
Abstract
Background
Many collateral pathways to the liver are dissected during hepatobiliary pancreatic surgery and, if the arterial bleeding is massive and a hematoma becomes larger, the adjacent portal vein can be compressed with impairment of the portal venous flow.
Purpose
To evaluate the frequency and severity of ischemic liver injuries after hepatic artery embolization in patients with delayed postoperative arterial hemorrhage after hepatobiliary pancreatic surgery.
Material and Methods
Eighteen patients undergoing proper or common hepatic artery embolization for delayed postoperative arterial hemorrhage after hepatobiliary pancreatic surgery achieved hemostasis. To evaluate the frequency and severity of ischemic liver injuries, the liver enzyme levels and CT findings before and after hepatic artery embolization were retrospectively compared and the clinical outcomes after hepatic artery embolization were analyzed. Angiographic findings were also analyzed to reveal any association with development of ischemic liver injuries after hepatic artery embolization.
Results
Ischemic liver injuries were observed in 15 (83%) of 18 patients undergoing hepatic artery embolization for postoperative hemorrhage. Injuries included hepatic infarction combined with abscess in one (5%) patient, hepatic infarction in 12 (67%) patients, and transient hepatic ischemia/dysfunction in two (11%). As for the extent of hepatic infarction, lobar infarction developed in two patients and subsegmental infarction in 11. One patient with right hepatic lobar infarction died of hepatic failure 11 days after hepatic artery embolization. In the other 14 patients with ischemic liver injuries, the elevated liver enzymes returned to baseline levels within two weeks. All of the four patients with portal vein stenosis, four patients with no hepatic arterial flow on post-embolization angiogram, and one patient with both had hepatic infarction after hepatic artery embolization. No ischemic liver injuries developed after hepatic artery embolization in three patients with no portal vein stenosis and bilobar hepatic arterial flow via the left hepatic artery aberrantly arising from the left gastric artery or from the common hepatic artery.
Conclusion
Ischemic liver injuries can develop in most patients undergoing hepatic artery embolization for postoperative arterial hemorrhage after hepatobiliary pancreatic surgery; hepatic infarction appears to be the most frequent type of ischemic liver injury. Hepatic artery embolization for postoperative arterial hemorrhage after hepatobiliary pancreatic surgery may carry a great risk of ischemic liver injury if a patient has portal vein stenosis or no aberrant hepatic artery.
Delayed postoperative arterial hemorrhage is an unusual but life-threatening complication after hepatobiliary pancreatic surgery (1–4). It occurs mainly as a result of vascular erosion, potentially related to localized infection and anastomotic leakage, and has a mortality of up to 50% because of its insidious nature (3–7). Precise identification of the bleeding artery by surgical exploration is rarely successful due to postoperative adhesions; indeed, primary repair of the bleeding artery is related to high mortality and morbidity (2, 8). Therefore, immediate angiography and subsequent therapeutic embolization have been the first-line approach for delayed postoperative arterial hemorrhage after hepatobiliary pancreatic surgery (9, 10).
On the other hand, arterial occlusion by embolization can cause severe ischemic damage to the organ distal to the bleeding area, depending on the site and location of the bleeding artery. Hepatic artery embolization has been considered to be safe and widely performed because, when hepatic arterial flow is interrupted, the dual blood supply and extensive collateral pathways of the liver can serve to protect this organ from ischemic insults (9–11). Despite excellent results on controlling the bleeding (4, 9), previous studies have reported that up to 44% of patients undergoing hepatic artery embolization for delayed postoperative hemorrhage died of hepatic failure (10, 12–16). Those results have put the safety of hepatic artery embolization in surgical patients with postoperative hemorrhage up to debate. Moreover, application of an endovascular covered stent as an alternative to hepatic artery embolization has become increasingly available, with recent advances in stent technology (17–20). Thus, we think it is necessary to reveal the frequency and severity of ischemic liver injuries after hepatic artery embolization in patients with postoperative hemorrhage following hepatobiliary pancreatic surgery.
