
Abstract
Background
Computed tomographic angiography (CTA) has become the primary non-invasive method for detection of cerebral artery aneurysms in many neurovascular centers.
Purpose
To compare MR-angiography at a 3.0 tesla (3T) scanner to CTA in the detection of unruptured intracranial aneurysms.
Material and Methods
CTA and 3T MRA data from 60 patients were evaluated. CTA was obtained with a 4–16-row helical CT-scanner after administration of 120 cc intravenous contrast agent, MRA was performed by a 3T MR-scanner using time-of-flight pulse sequence.
Results
Fifty-five cerebral artery aneurysms were detected by MRA and 47 aneurysms by CTA. Most of the aneurysms detected by MRA but not by CTA were small internal carotid artery (ICA) aneurysms. Bone structures and venous enhancement deteriorated CTA accuracy, especially in skull base. In one patient a fairly large anterior communicating artery aneurysm was not visible in MRA due to spin saturation, although it was clearly visualized in CTA. After contrast injection the aneurysm was also seen in MRA. Although the overall image quality of MRA and CTA were comparable, MRA was more susceptible to artifacts and thus re-formatted surface-shaded volume rendered 3-dimensional images of aneurysms from MRA were inferior compared to those from CTA.
Conclusion
MRA at 3T appears to be at least as sensitive as CTA in the detection of unruptured cerebral artery aneurysms, however image quality control is crucial and contrast agent enhances visualization of complex and large aneurysms.
Computed tomographic angiography (CTA) with multislice helical CT scanners has become the primary diagnostic technique for evaluating cerebral arteries in patients with suspected intracranial aneurysms in many busy neurovascular centers (1, 2). CTA is a rather non-invasive, fast, and safe technique and it has also been reported that with current multislice technology it has sensitivity comparable to that of digital subtraction angiography (DSA) in condition that raw data are adequately analyzed and re-formatted images are constructed in a workstation (1, 3).
As CTA and DSA are the primary methods for evaluating patients with acute subarachnoid hemorrhage (SAH), in many patients CTA is performed due to screening of unruptured aneurysms. It has remained open whether it would be sufficient to evaluate these patients by state-of-the-art magnetic resonance angiography (MRA) which is even less invasive than CTA and does not require the use of ionizing radiation or contrast agent. According to literature, the sensitivity of 1.5T MRA to detect cerebral artery aneurysms has been poorer or equal to that of CTA (4) and less than the sensitivity of DSA (5, 6). An earlier study has shown that 3T TOF MRA has superior image quality (7) and better depiction of cerebral arterial aneurysms (8) than the 1.5T TOF MRA and also, a recent study has shown comparable diagnostic value of 3T TOF MRA and multislice CTA (9).
The purpose of the present study was to compare retrospectively 3T TOF MRA with multislice CTA in the detection of unruptured intracranial arterial aneurysms in clinical practice.
Material and Methods
Patients and MRA
During 2004–2007, all 60 patients in our institution (age range 18–77 years, mean 48.4 years) in whom both 3T high resolution MRA and multislice CTA examinations of cerebral vasculature were available were retrospectively evaluated. Patients had no history of SAH. MRA and CTA were acquired within one year, the reasons for these studies were not only suspicion of aneurysms but also other cerebrovascular diseases such as vasculitis and atherosclerosis. MRA images were acquired at the Advanced Magnetic Imaging (AMI) Center, Helsinki University of Technology with a Signa VH/i 3T MRI scanner (GE Healtcare, Milwaukee, WI, USA) or in our hospital with an Achieva 3T (Philips Medidal Systems, Best, The Netherlands) with a 3-dimensional (3D) TOF sequence without contrast agent. Imaging parameters with the GE Signa scanner were: TE 4.3–4.4 ms, TR 37 ms, flip angle (FA) 25, number of excitations (NEX) 1, field of view (FOV) 160 mm (AP) × 140 mm (RL) × 49.6 mm (FH), matrix 416 × 384, slice thickness 0.8 mm (oblique axial slices). With the Philips Achieva scanner the parameters were: TE 3.5 ms, TR 25 ms, FA 20, NEX 1, FOV 200 mm (AP) × 171 mm (RL) × 90 mm (FH) with matrix 332 × 286 and slice thickness 0.6 mm (sequence 1), or FOV 200 mm (AP) × 170 mm (RL) × 122 mm (FH) with matrix 720 × 310 and slice thickness 1.0 mm (sequence 2), or FOV 200 mm (AP) × 181 mm (RL) × 80 mm (FH) with matrix 496 × 256 and slice thickness 1.0 mm (sequence 3).
