients had normal ECGs.
Conclusion
VSA in adults is usually detected incidentally. It is seen in the membranous portion of the interventricular septum with a lobulated shape on CCTA. It is occasionally associated with a conduction anomaly.
An aneurysm of the interventricular septum is a rare condition. Rae (1936) reported four membranous ventricular septal aneurysms in 3000 autopsies (1), and Graffigna et al. (2) reported that the incidence of ventricular septal aneurysms (VSAs) is 0.3% in patients with congenital heart disease. Mall et al. (3) concluded that aneurysms occur in children when the membranous septum, congenitally weakened by a mildly dextroposed aorta, is placed in a somewhat horizontal position. There are also many reports concerning children with small, membranous, ventricular septal defects (VSDs) accompanied by aneurysm formation (4–10). VSDs associated with an aneurysm of the membranous septum tend to spontaneously decrease in size or to close more frequently than do defects without such an aneurysm. VSAs are occasionally caused by increased atrial or ventricular pressure or by endocarditis (4, 11, 12).
VSAs are traditionally imaged by echocardiography or cardiac angiography (12). With the increasing use of cardiac magnetic resonance imaging (MRI) and multidetector computed tomography (MDCT) for non-invasive cardiac imaging, the number of incidentally detected VSAs in adults has increased. Dodd et al. (12) reported three cases of cardiac septal aneurysms mimicking pseudomasses on ECG-gated MDCT. However, to date, there are not sufficient well-organized data regarding adults with VSAs on MDCT images. Therefore, we evaluated the imaging findings of VSAs in adults as seen by ECG-gated MDCT and the associated clinical features of these patients.
Material and Methods
A total of 3402 adult patients did undergo contrast-enhanced cardiac CT angiography (CCTA) at our institution between October 2006 and December 2009. We retrospectively reviewed the cardiac CT reports using an electronic database through the text search. Among these patients, eight were diagnosed with a VSA. The clinical and imaging features of those eight patients were evaluated. The mean age was 59 years (range 48–75 years), four were men and four were women. The patients underwent CCTA to evaluate chest pain (n = 2), dyspnea (n = 1), ECG abnormality (n = 1), palpitation (n = 1), high risk of coronary artery disease (n = 2) or significant abnormality of the intima-media thickness on the carotid ultrasonography (USG) (n = 1). Of the eight study patients, four had histories of hypertension, two had diabetes mellitus, and four had hyperlipidemia (Table 1). One patient had a history of myocardial infarction 10 years ago, but there was no recent history of cardiac events in any of the patients.
Clinical characteristics (CC) of patients with ventricular septal aneurysms
MR = mitral regurgitation, TR = tricuspid regurgitation, LVH = left ventricular hypertrophy, VSA = ventricular septal aneurysm, DM = diabetes mellitus, CAD = coronary artery disease, MI = myocardial infarction, N/A = not available
Three patients were scanned with a 64-slice MDCT (Lightspeed VCT 64; GE Healthcare, Milwaukee, WI, USA) and five patients were scanned with dual-source CT (DSCT) (Somatom definition, Siemens, Erlangen, Germany). For patients scanned with 64-slice MDCT, if a patient's heart rate exceeded 65 bpm, heart-rate control was achieved with the oral beta-blocker, propranolol hydrochloride (Indenol@, DongKwang Phama Co. Ltd., Seoul, Korea) except in the event of contraindications regarding the beta-blocker. For 64-slice MDCT, examinations were acquired in the craniocaudal direction using a slice thickness of 0.625 mm, a tube voltage of 100–120 kVp (depending on the BMI), and a tube current of 600 mAs. The ECG-triggered tube current modulation was switched on at 50% of the R-R interval.
For patients scanned with DSCT, if a patient's heart rate exceeded 80 bpm, heart-rate control was achieved by an intravenous selective beta1-blocker, esmolol (Jeil Brevibloc@, Jeil Phama Co., Ltd., Seoul, Korea). Scanning parameters were as follows: 100–120 kVp (depending on BMI), 350 mAs, 0.33 sec/rotation, 0.36 pitch, tube current modulation using ECG pulsing, 0.75-mm slice thickness, and 0.5-mm reconstruction increment.
We used a two-phase contrast media protocol that was adjusted to the scan duration. The first phase consisted of the administration of 80 mL of contrast agent (Iopromide, Ultravist 300; Bayer Schering Pharma AG, Berlin, Germany) at a rate of 4–5 mL/s for 16 seconds, while the second phase included the administration of 50 mL of 15% contrast medium and 85% saline solution or 100% saline at a rate of 4–5 mL/s for 10 s. We used the 100% saline as a chaser with earlier patients (n = 1150), and then we changed to contrast mixture as a chaser (n = 2252) because it is better for evaluating the right heart.