The aim of this study was to evaluate the frequency and severity of ischemic liver injuries following hepatic artery embolization in patients with delayed postoperative arterial hemorrhage after hepatobiliary pancreatic surgery.
Material and Methods
Institutional review board approval was obtained to enable the required retrospective review of patients' records, but informed patient consent was not required for this retrospective analysis. Between August 1996 and December 2008, 23 patients presenting with delayed postoperative hemorrhage after hepatobiliary pancreatic surgery were confirmed by angiography to have bleeding from the hepatic artery; 22 patients underwent emergent interventional treatment and one patient underwent surgical treatment to control bleeding. Interventional procedures performed in the 22 patients were hepatic artery embolization in 17 patients, selective embolization of the gastroduodenal artery stump in three patients, and covered stent placement on the hepatic artery in two patients. Hemostasis after interventional management was achieved in 21 patients except one, who died of continuous bleeding the day after coil embolization of the common hepatic artery. Two of the three patients who had undergone selective embolization of the gastroduodenal artery stump finally underwent hepatic artery embolization to treat rebleeding that occurred 6 and 27 days after initial embolization, respectively. Because this study intended to evaluate ischemic liver injuries after hepatic artery embolization, two patients who underwent hepatic artery embolization for re-bleeding after initial gastroduodenal artery stump embolization were included and one patient who died of continuous bleeding after hepatic artery embolization was excluded from the study. Eighteen patients who achieved hemostasis after hepatic artery embolization were enrolled in this study.
Clinical characteristics of the 18 patients are summarized in Table 1. There were 17 men and one woman, ranging in age from 42 to 74 years with a mean age of 58.8 years. The underlying diseases were common bile duct cancer in seven patients, ampulla of Vater cancer in three patients, pancreatic cancer in six patients, pancreatic and gastric cancer in one patient, and ampulla of Vater and gall bladder cancer in one patient. All patients had contrast-enhanced abdominal computed tomography (CT) scans taken as preoperative evaluation. Six patients had angiograms of the celiac and superior mesenteric arteries obtained before surgery because preoperative angiographic evaluation was routinely performed in our hospital until the year of 2000. The surgical procedures included pylorus preserving pancreatoduodenectomy in nine patients, Whipple's operation in six, and one each of Whipple's operation combined with right hepatic lobectomy, Whipple's operation combined with total gastrectomy, and Whipple's operation combined with resection of the left hepatic lateral segment. Thirteen patients had postoperative complications, including pancreaticojejunostomy leakage in six patients, hepaticojejunostomy leakage in three patients, wound infection in three patients, and intra-abdominal abscess in one. Bleeding occurred from 12 to 42 days (median 19.5 days) after the primary operation. Eight patients presented with gastrointestinal bleeding, eight patients presented with intraperitoneal bleeding (i.e. bleeding from the drain in the peritoneal cavity), and the other two patients presented with both gastrointestinal and intraperitoneal bleeding. Nine patients had abdominal CT scans before hepatic artery embolization that were performed to detect bleeding focus.