With the GE Signa scanner two slabs of 12 min 54 s were obtained in a separate series to cover the whole imaging volume. With the Philips Achieva scanner one series was acquired, the scanning time was 10 min 37 s (sequence 1), 9 min 10 s (sequence 2) or 6 min 26 s (sequence 3). The imaging volume was designed to well include the pericallosal arteries with the origin of callosomarginal branches and the origin of the posterior inferior cerebellar artery (PICA).
CTA
Multislice helical CT scanner with 4-16 detector rows was used for CTA (GE Lightspeed QX/i; GE Healtcare, Milwaukee, WI, USA). The raw images were acquired using 1.25-mm slice thickness, 120 kV, 230 mA, field of view 23 cm, a table speed of 3.75 mm/s, and rotation speed 0.8 s. Total volume of 120 cc of the contrast media (Ultravist 300; Bayer Schering Pharma AG, Berlin, Germany) was injected into the cubital vein using automated injector with injection speed 4 mL/s. Contrast media injection started 18 s prior image acquisitions for patients younger than 60 years old and 20 s for patients older than 60 years old. The imaged region started from the level of first cervical vertebra and continued above the roof of lateral ventricles. From the obtained raw images, the technicians reconstructed thick slab re-format images in axial, coronal, and sagittal planes.
Data analysis
Analysis of the CTA data followed our standard clinical protocol: 3D raw data were processed by at least one experienced neuroradiologist using GE Advantage Windows workstation (version 4.2–4.4) and vendor software to produce 2-dimensional multiprojection image reconstructions on which the diagnostic evaluation of the CTA data was based. For this study the MRA raw data were analyzed by two neuroradiologists following exactly the same protocol as with the CTA data. The final decision of the two neuroradiologists was done in consensus. Analysis of the CTA data was blinded to the analysis of the MRA data and vice versa. For visualization, also 3D volume rendered surface shaded images were constructed.
Results
Voxel sizes for CTA and MRA
The optimized imaging parameters for TOF MRA provided 0.385 mm × 0.367 mm in-plane resolution with 0.8 mm slice thickness (GE Signa), 0.6 mm × 0.6 mm in plane with 0.6 mm slice thickness (Achieva, sequence 1), 0.28 mm × 0.55 mm in plane with 1.0 mm slice thickness (Achieva, sequence 2), or 0.4 mm × 0.7 mm in plane with 1.0 m slice thickness (Achieva, sequence 3). For CTA, in-plane resolution was reported by the CT scanner manufacturer to be 0.45 × 0.45 mm with 0.77 mm resolution in Z-direction.
Detection of cerebral artery aneurysms by MRA and CTA
In 60 patients, 59 cerebral artery aneurysms were detected by MRA or CTA, 55 aneurysms were detected by MRA and 47 aneurysms by CTA. Three aneurysms were fusiform in nature, others were saccular. Table 1 shows summary of the locations of the aneurysms. Re-formatted 2-dimensional images of some aneurysms detected by CTA or MRA are also shown in Figs. 1–3. In 20 patients no aneurysms were detected by MRA or CTA. Two patients had four aneurysms, one patient had three aneurysms, and all the other patients had 1–2 aneurysms. The average diameter of those aneurysms which were detected by both CTA and MRA were in practice equal when measurements based on CTA and MRA were compared: 4.54 mm in CTA and 4.52 mm in MRA (P = 0.85, NS, paired t-test). The average size of MRA positive CTA negative aneurysms was 2.4 mm and the average size of MRA negative CTA positive aneurysms was 3.6 mm.

