
Abstract
Background
Magnetic resonance imaging (MRI) has been frequently used to determine a preoperative treatment plan for gynecologic cancers. However, the MR accuracy for staging an endometrial cancer is not satisfactory based on the old FIGO staging system.
Purpose
To evaluate MR accuracy for staging endometrial cancer using the new FIGO staging system.
Material and Methods
Between January 2005 and May 2009, 199 women underwent surgery due to endometrial cancer. In each patient, an endometrial cancer was staged using MR findings based on the old FIGO staging system and then repeated according to the new FIGO staging system for comparison. Histopathologic findings were used as a standard of reference.
Results
The accuracy of MRI in the staging of endometrial carcinoma stage I, II, III, and IV using the old FIGO staging system were 80% (159/199), 89% (178/199), 90% (179/199), and 99% (198/199), respectively, compared to 87% (174/199), 97% (193/199), 90% (179/199), and 99% (198/199), respectively, when using the new FIGO staging criteria. The overall MR accuracy of the old and new staging systems were 51% (101/199) and 81% (161/199), respectively.
Conclusion
MRI has become a more useful tool in the preoperative staging of endometrial cancers using the new FIGO staging system compared to the old one with increased accuracy.
In 1988, the International Federation of Obstetricians and Gynecologists (FIGO) significantly changed the staging system for endometrial cancer by replacing the previous clinical classification with a surgical classification (1). Recently, the FIGO committee recognized that the time had come to revise the staging of endometrial cancer due to the explosive growth of medical research and practice in the field of gynecologic oncology (2). In 2009, the new FIGO staging system was developed by some modifications of the old stage I and II (Tables 1 and 2).
The Old FIGO stage that was revised in 1988
The new FIGO stage that was revised in 2009
Magnetic resonance (MR) imaging is known to be a more accurate modality for preoperative staging of endometrial cancer compared to ultrasound and CT. However, in contrast to promising preliminary results (3–6), recent studies have reported poor sensitivity by using the old FIGO staging criteria in the staging of stage I and II endometrial cancers (7–10). By histopathology examinations as well as MR imaging it is not easy to distinguish between the old stage IA and IB cancers, and the same is true when identifying stage IIA of low grade endometrial cancers (11, 12). The new FIGO stage has two key features different from the old FIGO staging system: One is that the old stage IA and IB is fused into the new stage IA. The second is that the old stage IIA is considered as the new stage I.
There is so far no report about MR accuracy in staging an endometrial cancer using the new FIGO staging system. Therefore, the purpose of our study was to evaluate the accuracy of MRI in staging endometrial cancers according to the new FIGO staging system.
Material and Methods
This retrospective study was approved by our institutional review board and informed consent was waived.
Patients
Between January 2005 and May 2009, using our database, 258 patients (age range 22–82 years, mean age 51.3 years) underwent a radical hysterectomy due to endometrial cancer at our institution. Fifty-nine patients were excluded from our study due to invisible cancer (n = 34) and suboptimal MR images (n = 25). Finally, 199 patients (age range 25–82 years, mean age 52.0 years) were included for data analysis. The pathologic subtypes of the endometrial cancer in these patients included endometrioid carcinomas (n = 176), mucinous adenocarcinoma (n = 9), serous adenocarcinoma (n = 7), clear cell adenocarcinoma (n = 4), squamous cell carcinoma (n = 1), and miscellaneous diseases (n = 2). In 20 of the 199 patients, lesion sizes were less than 1cm on MR images. These endometrial cancers could be staged but sizes could not be measured accurately. Lesion sizes in the other 179 patients had maximum diameters of 1–11 cm (mean 3 ± 1.9 cm). The interval time between MR imaging and surgery ranged from 1–35 days (mean 11 days).
MR imaging
All patients underwent preoperative MRI prior to hysterectomy. MR examinations were performed at 1.5T MR scanner (Signa; GE Healthcare, Milwaukee, WI, USA) in 59 patients or at 3.0T MR scanner (Intera Achiva 3T; Philips Medical System, Best, The Netherlands) in 140 patients. MR imaging was obtained to scan the pelvis initially and then the upper abdomen with an overlap between pelvis and upper abdominal sequences.