Clinical characteristics of 18 patients undergoing hepatic artery embolization for delayed postoperative arterial hemorrhage after hepatobiliary pancreatic surgery
*Re-bleeding after selective GDA stump embolization
AOV = ampulla of Vater, PPPD = pylorus preserving pancreatoduodenectomy, HJ = hepaticojejunostomy, PJ = pancreaticojejunostomy, BFD = blood from drain, POD = postoperative day, GDA = gastroduodenal artery
Hepatic artery embolization was performed as follows. Informed consent was obtained from all patients or their family members before the procedures. The diagnostic angiographies were performed with a 5-F angiographic catheter (Yashiro; Terumo, Tokyo, Japan; RH catheter, Cook, Bloomington, IN, USA) via a transfemoral route. Selective celiac, common hepatic, and superior mesenteric arteriographies were routinely performed to detect the bleeding points, and arterial portography was also taken to evaluate the patency of the portal vein. Bleeding was considered to be present when there was a pseudoaneurysm and/or extravasation of contrast media on angiography. The bleeding points were the gastroduodenal artery stump in 11 patients, proper hepatic artery in four patients, common hepatic artery in two patients, and both the gastroduodenal artery stump and proper hepatic artery in one patient. After identifying the bleeding point, a 3-F microcatheter (Microferret, Cook, Bloomington, IN, USA) was advanced into the hepatic artery to exclude the bleeding point, and then adequately sized platinum coils (Tornado/Nester, Cook, Bloomington, IN, USA) 0.018 inches in diameter were placed in the corresponding hepatic artery distal and proximal to the bleeding point. At the end of the procedures, common hepatic or celiac arteriography was performed to confirm cessation of the bleeding.
Liver function tests, including total bilirubin, aspartate aminotransferase (AST), and alanine aminotransferase (ALT), were routinely checked before and after hepatic artery embolization. Abdominal CT scans after hepatic artery embolization, which was available in all 18 patients, was obtained at the discretion of the clinician in order to confirm persistent occlusion of the pseudoaneurysm or to identify the development of complications. The interval between CT scans and hepatic artery embolization was 2–40 days (median 5.5 days).
To evaluate the frequency and severity of ischemic liver injuries, two radiologists working in consensus retrospectively compared liver enzyme levels and CT findings before and after hepatic artery embolization. Clinical outcomes after hepatic artery embolization were also analyzed. Nine patients did not have abdominal CT scans before hepatic artery embolization, so abdominal CT scans before surgery was instead used for the comparison. Hepatic ischemia or dysfunction was considered when there was an elevation of liver enzyme levels without new hepatic lesions on CT scan after hepatic artery embolization. Hepatic infarction was considered when there was an elevation of liver enzyme levels with new wedge-shaped or geographic low-attenuated lesions on CT scan after hepatic artery embolization. The extent of hepatic infarction was described as subsegmental, segmental, or lobar infarction. Liver abscess was considered when there was a new rim-enhancing low attenuated lesion on CT scan with clinical symptoms and signs of infection (i.e. fever, chilling, and leukocytosis). Angiographic findings (i.e. anatomical variation of the hepatic artery, >50% stenosis of the portal vein, hepatic arteries embolized, or presence of arterial blood flow to the liver on post-embolization angiograms) were also retrospectively analyzed to find any association with development of ischemic liver injuries after hepatic artery embolization. Interruption of gastroduodenal arterial flow by hepatobiliary pancreatic surgery could be a cause of ischemic liver injuries in patients with stenosis of the celiac artery, therefore all CT images and angiograms were reviewed to reveal if a patient had underlying stenosis (>50% in diameter) of the celiac artery.
Results
Ischemic liver injuries were observed in 15 (83%) of 18 patients undergoing hepatic artery embolization for delayed postoperative hemorrhage after hepatobiliary pancreatic surgery, which included hepatic infarction combined with gas-forming abscess in one (5%) patient, hepatic infarction in 12 (67%) patients, and transient hepatic ischemia/dysfunction in two (11%) patients. As for the extent of hepatic infarction, two patients had lobar infarction and 11 patients had subsegmental infarction (Fig. 1). Marked elevation (>1000 IU/L) of liver enzyme (AST or ALT) levels was found in four (36%) of 11 patients with subsegmental infarction as well as in two patients with lobar infarction (Table 2). Six patients had serum total bilirubin levels >2 mg/dl after hepatic artery embolization, and the elevated total bilirubin returned to baseline levels within two weeks in five of the six patients, except in one who died of hepatic failure. One patient (patient 2) with lobar infarction in the right hepatic lobe died of hepatic failure 11 days after hepatic artery embolization (Fig. 2); this patient had liver enzyme levels that were markedly elevated after embolization (AST up to 18900 IU/L, ALT up to 7650 IU/L). In the other 14 patients with ischemic liver injuries after hepatic artery embolization, the elevated liver enzymes returned to baseline levels within two weeks. However, one patient (patient 18) with subsegmental infarction died of acute heart failure secondary to myocardial infarction 15 days after hepatic artery embolization. Another patient (patient 12) with lobar infarction involving the left hepatic lobe and segment 1 required percutaneous drainage for combined gas-forming abscess. Except for two patients who died of hepatic failure or heart failure, the remaining 16 patients were discharged from the hospital 7–196 days (median 23.5 days; mean 36.8 days) after hepatic artery embolization and followed up for 1–73 months (median 24 months; mean 28.5 months). Two patients died of tumor recurrence at 17 and 68 months follow-up and 14 patients were alive until the time of investigation (n = 5), loss to follow-up (n = 7), or referral to local hospital (n = 2). Detailed results on patient outcomes and ischemic liver injuries after hepatic artery embolization in the 18 patients are presented in Table 2.