Re-formatted 2D CTA (a–d) and MRA (e–h) images of four aneurysms from the same patient. CTA (a–d) images are at the top and corresponding MRA images (e–h) at the bottom. Bilateral MCA bifurcation aneurysms (a, b and e, f), posterior communicating artery aneurysm (c and g), and PCA aneurysm at the segment 1–2 (P1–2) level are seen in MRA image (small solid arrow on h). The P1–2 aneurysm is not seen in CTA image due to adjacent vein filled with contrast media (small solid arrow on d)
Summary of cerebral artery aneurysms found in 60 patients by MRA or CTA
Aneurysms detected by MRA, but not by CTA
One internal carotid artery (ICA)/ophthalmic artery aneurysm, which was detected by MRA, was suspected in CTA but was not considered convincing. It was later confirmed by DSA (Fig. 2) and intraoperatively. In addition, there were seven similar MRA positive CTA negative ICA aneurysms which were not confirmed by DSA, their visibility in CTA were deteriorated by masking effect of bone structures or contrast enhancement of cavernous sinus or atherosclerotic vessel wall changes. One such 4.8-mm ophthalmic level ICA aneurysm was retrospectively clearly visible in CTA and was considered clinically significant, others were due to possible extradural origin or small size clinically non-significant. One saccular posterior cerebral artery aneurysm (P1) of 1.5 mm diameter was found in MRA but was not visible in CTA due to overlapping of adjacent vein (Fig. 1), similarly one 1-mm M1 aneurysm was not visible in CTA. There was one MRA positive pericallosal aneurysm, which was considered as a vessel branch origin in CTA and another pericallosal aneurysm which could not even be seen in DSA.
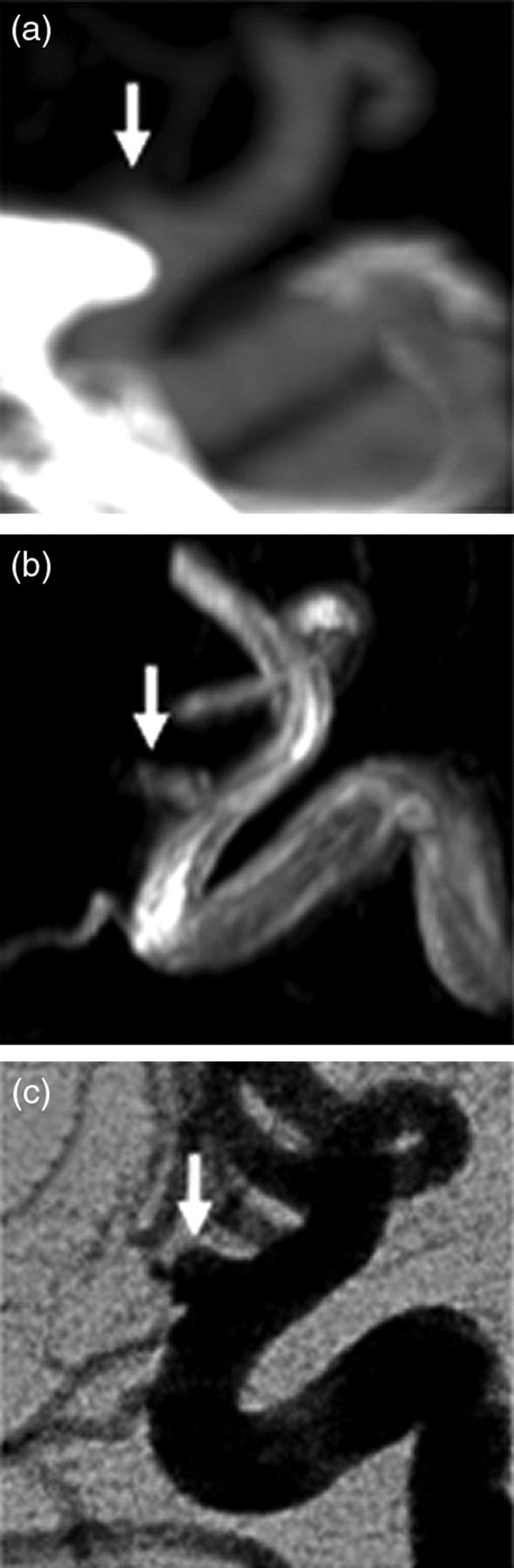
One patient's ophthalmic artery aneurysm on CTA (arrow on a), MRA (arrow on b), and DSA (arrow on c)
Aneurysms detected by CTA, but not by MRA
One 8-mm aneurysm of anterior communicating artery was not visible in routine TOF MRA without contrast agent although it was prominent in CTA (Fig. 3). In this patient also the A2 segments of anterior cerebral artery (ACA) were not well seen in MRA because the patient had also a large ICA bifurcation aneurysm which caused spin saturation. The aneurysm and the vessels were well depicted when gadolinium contrast medium was applied in TOF MRA sequence. In one patient a CTA positive M1 aneurysm was outside the field of view in MRA, in another patient a CTA positive MCA aneurysm was not visible in MRA because of artifacts. One M1 aneurysm in CTA (MRA negative) was considered as a vein loop after MRA examination.
