
Abstract
Background
Time-of-flight MR angiography (TOF MRA) is currently the most widely used non-invasive imaging tool to diagnose dural arteriovenous fistula (DAVF). It is, however, not as sensitive as invasive digital subtraction angiography (DSA) for detecting the arteriovenous shunting inherent in DAVF. Dynamic contrast-enhanced MR angiography allows separation of arterial and venous phases of contrast passage though the brain and can thus demonstrate early venous filling through the arteriovenous shunt.
Purpose
To compare the diagnostic value of TOF MRA and a commercially available dynamic contrast-enhanced MR angiography sequence (TRICKS) at 1.5T in detecting posterior fossa DAVF.
Material and Methods
We retrospectively collected image data for 19 patients who underwent TOF MRA, TRICKS, and DSA either for primary diagnosis or for follow-up of posterior fossa DAVF and assessed the performance of TOF MRA and TRICKS in demonstrating the arteriovenous shunt, with DSA as the reference standard.
Results
TRICKS detected early arterial filling at 94.4% sensitivity and 83.3% specificity. TOF MRA detected high flow-related signal within venous structures at 64.7% sensitivity and 80% specificity.
Conclusion
The commercially available dynamic MR angiography sequence TRICKS with fully automatic vendor postprocessing at 1.5T is more sensitive than TOF MRA in detecting the arteriovenous shunt in posterior fossa DAVF.
In cases of dural arteriovenous fistula (DAVF), structural brain MRI is typically normal unless there are secondary signs related to cortical venous reflux (1). Time-of-flight MR angiography (TOF MRA) may reveal an increased flow-related signal within venous structures but is relatively insensitive, especially with low-flow shunts (2). As untreated DAVF may cause disturbing symptoms and present a risk for hemorrhage, DAVF suspicion and follow-up have remained some of the few undisputed indications for diagnostic cerebral DSA. DSA, however, being an invasive procedure with risks of serious complications (3, 4), is burdensome for the patient, and necessitates the use of iodinated contrast media and ionizing radiation.
Modified k-space sampling techniques and coil technology development have recently offered dynamic contrast-enhanced MR angiography a temporal resolution able to distinguish arterial, parenchymal, early venous, and late venous phases of contrast bolus passage through the brain (5, 6). This could allow non-invasive detection of the arteriovenous shunt inherent in DAVF. As the presence of cortical venous reflux (CVR) predicts the fistula's clinical behaviour and dictates the aggressiveness of its treatment (7, 8). A non-invasive tool for DAVF assessment should also ideally be able to detect CVR.
Several case reports and small series have produced promising results with dynamic contrast-enhanced MR angiography in the diagnosis and follow-up of posterior fossa DAVF (9–13), high-flow carotico-cavernous fistula (14), and DAVF of the cavernous sinus (15). To date, seven larger series suggest that dynamic contrast-enhanced MR angiography may prove a valuable tool for DAVF diagnosis and follow-up (16–22). Two of these (17, 20). have compared the performance of dynamic MR angiography to that of TOF MRA in the diagnosis of posterior fossa DAVF. Between these studies, however, imaging sequences, temporal resolution, field strength, and the extent of manual postprocessing differ.
We report here our experience with dynamic contrast-enhanced MR angiography at 1.5T for the diagnosis and classification of posterior fossa DAVF and compare its diagnostic value to TOF MRA, with DSA as the reference standard. To the best of our knowledge, our study is the first to investigate this issue with a modern, commercially available MR angiography technique that includes no elaborate postprocessing.