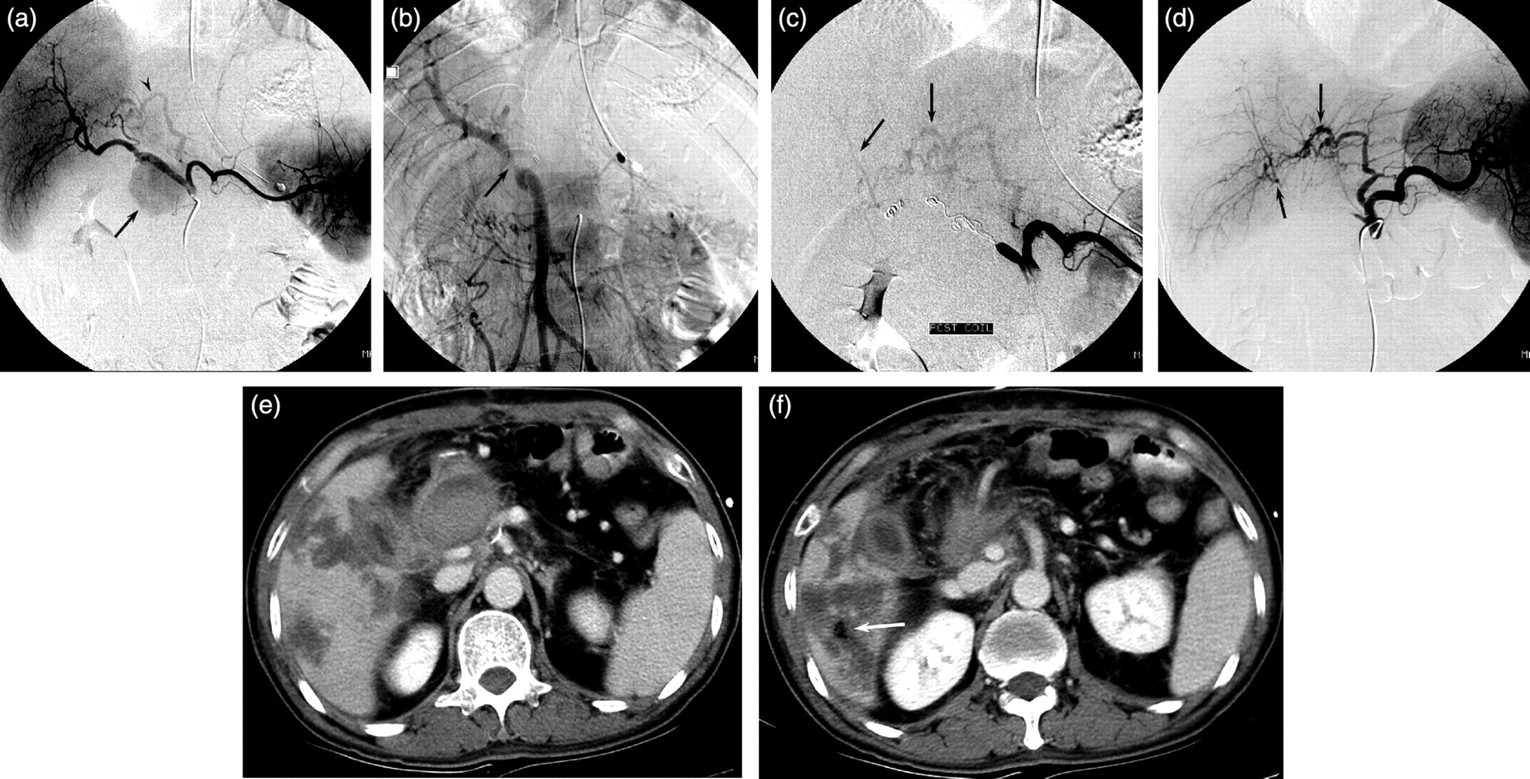
A 57-year-old man (patient 6) with subsegmental infarction after hepatic artery embolization. (a) Celiac angiogram shows a pseudoaneurysm (arrow) at the stump of the gastroduodenal artery and aberrant left hepatic artery (arrowhead) arising from the left gastric artery; (b) Superior mesenteric arterial portogram shows focal stenosis >50% at the main portal vein (arrow), probably due to extrinsic compression by the pseudoaneurysm; (c) Angiogram obtained immediately after coil embolization of the right to common hepatic arteries shows both complete exclusion of the pseudoaneurysm and bilobar hepatic arterial flow (arrows) via intrahepatic collaterals from the aberrant left hepatic artery; (d) Follow-up angiogram obtained 3 days after embolization clearly shows bilobar hepatic arterial flow (arrows) via the aberrant left hepatic artery; (e, f) CT scans obtained 3 days after embolization demonstrate geographic low attenuated lesions with an air bubble (arrow) in segments 5 and 6, representing subsegmental infarction. The serum AST and ALT levels were elevated from 24 IU/L and 32 IU/L before embolization to 589 IU/L and 499 IU/L after embolization, respectively. The patient was conservatively managed and discharged 14 days after embolization

A 63-year-old man (patient 2) with lobar infarction after hepatic artery embolization. (a) Celiac and (b) common hepatic angiograms show active bleeding (arrow) from the common hepatic artery; (c) On superior mesenteric arterial portogram, the main portal vein is not visualized (arrows), probably due to compression by a massive hematoma; (d) Angiogram obtained immediately after coil embolization of proper to common hepatic artery shows complete exclusion of the bleeding point and no hepatic arterial flow; (e) CT scan obtained 5 days after hepatic artery embolization demonstrates a large low-attenuated lesion containing air bubbles (arrows) in the entire right hepatic lobe, representing lobar infarction. The serum AST and ALT levels were elevated from 71 IU/L and 139 IU/L before embolization to 18900 IU/L and 7650 IU/L after embolization, respectively. The patient died of hepatic failure 11 days after hepatic artery embolization
Ischemic liver injuries and outcomes after embolization in 18 patients undergoing hepatic artery embolization for postoperative hemorrhage after hepatobiliary pancreatic surgery