Retrospective data analysis was available in the most motionless phase of the cardiac cycle, which was most frequently the mid-diastolic phase (75% of the R-R interval). Assessments were performed by two radiologists (MC, JIJ) by consensus. VSAs were defined as notable aneurysms protruding into the right ventricle via the interventricular septum. We measured the longest diameter of the aneurysm and the longest diameter of the neck of the aneurysm on axial images. If the diameter of the neck was more than half of the longest diameter of the aneurysm, we defined the aneurysm as having a wide neck. We also evaluated the clinical data of the patients. All study patients performed standard, 13-lead ECG as part of routine examination. Echocardiography was performed in seven patients for the evaluation of left ventricular function because of ECG abnormalities (n = 5), hypertension (n = 1), or previous myocardial infarction with conduction abnormality (n = 1).
These clinical tests and CCTAs were performed within two years of each other without interim cardiac events, and most of the clinical tests were performed before the CCTAs. The institutional review board of our institute approved this study.
Results
The clinical data are summarized in Table 1. On the ECGs, conduction anomalies were noted in four patients, including an incomplete right bundle branch block (RBBB) (n = 2), and a first-degree atrio-ventricular (AV) block with or without incomplete RBBB (n = 2). The remaining four patients showed no significant ECG abnormality.
Imaging findings from contrast-enhanced, coronary CT angiography in patients with ventricular septal aneurysms
IVS = interventricular septum, LAD = left anterior descending artery, RCA = right coronary artery, LCx = left circumflex artery, LV = left ventricle
Echocardiography was performed in seven patients, and VSAs were detected in two of them. VSAs were not detected in the other five patients. In the five patients in whom VSAs were not detected, the echocardiographs reported non-specific minor findings in two patients, old inferior wall myocardial infarction in one patient and were negative for the other two patients.