Material and Methods
Patients
The Institutional Review Board approved this retrospective study. We reviewed our institution's digital imaging archives from January 1, 2005 to June 30, 2010 to identify all patients (n = 19, 10 men) who underwent both TRICKS and DSA for evaluation of posterior fossa DAVF, so that the examinations likely represented the same clinical situation (maximum interval between TRICKS and DSA 3 months during which there were no treatments). Of these patients, three underwent the examinations twice and one patient three times during the inclusion period, yielding in total 24 TRICKS + DSA combinations. TOF MRA, likely representing the same clinical situation as DSA (criteria identical to those above), was available for 22 of the 24 TRICKS + DSA combinations, either from our institution or from a referring hospital. Of the 24 TRICKS + DSA combinations, 15 were done for follow-up of a previously treated DAVF, and nine for suspicion of a previously non-diagnosed DAVF.
Conventional angiography
Catheter angiography had been performed for all patients with a dedicated biplane neuroangiography suite (Siemens Axiom Artis; Siemens Medical Solutions, Erlangen, Germany). The DSA examinations included a minimum of two views (frontal and lateral), with selective injections of the appropriate carotid and vertebral arteries with iodinated contrast medium (Hexabrix 320 mgI/mL, Guerbet, Villepinte, France).
Dynamic contrast-enhanced MRA (TRICKS)
All dynamic contrast-enhanced MRA examinations had been performed with a 1.5T MRI scanner (Signa; GE Healthcare, Milwaukee, WI, USA), an 8-channel head coil, and a commercially available sequence ‘time-resolved imaging of contrast kinetics’, TRICKS. The TRICKS sequence segments the k-space into peripheral and central zones and samples the central zone that determines the image contrast more frequently than the peripheral zones that determine the image resolution. Image encoding is done via elliptic centric view ordering to reduce artifacts; a full description of the technique is available in the literature (23, 24).
Imaging parameters for TRICKS acquisition were: TE 1.7 ms, TR 4.8 ms, fractional echo acquisition, slice thickness 10 mm, spacing 5 mm, FOV 24 × 24 cm, true in-plane acquisition matrix 320 × 320, reconstructed matrix 512 × 512, NEX 1, flip angle 40, zero filling in the section dimension, and parallel imaging method with k-space sensitivity encoding (asset factor 2). We set the central k-space sampling rate (equivalent to temporal resolution) at 1.7–1.9 s, depending on coverage requirements. The coil performance of our MRI system did not allow imaging of the whole head at an appropriate temporal resolution. Instead, a neuroradiologist determined the imaging volume individually for all cases to adequately cover the posterior fossa venous structures. 20 mL of gadolinium contrast medium (Dotarem; Guerbet, Villepinte, France) was injected at 1 mL/s with a 2-cylinder MR-compatible injector (Medrad, Warrendale, PA, USA) through a catheter in an antecubital vein, followed by a saline bolus (25 mL, 2 mL/s). Acquisition of 35 successive volumes started simultaneously with the contrast injection. Scan time was approximately 1 min 13 s, including the mask image used for subtraction of the contrast-enhanced volumes.
TOF MRA
TOF MRA imaging had been done in three institutions for five years; during that time, imaging parameters differed between institutions and underwent changes. All TOF MRA images were done at 1.5T with an 8-channel head coil and 3D fast imaging with a steady-state precession sequence with TE 2.6–7.2 ms, TR 23–42 ms, flip angle 20° or 30°, FOV 22 × 22 cm, matrix 512 × 512, slice thickness/spacing 1.4/0.7 mm or 1.6/0.8 mm in all but two cases with slice thickness/spacing of 0.75/0.285 mm.
Image processing and review
Thick-slab maximum intensity projections (MIPs) in the plane of image acquisition were automatically formed from the 3D TRICKS volumes at the MRI consol by vendor software, yielding a 35-frame ‘image loop’ that was sent to the digital image archive. Scrolling through the loop, the reviewer can observe the passage of contrast from early the arterial to late venous phase.
We independently randomized the TRICKS and TOF MRA examinations, removed all patient-identifying information, and transferred the TRICKS image loops and the TOF MRA raw data to a viewing workstation (Advantage Windows workstation; GE Healthcare, Milwaukee, WI, USA) for blinded review by two neuroradiologists (JP and MK, with 5 and 3 years' experience in reading dynamic contrast-enhanced MR-angiograms). The results were obtained by consensus.