HA = hepatic artery, LHA-LGA = replaced left hepatic artery from left gastric artery, LHA-CHA = left hepatic artery aberrantly arising from common hepatic artery, PVS = portal vein stenosis, P-CHA = proper to common hepatic artery, R-CHA = right to common hepatic artery, LHL = left hepatic lobe, BHL = both hepatic lobes, RHL = right hepatic lobe, RIPA = right inferior phrenic artery, LGA = left gastric artery, aLHA = aberrant left hepatic artery, RGA = right gastric artery, LIPA = left inferior phrenic artery, SS = subsegmental, AST = aspartate aminotransferase, ALT = alanine aminotransferase, T-bil = total bilirubin, FU = follow-up
Anatomic variation of the hepatic artery was observed in six (33%) of 18 patients; these variations included a replaced left hepatic artery arising from the left gastric artery in four patients and the left hepatic artery aberrantly arising from the common hepatic artery in two patients. Stenosis (>50%) of the main portal vein, probably resulting from the mass effect of a hematoma or pseudoaneurysm, was observed in five (28%) of 18 patients. As for the hepatic arteries that were embolized, 11 patients underwent embolization from proper hepatic artery to the common hepatic artery, and seven patients underwent embolization from the right hepatic artery to the common hepatic artery. The left hepatic artery was preserved from embolization in six patients who had a variation of the left hepatic artery. In 13 (72%) of 18 patients, post-embolization angiogram demonstrated hepatic arterial flow, which included bilobar hepatic arterial flow in seven patients (via intrahepatic collaterals from the aberrant left hepatic artery in five patients and extrahepatic collaterals in two patients), left hepatic arterial flow in four patients (via the aberrant left hepatic artery in one and extrahepatic collaterals in three patients), and right hepatic arterial flow in two patients (via extrahepatic collaterals). No hepatic arterial flow was seen in the other five patients. None of the 18 patients had underlying stenosis (>50%) of the celiac artery.
All of the four patients with portal vein stenosis, four patients with no hepatic arterial flow on post-embolization angiogram, and one with both had hepatic infarction after hepatic artery embolization, which included lobar infarction in two and subsegmental infarction in seven patients. Right hepatic lobar infarction causing fatal hepatic failure developed in one