On CCTA, VSAs appeared as bulges with a distinct margin protruding into the right ventricle via the interventricular septum just under the aortic valve in all eight patients (Figs. 1 and 2). The longest diameter was 10–22 mm (median 16 mm), and all VSAs had wide necks (median 12 mm). The walls of all of the aneurysms were lobulated (Figs. 1 and 2). There was no morphological difference between VSAs with conduction abnormality and VSAs without conduction abnormality. On CCTAs, four patients showed normal coronary artery findings. Three patients had insignificant coronary artery stenosis, and one patient had a thrombosed occlusion of the right coronary artery (Table 2).
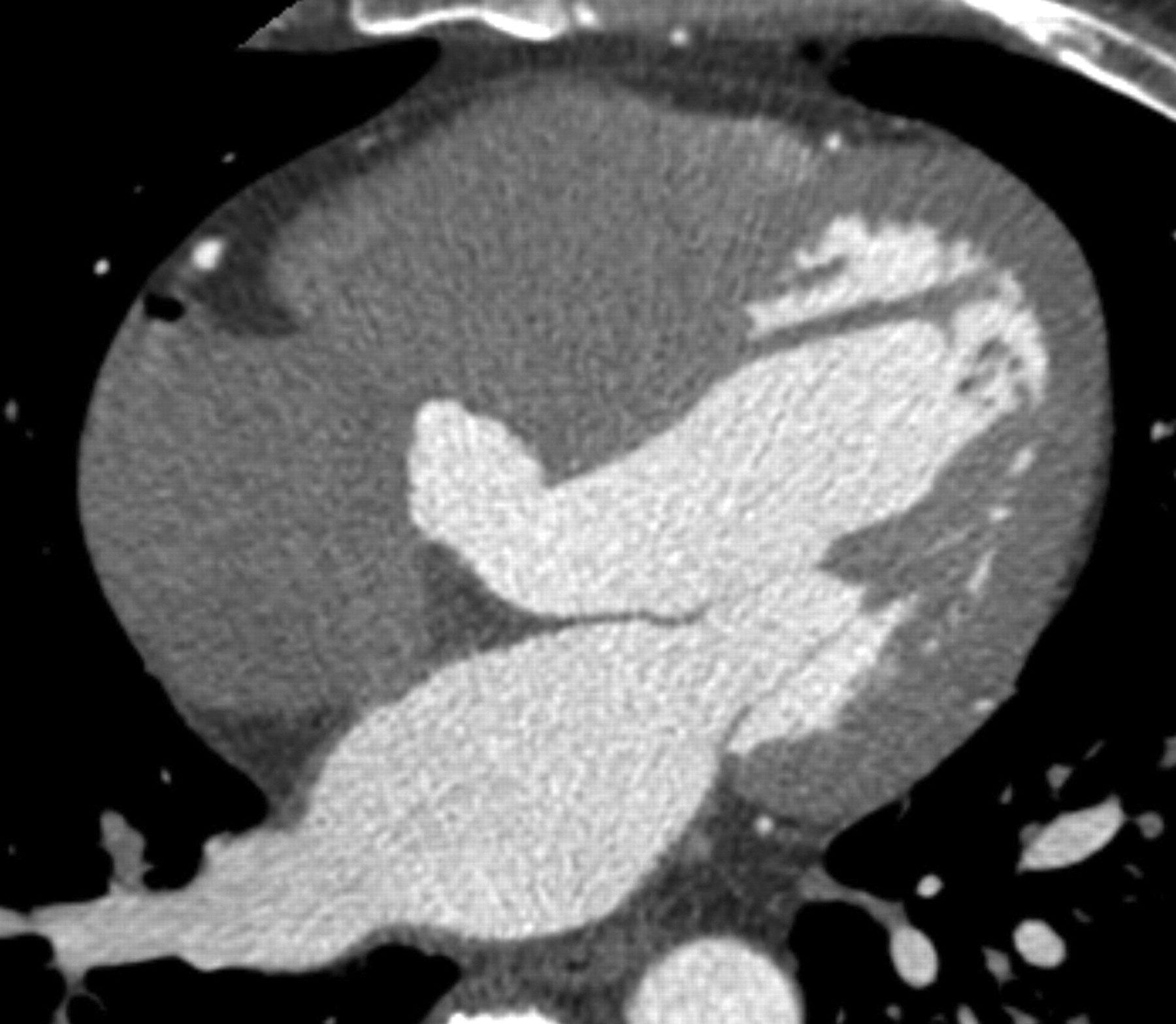
A 49-year-old man with an interventricular septal aneurysm detected on an echocardiogram. A lobulated, out-pouching lesion (about 19 mm at the largest diameter) with a wide neck (about 13 mm at the largest diameter) is noted in the membranous portion of interventricular septum on axial view on the coronary CT angiography. ECG was normal
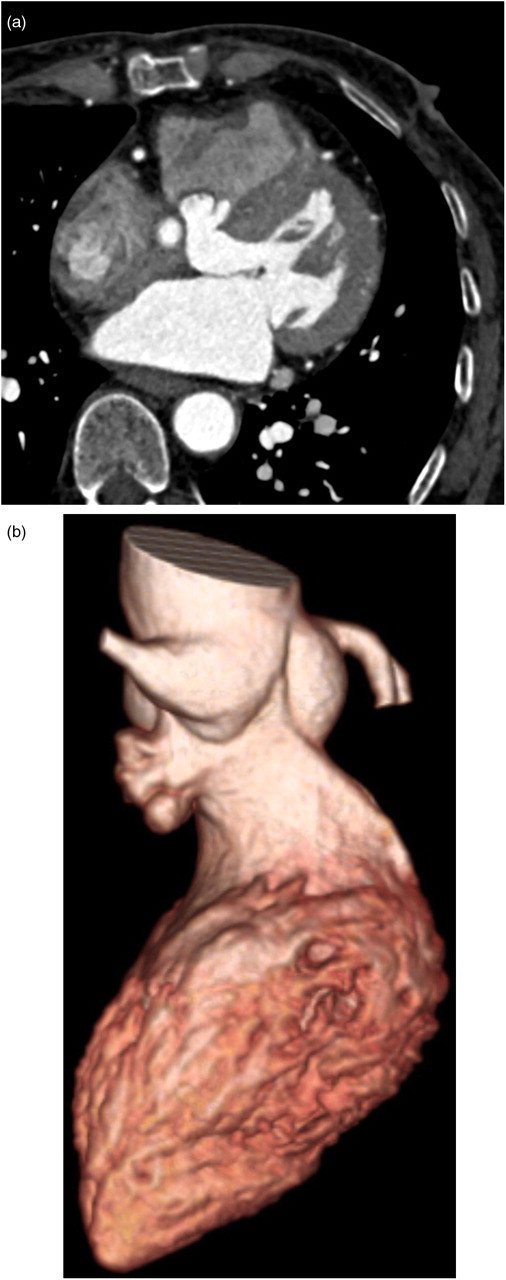
A 68-year-old woman evaluated coronary CT angiography because of increase of intima-media thickness on carotid ultrasonography with underlying diabetes mellitus. Axial image (a) and volume rendering image (b) of the CCTA shows a lobulated out-pouching lesion measuring approximately 15 mm at its longest diameter in the membranous portion of the ventricular septum. ECG revealed an incomplete first degree AV blockage
Discussion
Ventricular septal aneurysm has been recognized for years as frequently associated with perimembranous ventricular septal defects (VSDs). Numerous pathology and clinical studies (4–10) have indicated that VSDs associated with aneurysms of the membranous septum tend to spontaneously decrease in size or to close more than defects without such aneurysms. However, the mechanism of closure remains largely speculative (13–18).