For both TRICKS and TOF MRA, the readers recorded the presence or absence of a fistula and CVR. The presence of a fistula was determined by filling of venous structures in the arterial phase of TRICKS, and abnormal flow-related signal within venous structures in TOF MRA. CVR was determined by filling of cortical venous structures in the arterial phase of TRICKS, and abnormal flow-related signal within cortical veins in TOF MRA.
For any fistula, the readers recorded its location by choosing from the following: (a) left lateral transverse sinus or sigmoid sinus near the transverse-sigmoid junction; (b) right lateral transverse sinus or sigmoid sinus near the transverse-sigmoid junction; (c) medial part of left transverse sinus; (d) medial part of right transverse sinus; (e) midline sinus confluence; (f) left jugular foramen region; (g) right jugular foramen region; and (h) tentorial edge. Choosing more than one location was allowable. For TOF MRA data, the readers also determined the presence or absence and location of abnormal vessels that could represent arterial feeders.
After completing the review of TRICKS and TOF MRA data, the two readers reviewed the DSA examinations at a PACS workstation. At this phase, they were allowed to see the DSA referrals and reports but not the corresponding TRICKS or TOF MRA examinations. They determined the presence or absence of a fistula and CVR in the angiograms and the fistula location using the same list of locations as for TRICKS and TOF MRA. Both TRICKS and TOF MRA readings were compared to the DSA readings as the reference standard.
Results
Of the 24 DSA examinations, an open fistula was present in 18. TRICKS was more sensitive than TOF in detecting the open fistulas; Table 1 summarizes the performance of TRICKS and TOF MRA in detecting findings related to the arteriovenous shunt.
Performance of TRICKS and TOF MRA in detecting early filling (TRICKS) or increased flow-related signal (TOF MRA) within venous structures with DSA as the reference standard