patient (patient 2) with both portal vein stenosis and no hepatic arterial flow on post-embolization angiogram. Left hepatic lobar infarction combined with abscess requiring percutaneous drainage developed in another patient with no hepatic arterial flow on post-embolization angiogram. Subsegmental infarction developed in three patients with no hepatic arterial flow on post-embolization angiogram and in four patients with portal vein stenosis (one with bilobar hepatic arterial flow via the aberrant left hepatic artery, two with bilobar hepatic arterial flow via extrahepatic collaterals, and one with left hepatic flow via extrahepatic collaterals).
Ischemic liver injuries developed in six (67%) of the other nine patients with hepatic arterial flow on post-embolization angiogram and no portal vein stenosis; these injuries included subsegmental infarction in four patients (one with right hepatic arterial flow via extrahepatic collaterals, two with left hepatic arterial flow via extrahepatic collaterals, and one with bilobar hepatic arterial flow via the aberrant left hepatic artery) and transient hepatic ischemia in two patients (one with right hepatic arterial flow via extrahepatic collaterals and the other with left hepatic arterial flow via the aberrant left hepatic artery). No ischemic liver injuries developed after hepatic artery embolization in three patients with no portal vein stenosis and bilobar hepatic arterial flow via the left hepatic artery aberrantly arising from the left gastric artery or from the common hepatic artery.
Discussion
Based on timing of the bleed, hemorrhagic complications after hepatobiliary pancreatic surgery can be divided into early or delayed (7, 21, 22). Early hemorrhage occurs within the first 48 hours after surgery and requires immediate laparotomy because it is generally caused by technical failure (7, 21). Delayed hemorrhage develops after this time period, mainly occurs from erosion or pseudoaneurysm of major visceral arteries (probably attributed to an anastomotic leakage, localized infection, or intraoperative injury), and most frequently involves the hepatic artery (3–7). Transcatheter arterial embolization has been suggested by many to be the treatment of choice in patients with delayed postoperative arterial hemorrhage, because operative management is difficult due to postoperative adhesion and carries a high mortality and morbidity of up to 90% (4, 9, 10, 21).