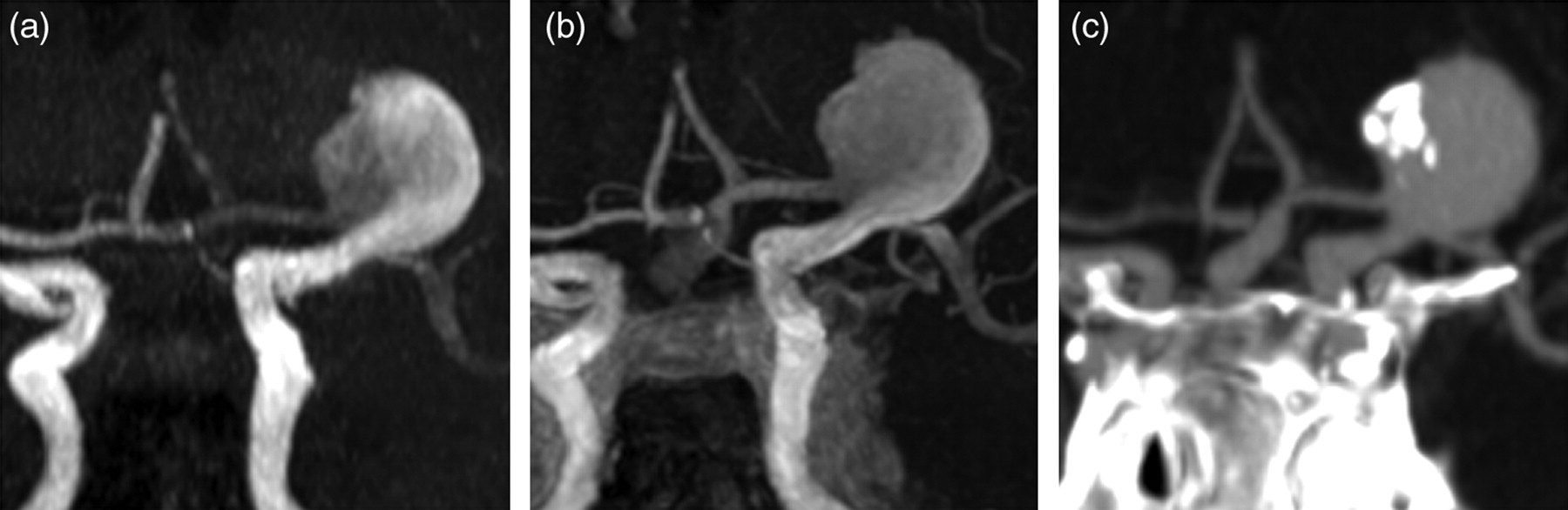
One patient with an anterior communicating artery aneurysm and ICA bifurcation aneurysm. The former is not seen in native TOF MRA (a), but is visible in gadolinium TOF MRA (b), and CTA (c)
Image quality
It is evident in Figs. 1–3 that arterial signal intensity of MRA images is much more heterogeneous than in CTA images. Especially large aneurysms have areas of low signal in MRA. However, all the neuroradiologists considered that the overall diagnostic quality of re-formatted 2D images obtained by MRA was comparable to CTA, and the anatomical details were more clearly seen in MRA than in CTA images. In contrast, re-formatted surface-shaded volume rendered 3D images from CTA, which are important for surgical planning, were superior to 3D images reconstructed from MRA.
Discussion
Our retrospective study compared the detection of unruptured cerebral artery aneurysms by CTA and 3T MRA. In our institution, about 650 CTA examinations of cerebral arteries are performed per year, and careful evaluation of this 3D CTA data in a workstation by an experienced neuroradiologist has become a standard method in search for aneurysms. In our experience DSA examination has very rarely revealed any relevant additional information over CTA in relation to surgical findings as close to 250 aneurysm patients are treated yearly in our neurosurgical unit. As it has been also documented that CTA is accurate enough in detecting cerebral aneurysms versus DSA (1), and the diagnostic value of 3T MRA and 64-channel CTA are comparable (9), our present study further confirms that high resolution 3T MRA is an excellent technique in screening of unruptured aneurysms.