In a review of 69 specimens of hearts with perimembranous VSD, Anderson et al. (13) found that 38% of the specimens had anatomical evidence of partial or complete closure of tissue arising from the vicinity of the tricuspid valve and the membranous septum. In most cases, the tissue was derived from the tricuspid valve (84%), from prolapse of aortic leaflets in two cases (8%), and in only two (8%) did subaortic tissue tags arise from the membranous septum itself (13). These malformed or maladherent leaflets of the tricuspid valve, which resemble an aneurysm, have been described in autopsy specimens of patients with membranous VSD (14). Therefore, the term ‘aneurysm of the membranous septum’ is a misnomer in most cases, although it may be indistinguishable from ‘true aneurysm’ by angiography (15, 16). It was suggested that describing this entity as a ‘ventricular septal defect associated with restrictive tissue’ or as a ‘tricuspid restricted defect’ would be more appropriate (16). However, because of the wide acceptance of the term, limited clinical studies, and the lack of more precise terminology, Freedom et al. continued to use ‘aneurysm of the membranous septum’, although they compromised by adding ‘so-called’ to their title (17).
A prevalence of VSAs in adults has not been reported. In our study, the frequency of VSA was estimated to be approximately 0.24% (8/3402). However, the prevalence might be significantly underestimated in our study, because we retrospectively collected cases through cardiac CT reports using an electronic database.
Ventricular septal aneurysms in adults are associated with conduction arrhythmias such as ventricular tachycardia, atrioventricular block or bundle branch block (2, 19, 20). In a previous report, a His bundle originating from the atrio-ventricular (AV) node was placed on the wall of the right atrium around the tricuspid valve along the septal wall and thereby provoked abnormal contraction of the ventricular wall. Based on characteristic location of VSAs and interfering the action of His bundle, VSAs might become a focus of arrhythmia including ventricular tachycardia, AV block or bundle branch block. In our series, the arrhythmia frequency was found to be 50% (4/8). However, any morphological difference between VSAs with conduction abnormality and VSAs without conduction abnormality was not found in our study.
The differential diagnoses of VSAs are an aneurysm of the sinus of Valsalva and an accessory mitral valve tissue (14, 20). Aneurysm of the sinus Valsalva shows saccular dilatation of the aortic sinus on CCTA (21–25) whereas VSA shows an outpouching lesion which originates in the left ventricle immediately beneath the aortic valve. Accessory mitral valve tissue can be confused with a VSA. However, an accessory mitral valve is parachute or sail shaped with a variable number of well-defined chordae anchoring the ends to either or both papillary muscles of the mitral valve, to normal chordae, and to the left ventricular free wall (26, 27). This tissue is completely separate from the subaortic membranous septum (26).
VSA can induce several complications such as infectious endocarditis with or without thrombus formation, obstruction of the right ventricular outflow, and aortic and tricuspid insufficiency (4–11, 17, 18, 20, 28). Hence if a VSA is indentified incidentally on MDCT, it should prompt an assessment for these other functional abnormalities and an assessment for the presence of a persistent shunt as with echocardiography.
Echocardiography is known as a principal technique for diagnosis the congenital heart disease in adults (29). Transesophageal echocardiography, in particular, offers the potential for more accurate characterization of the aneurysm. However, diagnosis of VSA in adult with echocardiography as the first-line test greatly depends on the knowledge and skill of the operators. Interestingly only two cases with VSAs were detected by transthoracic echocardiography in the present study. This might be due to unfamiliarity with the particular problems of adult congenital heart disease such as VSA or operator's skill or the small size of VSAs.
There are several limitations to our study. One is the small sample size. We believe that a study with a large population will be necessary in order to determine the clinical significance of VSAs. Another limitation is that a very limited number of patients underwent confirmatory testing with Holter or echo. The third limitation is the shunt flow of a VSD. Because one of our patients did not undergo echocardiography, a patient might have a low level of shunt flow that was not detected on CT.
In conclusion, VSAs in adults are usually detected incidentally on CCTA. They occur in the membranous portion of the ventricular septum toward the right ventricle. VSAs are lobulated in shape and may be associated with conduction arrhythmias such as AV block or bundle branch block.