Hepatic artery embolization has been considered to be safe and is a widely performed procedure because when hepatic arterial flow is interrupted, the dual blood supply and extensive collateral pathways of the liver can serve to protect this organ from ischemic insults (9–11). A number of collateral pathways to the liver are dissected during hepatobiliary pancreatic surgery, however, and if the arterial bleeding is massive and a hematoma becomes larger, the adjacent portal vein can be compressed with impairment in the portal venous flow. Studies have shown that up to 44% of surgical patients undergoing hepatic artery embolization for postoperative hemorrhage die of hepatic failure (10, 12–16). Thus, hepatic artery embolization in surgical patients with delayed postoperative arterial hemorrhage may place the patient at great risk of ischemic liver injuries.
Hepatic artery embolization can cause ischemic liver injuries, including transient hepatic ischemia/dysfunction, hepatic infarction, liver abscess, and fatal hepatic failure. Previous studies showed that fatal hepatic failure was observed in 0–44% of cases, transient hepatic ischemia/dysfunction in 40–100% of cases, liver abscess in 0–30% of cases, and hepatic infarction in a few cases (10, 12–16, 21). However, we do not think that ischemic liver injuries other than fatal hepatic failure have been fully investigated, because those studies were focused mostly on fatality after hepatic artery embolization and most results were obtained without analysis of cross-sectional imaging studies. For the objective evaluation of ischemic liver injuries, a combination of cross-sectional imaging findings, changes in liver enzyme levels, and clinical outcomes should be analyzed together. Therefore, CT findings as well as changes in liver enzyme levels and clinical outcomes were analyzed in this study. According to our results, ischemic liver injuries were observed in 15 (83%) of 18 patients undergoing hepatic artery embolization for delayed postoperative arterial hemorrhage after hepatobiliary pancreatic surgery. Of the 15 patients with ischemic liver injuries, one patient was found to have a combination of hepatic infarction and abscess, another patient was found to have hepatic infarction causing fatal hepatic failure, 11 patients were found to have hepatic infarction without hepatic failure, and two patients were found to have transient hepatic ischemia/dysfunction. It is interesting that the frequency (72%, 13 of 18 patients) of hepatic infarction in this study is higher than that of previous studies, whereas the frequency (6%, one of 18 patients) of fatal hepatic failure in this study is comparable to that (0–44%) of previous studies (10, 12–16, 21). If CT analysis had not been considered, 11 of our 13 patients with hepatic infarction would have been noted to have transient hepatic ischemia/dysfunction as reported in previous studies (10, 12–16, 21). Thus, we carefully claim that ischemic liver injuries are observed in most patients undergoing hepatic artery embolization for delayed postoperative arterial hemorrhage after hepatobiliary pancreatic surgery, and hepatic infarction, not transient hepatic ischemia/dysfunction, appears to be the most frequent type of ischemic liver injuries encountered in those patients.
Our two patients with lobar infarction either died of hepatic failure or required percutaneous drainage to treat combined gas-forming abscess. All 11 patients with subsegmental infarction were conservatively managed, except one who died of acute heart failure secondary to myocardial infarction. Hashimoto et al. reported a case of fatal hepatic failure that developed in a patient with segmental infarction in the left lateral segment after selective embolization of the left hepatic artery for iatrogenic biliary hemorrhage (23). Thus, it could be claimed that patients with subsegmental infarction might not be associated with unfavorable outcome after hepatic artery embolization. On the other hand, marked elevation (>1000 IU/L) of liver enzyme (AST or ALT) levels, probably representing severe ischemic injury (whether or not it is temporary), was found in four (36%) of 11 patients with subsegmental infarction as well as in two patients with lobar infarction. Despite no cases of fatality in this study, these results might imply that an unfavorable outcome of hepatic failure can develop in a patient with subsegmental infarction after hepatic artery embolization. This can be clarified in a study with a large case series.