The majority of aneurysms that were detected by MRA but not by CTA, were ICA aneurysms. In CTA bone structures in the skull base may obscure small aneurysms. Unfortunately, we had DSA confirmation for only one ICA aneurysm, so that we can not rule out false-positive findings of MRA. However, infundibular enlargements of the origin of the posterior communicating arteries were ruled out based on anatomical knowledge and location of the MRA positive CTA negative aneurysms. The present study was carried out with the first or second generation multislice CT scanners with anisotropic voxel size. Although novel CT scanners can achieve isotropic and smaller voxel size these improvements still cannot overcome the limitations of CTA at skull base region that would require CTA technique with subtraction.
One cerebral artery aneurysm was detected by MRA but was not visible in CTA because of venous contamination, which means overlapping of contrast agent filled vein over the aneurysm in CTA. In MRA slow venous flow is saturated with TOF technique and MRA shows mainly just arteries and arterial aneurysms. In another patient, a venous structure was considered to be an aneurysm but MRA showed no arterial aneurysm. It has been stated that with the most recent multislice CT technology the venous enhancement in CTA could be minimized (10), because fast image acquisition allows optimized timing so that mainly arteries are filled with contrast. In our experience, there remains some variations based on operator skills and individual differences in patient blood flow dynamics so that venous contamination still exists with even novel CT scanners and imaging protocols.
Saturation of slow moving blood and phase dispersion by complex flow within large aneurysms causes signal loss and large aneurysms are not well visualized in TOF MRA (11). In our series, we showed an interesting case where blood flow inside proximal ICA aneurysm caused spin saturation distally to the aneurysm so, that distal arteries or a distally located anterior communicating artery aneurysm were not visible in TOF MRA images. In gadolinium-enhanced TOF MRA images the distal arteries and the aneurysm were clearly visible. We conclude that on-line image quality control is important to notice possible limitations of TOF MRA technique that can be overcome during imaging sessions by obtaining additional pulse sequences, like gadolinium-enhanced MRA (11, 12), standard anatomic sequences or possibly by phase contrast MRA technique (13). In the follow-up of coiled aneurysms with MRI we routinely have TOF MRA with and without gadolinium. With gadolinium-enhanced MRA slow flow in aneurysm remnants are better visualized. In screening, especially if on-line evaluation of the imaging data is not possible, use of gadolinium routinely should be considered.
Although diagnostic evaluation of CTA and MRA examinations are based on re-formatted 2D images, 3D visualization of aneurysms and related vessel anatomy is essential for surgical or endovascular treatment. With the protocol used in our study the 3D renderings of MRA images did not achieve the quality of CTA images. Often the 3D MRA images were received as good in one viewing direction but there was not enough information to get optimal 3D image in other directions. This problem seemed to be due to non-isotropic voxels in our MRA protocol and the zero-fill interpolation did not help which is quite obvious because interpolation does not create real new sampling points of data. Also, CT gathers information in a more volumetric fashion. If the slab size for MRA is decreased without diminishing the number of slices, a slice thickness comparable to within-plane pixel size would be achieved and thus truly isotropic voxels. Of course the SNR would decrease, but theoretically, this could lead to better 3D visualization of the MRA data.
Due to the retrospective nature of our study we did not have a unique protocol for 3T TOF MRA, nor did we use the latest multislice CT technology. No DSA controls of cases with a mismatch between MRA and CTA were performed. As recently shown, 3T TOF MRA is comparable to 64-channel CTA (9). Our conclusion with regard to the suitability of 3T TOF MRA for screening of cerebral aneurysms remains unchanged. Because the majority of MRA and CTA proven aneurysms showed no clinically significant differences, DSA control examinations of these patients were usually not considered necessary in either group. DSA is an invasive technique and the risks performing DSA seemed not justified, except in one case.
In conclusion, based on our 60-patient study, the sensitivity of 3T TOF MRA exceeds the sensitivity of CTA in screening of unruptured cerebral artery aneurysms. However, image quality during scanning remains crucially important to obtain additional pulse sequences like gadolinium-enhanced TOF MRA in selective cases to detect complex and large aneurysms or abnormal anatomy. Alternatively, gadolinium-enhanced TOF MRA should be added to the protocol routinely.
Footnotes
Acknowledgements
The authors thank radiographer Marita Kattelus for helping in the MRA measurements, Dr Anna Piippo for collecting the patient information, and Professor Riitta Hari for constructive comments on the manuscript.