Pelvic MR examinations were composed of T2-weighted images, T1-weighted images, and dynamic contrast-enhanced images at 1.5T and 3.0T. The parameters of these MRI sequences were summarized in Table 3.
Parameters for 1.5T and 3.0T pelvis MRI
FSE = fast spin echo; TSE = turbo spin echo; FSPGRE = fast spoiled gradient recalled echo; 3D FFE = three-dimensional fast field echo
The MR scan range of the upper abdomen was located between the lower lung and the aortic bifurcation. These MRI sequences consisted of T2-weighted images and T1-weighed l images at 1.5T and 3.0T. The parameters of these MRI sequences were summarized in Table 4.
Parameters for 1.5T and 3.0T upper abdominal MRI
FSE = fast spin echo; TSE = turbo spin echo; FSPGR = fast spoiled gradient echo; FFGR = fast field gradient echo
Data analysis
Endometrial cancer was first staged using MR findings according to the old FIGO staging system (1), and then according to the new FIGO stage (2). MR staging was not performed with the retrospective review but with using the original report by one of two radiologists who had experienced interpretation of gynecologic MR images for more than five years. At the time of MR interpretation, the radiologists were only aware of a positive cytology for malignancy.
Endometrial cancer was defined as a hypointense lesion on T2-weighted images or a poorly enhancing lesion on contrast-enhanced images (13). Myometrial invasion was defined to be present when the inner myometrium showed loss of distinct low intensity on T2-weighted images or loss of early enhancement on contrast-enhanced images (14). Depth of myometrial invasion was determined by calculating thickness ratios of residual myometrium to adjacent intact myometrium.
Cervical glandular invasion was defined as cancer protrusion into the cervical canal without disruption of the stromal ring (15). Cervical stromal invasion was considered when the stromal ring showed loss of distinct low intensity on T2-weighted images.
A disrupted outer myometrium or the presence of serosal nodules of the uterus, ovary, or salpinx was considered evidence of cancer extension to the outside of the uterus corpus. Vaginal involvement was defined as obliteration of the vaginal fornix. A lymph node with a shortest diameter >1 cm were considered metastatic (16).
Complete disruption of the entire bladder or bowel wall was considered evidence of bladder or bowel invasion. Distant metastasis was defined as hematogenous metastasis to another organs or metastasis to inguinal lymph nodes.
Pathologic reports were used as a standard reference for the MR staging accuracy of endometrial cancer. Pathologic stages were originally classified using the old FIGO staging system and then reclassified using the new FIGO staging system in order to compare MR staging accuracies.
Statistical analysis
MR sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for old and new FIGO stages and compared. A commercially available software program (PASW Statistics, version 17, Chicago, IL, USA) was used for statistical analysis.
Results
According to the old FIGO staging system, pathologically, 143 patients had stage I disease (55 in IA, 73 in IB, and 15 in IC), 26 stage II (17 in IIA and nine in IIB), 27 stage III (seven in IIIA and 20 in IIIB) and three patients had stage IV (three in IVB). MR images showed that 177 patients had stage I disease (49 in IA, 110 in IB, and 18 in IC), seven patients stage II (four in IIA and three in IIB), 13 patients stage III (one in IIIB and 12 in IIIC), and two had stage IV (two in IVB).
According to the new FIGO staging system, pathologically, 160 patients had stage I disease (142 in IA and 18 in IB), nine patients stage II, 27 patients stage III (seven in IIIA, 13 in IIIC1 and seven in IIIC2) and three patients had stage IV (three in IVB). MR images showed that 181 patients had stage I disease (162 in IA and 19 in IB), three patients stage II, 13 patients stage III (one in IIIB, 10 in IIIC1 and two in IIIC2), and two patients had stage IV (two in IVB).
The MR accuracy of the old FIGO stage I was 80% (159/199) (Table 5). The MR accuracy for cancer confined to the endometrium (stage IA) was 77% (153/199) (Fig. 1). The MR accuracy for cancer invading less than half myometrium (stage IB) was 63% (126/199) and that for cancer invading more than half myometrium (stage IC) was 90% (180/199). In contrast, the MR accuracy of the new FIGO stage I was 87% (174/199) (Table 6). The MR accuracy for cancer (stage IA) confined to the endometrium or invading less than half myometrium was 87% (173/199). The MR accuracy for cancer invading more than half myometrium (stage IB) was 90% (180/199).