It has been suggested that poor development of collateral pathways to the liver and impaired portal venous flow may lead to an unfavorable outcome after hepatic artery embolization in patients with postoperative hemorrhage following hepatobiliary pancreatic surgery, because portal vein stenosis and/or poor development of collateral pathways to the liver was observed in many patients who died of hepatic failure after hepatic artery embolization (12, 13, 15). Michels (24) described 26 possible collateral pathways to the liver in surgical anatomic work based on dissection of 200 cadavers, and Takeuchi et al. (11) revealed that extrahepatic arterial supply to the liver is readily evident in a larger proportion of patients during temporary balloon occlusion of the proper hepatic artery. However, in clinical practice, it is impossible to check all possible arterial collaterals to the liver before and after hepatic artery embolization. Therefore, we regarded no hepatic arterial flow on post-embolization angiogram as representing poor development of collateral pathways to the liver, even though this might not be the case in some patients. In this study, all of the four patients with portal vein stenosis, four patients with no hepatic arterial flow on post-embolization angiogram, and one with both of them had hepatic infarction after hepatic artery embolization. One patient with both portal vein stenosis and no hepatic arterial flow on post-embolization angiogram had lobar infarction and died of hepatic failure 11 days after hepatic artery embolization. The other eight patients with portal vein stenosis or no hepatic arterial flow on post-embolization angiogram had one lobar and seven subsegmental infarctions after hepatic artery embolization. Thus, patients with portal vein stenosis or poor development of collateral pathways to the liver appear to be more vulnerable to ischemic liver injuries after hepatic artery embolization.
It is important to know who will have poor arterial collaterals to the liver after hepatic artery embolization; however, this cannot be predicted before the hepatic artery embolization procedure. In addition, based on our results that six (67%) of nine patients with hepatic arterial flow on post-embolization angiogram and no portal vein stenosis had subsegmental infarction (n = 4) or transient hepatic ischemia/dysfunction (n = 2) after hepatic artery embolization, blood flow via the arterial collaterals could be insufficient to protect ischemic liver injuries after hepatic artery embolization. On the other hand, there is an exception in predicting poor arterial collateralization to the liver after hepatic artery embolization. In patients with an aberrant hepatic artery (i.e. aberrant left hepatic artery from the left gastric artery), it can be expected before embolization that arterial blood flow to at least the part of the liver supplied by the aberrant hepatic artery will be preserved after hepatic artery embolization, and this may induce no or less severe ischemic liver injuries after hepatic artery embolization. All six patients with an aberrant left hepatic artery in this study kept the patency of the aberrant left hepatic artery after proper hepatic artery or common hepatic artery embolization as expected before hepatic artery embolization, and no ischemic liver injuries developed in three (50%) of them. Thus, hepatic artery embolization for postoperative arterial hemorrhage after hepatobiliary pancreatic surgery seems to carry greater risk of ischemic liver injuries if a patient has portal vein stenosis or no aberrant hepatic artery. Endovascular covered stent placement can be an alternative to hepatic artery embolization for those patients, based on previous studies in which endovascular covered stent placement has been suggested as the first-line treatment for postoperative arterial hemorrhage in critical situations where the consequences of superior mesenteric or hepatic artery occlusion may be disastrous (12, 18).
This study has some drawbacks. First, CT scans before and after hepatic artery embolization should be obtained at fixed times to accurately evaluate ischemic liver injuries. However, due to the retrospective nature of this study, CT scans before hepatic artery embolization were not available in nine patients, and the interval between hepatic artery embolization and CT scans after hepatic artery embolization was not fixed. Second, the number of cases is small due to the rarity of hemorrhagic complications. Thus, statistical analysis was not used in this study.
In conclusion, ischemic liver injuries can develop in most patients undergoing hepatic artery embolization for delayed postoperative arterial hemorrhage after hepatobiliary pancreatic surgery. Hepatic infarction, not transient hepatic ischemia/dysfunction, appears to be the most frequent type of ischemic liver injury encountered in those patients. Hepatic artery embolization for postoperative arterial hemorrhage after hepatobiliary pancreatic surgery seems to carry a greater risk of ischemic liver injury if a patient has portal vein stenosis or no aberrant hepatic artery.