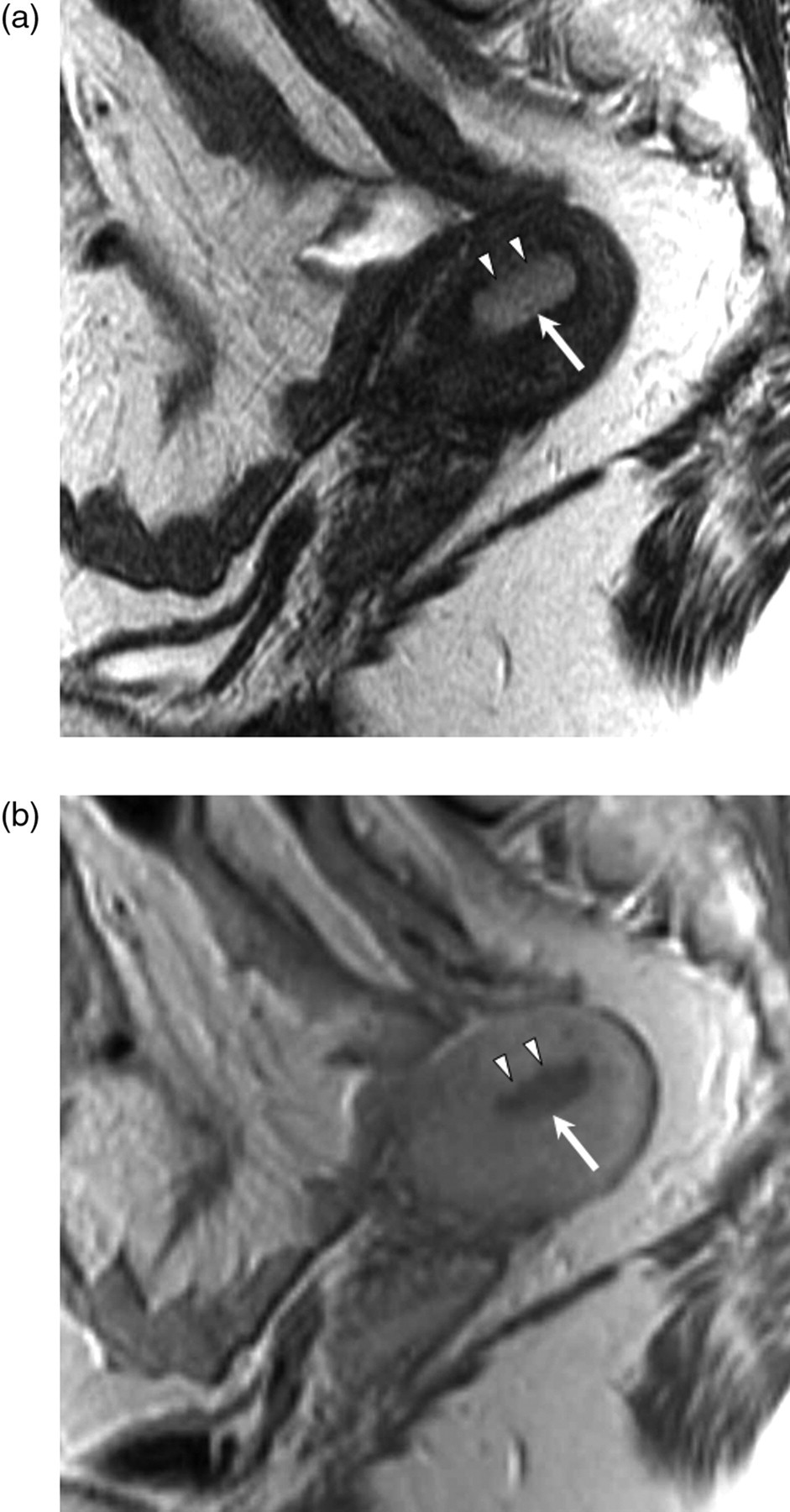
A 53 year-old woman with endometrial cancer. T2-weighted (a) and contrast-enhanced (b) sagittal MR images show a well-defined endometrial cancer (arrow) with an irregular margin (arrows) as if it invaded the superficial myometrium. This lesion corresponds to old FIGO stage IB cancer and new FIGO stage IA cancer. Pathologic examination revealed endometrial cancer confined to the endometrium. Since the endometrium histologically interdigitated with the inner myometrium, the endometrial cancer appeared to invade a superficial myometrium on MR images
MR accuracy for the old FIGO stage
PPV = positive predictive value; NPV = negative predictive value
MR accuracy for the new FIGO stage
PPV = positive predictive value; NPV = negative predictive value
Of the 55 patients who were pathologically confirmed as old FIGO stage IA, 26 (47%) were over-staged as IB (n = 25) or IIA (n = 1) by MRI. Of the 73 patients who were pathologically confirmed as old FIGO stage IB, 15 (21%) were under-staged as IA and three were over-staged as IC (n = 2) or IIIB (n = 1) by MRI. Of the 15 patients who were pathologically confirmed as old FIGO stage IC, seven (47%) were under-staged as IB and one (7%) was over-staged as IIIC. The MR sensitivities for old FIGO stage IA, IB, and IC were 53% (29/55), 75% (55/73), and 47% (7/15), respectively while those for the new FIGO stage IA and IB were 98% (139/142) and 50% (9/18), respectively (Tables 5 and 6). Of the 17 patients who were pathologically confirmed as old FIGO stage IIA, 14 were the new FIGO stage IA and three were stage IB (Figs. 2 and 3).
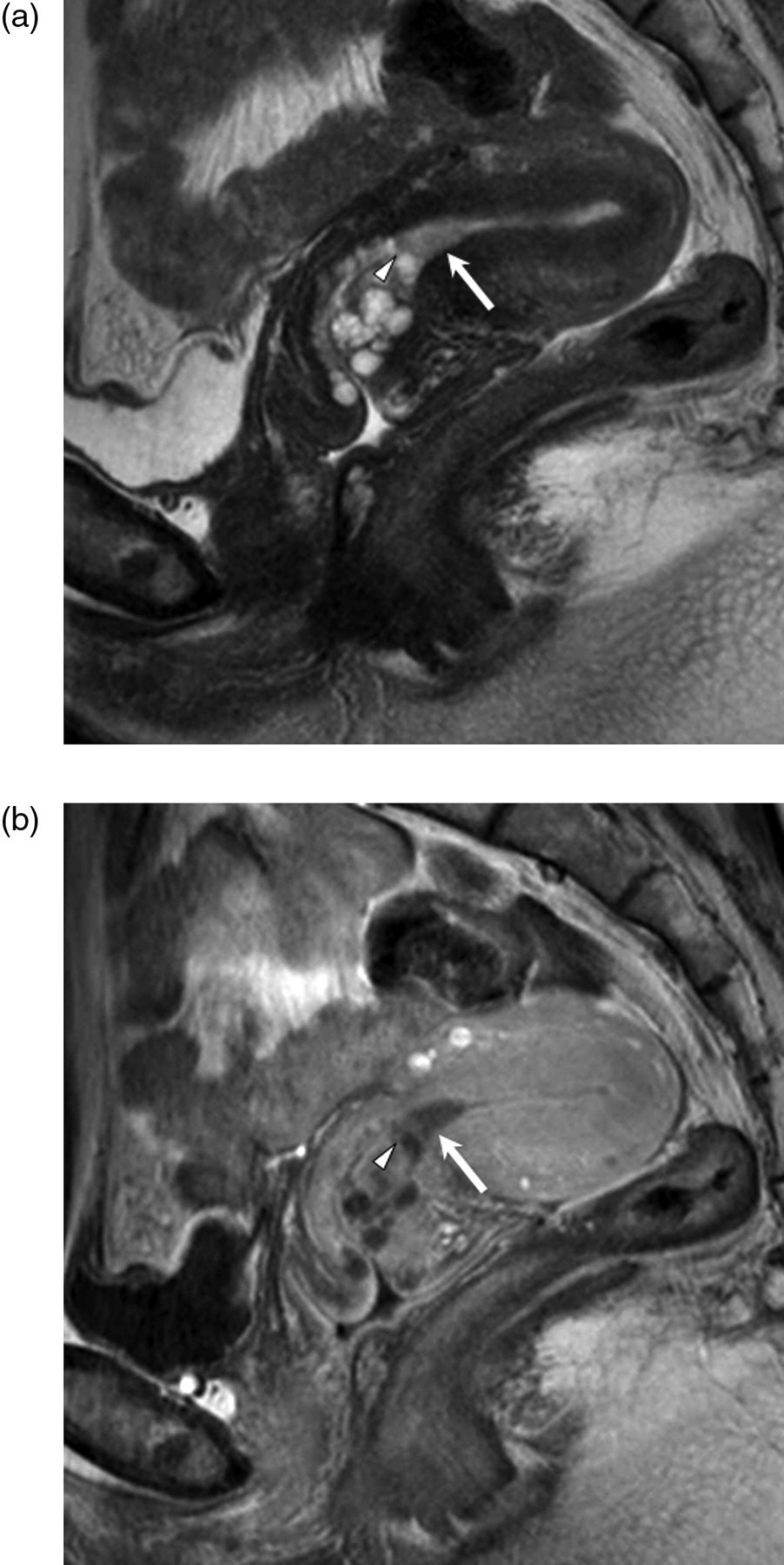
A 46 year-old woman with endometrial cancer. T2-weighted (a) and contrast-enhanced (b) sagittal MR images show a small endometrial cancer (arrow) invading the cervical gland (arrowhead) but the stroma. This lesion corresponds to old FIGO stage IIA cancer and new FIGO stage IA cancer. Pathologic examination revealed that the cancer did not invade cervical stroma but that it did invade the gland
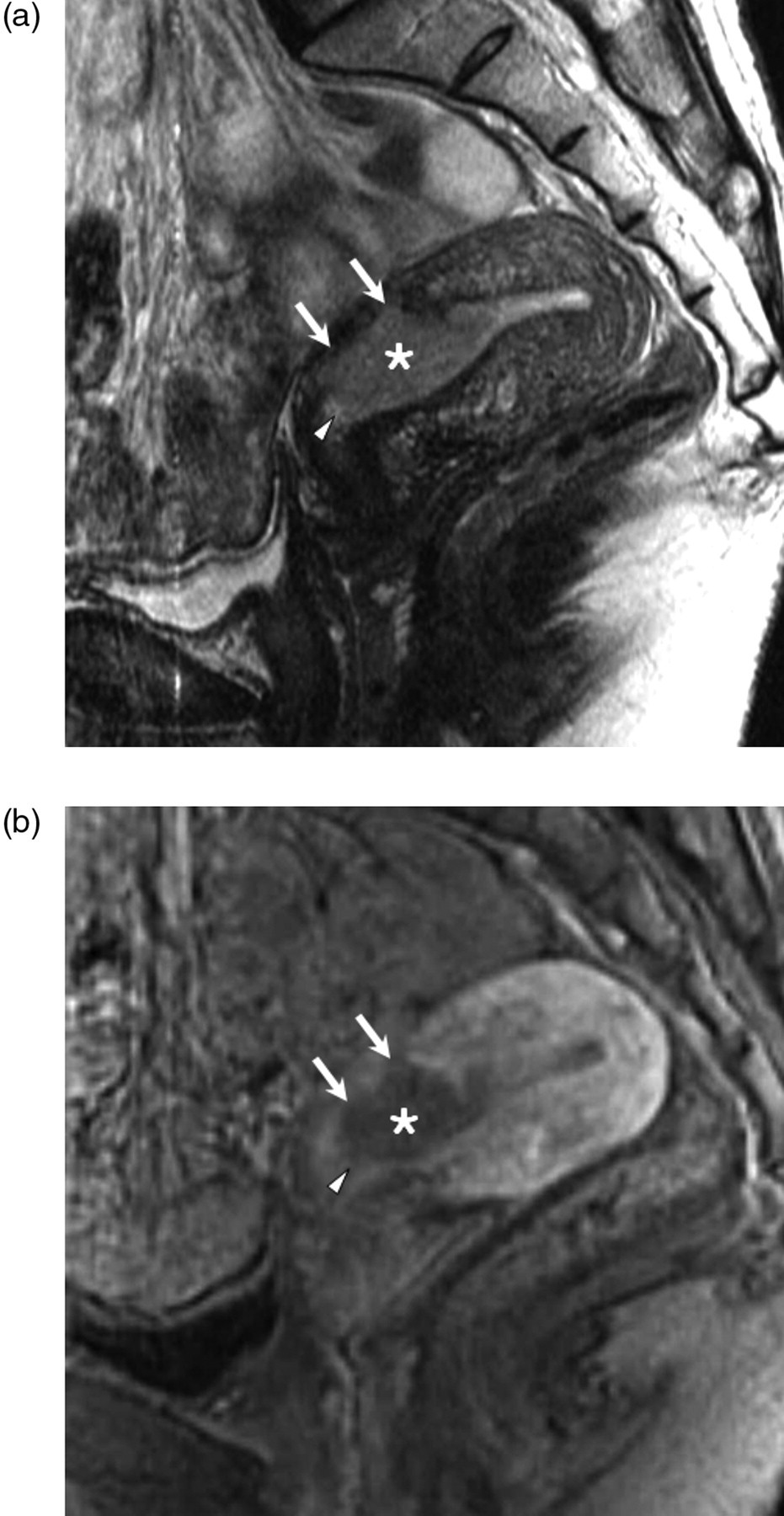
A 34 year-old woman with endometrial cancer. T2-weighted (a) and contrast-enhanced (b) sagittal MR images shows a large endometrial cancer (asterisk) invading the endocervical glands (arrowhead) and deep myometrium (arrows). However, this lesion does not invade cervical stroma. It corresponds to the old FIGO stage IIA cancer and new FIGO stage IB cancer. Pathologic examination revealed the endometrial cancer invaded cervical gland as well as deep myometrium. Histologically, cervical stroma was intact
The MR accuracy for old FIGO stage II was 89% (178/199) (Table 5). The MR accuracy for cancer (stage IIA) involving the cervical gland was 90% (180/199) and that for cancer (stage IIB) involving the cervical stroma was 97% (193/199). However, the MR sensitivities for old FIGO stage IIA and IIB were 6% (1/17) and 33% (3/9), respectively. Of the 17 patients who were confirmed as stage IIA, 16 (94%) were under-staged as IA (n = 4), IB (n = 11), or IC (n = 1) because MRI did not detect microscopic involvement of endocervical glands. In contrast, MR accuracy and sensitivity for new FIGO stage II were 97% (193/199) and 33% (3/9), respectively (Table 6).
The MR accuracy for old FIGO stage III was 90% (179/199) (Table 5). The MR accuracies for old FIGO stage IIIA, IIIB, and IIIC was 96% (192/199), 99% (198/199), and 94% (187/199), respectively. In contrast, the MR accuracy for new FIGO stage III was 90% (179/199) (Table 6). The MR accuracies for new FIGO stage IIIA, IIIB, IIIC1 and IIIC2 were 96% (192/199), 99% (198/199), 94% (188/199), and 97% (194/199), respectively.
The MR accuracies for both old and new FIGO stage IV were 99% (198/199) (Tables 5 and 6). Metastasis was observed in one or more organs: liver (n = 1), inguinal lymph node (n = 1), and omentum (n = 2).
Finally, the overall MR sensitivity and accuracy of the old FIGO staging system were 77% (101/131) and 51% (101/199), respectively, whereas those of new FIGO staging system were 98% (161/165) and 81% (161/199), respectively.
Discussion
Our study showed that the MR staging accuracy of the new FIGO staging system was significantly better than that of the old FIGO staging system in endometrial cancer, despite the small modifications adopted (1, 2). More specifically, stages IA and IB in the old system was fused into stage IA of the new system. In addition, the stage IIA of the old FIGO staging system moved to the new stage I and the stage IIB was renamed stage II in the new FIGO staging system. With these changes in the FIGO staging system, the MR staging accuracy for endometrial cancer improved significantly in our study from 51% to 81%.
The MR sensitivity for cancer limited to the endometrium ranged between 43% and 100% (7, 9, 17–19). In our study, the MR sensitivity was 53% because of over-staging polypoid or full thickness cancers that are limited to the endometrium. Pathologically, old FIGO stage IA is not so easy to diagnose, either. In contrast to the large bowel, where the muscularis mucosa is clearly identified between the mucosa and submucosa, the interface of the endometrium and myometrium is often unclear or irregular. Furthermore, irregular or sinuous interdigitations of the endometrium are frequently encountered (12). Since the neoplastic glands of the tumors confined to the endometrium often replace the endometrial stroma in these endometrial interdigitations, the old FIGO stage IA may be over-staged as IB even by pathologic examination (11, 12). Therefore, the fusion of the old FIGO stage IA and IB may help both radiologists and pathologists to accurately stage endometrial cancer before and after surgery, which explains improvement of preoperative MR staging accuracy of the new FIGO staging system.
Previous studies reported that preoperative MRI showed a good accuracy for predicting the depth of myometrial invasion (3–6, 17). Deep myometrial invasion is associated with a higher probability of pelvic lymph node metastasis, whereas a cancer limited to the endometrium rarely metastasizes to the lymph node (20, 21). Unlike earlier studies which reported that MR sensitivity for deep myometrial invasion ranged from 87–91% (3–6), recent studies reported a range of 36–56% (7–9). Several studies reported that various conditions, such as, fibroid, adenomyosis, polypoid tumor, or the presence of an isointense junctional zone to myometrium, may reduce MR sensitivity for the depth of the myometrial invasion (6, 7, 17). For these reasons, MRI is reported to overestimate the depth of myometrial invasion (6, 7, 22, 23). However, our study had a poor MR sensitivity (47%) for deep myometrial invasion, mainly due to the underestimation of FIGO stage, as was reported previously (17, 19, 24).
In our study, MR sensitivities for old stage IIA and IIB were very low because microscopic involvement of the cervical gland or stroma tissue was not detected. Reports upon the ability of MRI to detect cervical extension are rare. Vasconcelos et al. reported an MR sensitivity for cervical extension of 61% (19/61), but they did not differentiate stage IIA and IIB (10). Pathologically, it is also difficult to diagnose stage IIA in grade I endometrial cancer in the absence of a desmoplastic host response because neoplastic glands are not easily differentiated from the pre-existing or newly-formed glands (12). Furthermore, the prognosis of stage IIA endometrial cancer is almost the same as that of stage I (12). This is why old FIGO stage IIA becomes new FIGO stage I. As a result, MR accuracy for new FIGO stage II is likely to be improved.
Our study has several limitations. First, our study inevitably had a selection bias because it was conducted in a retrospective manner. However, we did not review MR images, but rather relied on MR results obtained preoperatively. Although retrospective evaluations of MR images were made in a blinded manner, radiologists were not completely unaware of clinical or pathological findings because they had encountered at least one or more cases during preoperative or postoperative discussion. Second, the number of stage III or IV cancers was too small to assess the validity of MR staging accuracy. Third, endometrial cancer was staged using 1.5T or 3.0T MR images. Since the diagnostic performances of these two MR scanners for endometrial cancer are not known, the MR accuracy shown in our study lies somewhere between accuracies of these two MR scanners. Finally, endometrial cancer was not evaluated by diffusion-weighted imaging. Several studies reported that this functional MRI was useful for discriminating endometrial cancer from normal endometrium, myometrium, and other benign uterine diseases because of obvious water restriction within cancer tissue (25, 26).
In conclusion, new FIGO stage of endometrial cancer reflect the limitations that MRI or pathologic examination has difficulty differentiating a cancer limited to the endometrium from a cancer invading superficial myometrium and identifying a cancer involving the endocervical gland alone. Therefore, MR accuracy for new FIGO stage I and II endometrial cancers becomes higher than that for old FIGO stage I and II. Preoperative MRI will help determine management and predict the prognosis of endometrial cancer when the new FIGO staging system is used.