CVR was visible in four DSA examinations. TRICKS detected three and TOF MRA one of these; the one CVR missed with TRICKS was also missed with TOF. In one case, TOF MRA failed to show both CVR and the fistulous flow itself: this patient had a non-treated tentorial DAVF draining through the cortical to the deep venous system. Feeder vessels and enlarged veins around the tentorial incisura were, however, visible. TRICKS correctly detected this fistula and its drainage pattern (Fig. 1). Excluding this case, there were no total misses of cortically draining fistulas either with TRICKS or TOF: the fistulous flow itself was detected even if CVR was not.
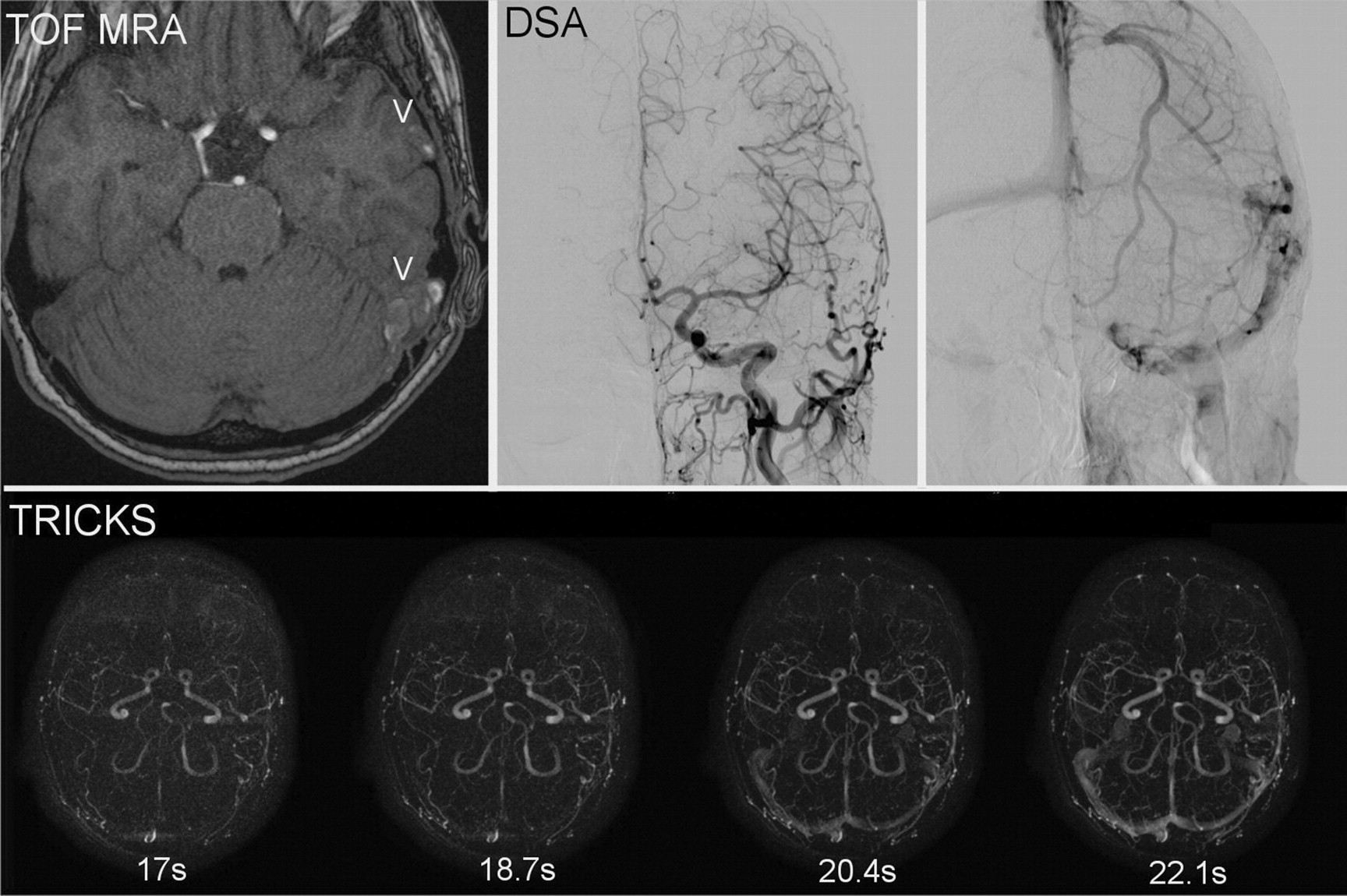
Time-of-flight MR angiography (TOF MRA), digital subtraction angiography (DSA), and dynamic contrast-enhanced MR angiography (TRICKS) images of a patient with headache as a presenting symptom. The patient had no prior diagnosis of a dural AV-fistula (DAVF). TOF MRA (upper left) shows high signal within venous stuctures (V): the left sigmoid sinus and a cortical vein on the left temporal lobe surface, raising a suspicion of DAVF with cortical drainage. TRICKS (lower row) showed no early filling of any venous structures near the left transverse-sigmoid sinus junction: The left sigmoid sinus fills with contrast simultaneously with the right sigmoid sinus at 20.4 s. DSA (upper right) shows prominent external carotid arterial branches near the left transverse-sigmoid junction, but no early-filling veins. Findings are indicative of a spontaneously thrombosed DAVF. The patient reported she had had a pulsating tinnitus that had now ceased. In this case, high signal within venous structures in TOF MRA represented fresh thrombus, and TRICKS agreed with DSA, showing no residual arteriovenous shunting
TRICKS was false-positive for CVR in two cases with an open fistula. TOF was false-positive for both fistulous flow and CVR in one case: This patient had had a spontaneous closure of a cortically draining DAVF where a fresh thrombus with high T1 signal was mistaken for abnormal flow-related signal within venous structures (Fig. 2). In this case, TRICKS findings corresponded to those of DSA.
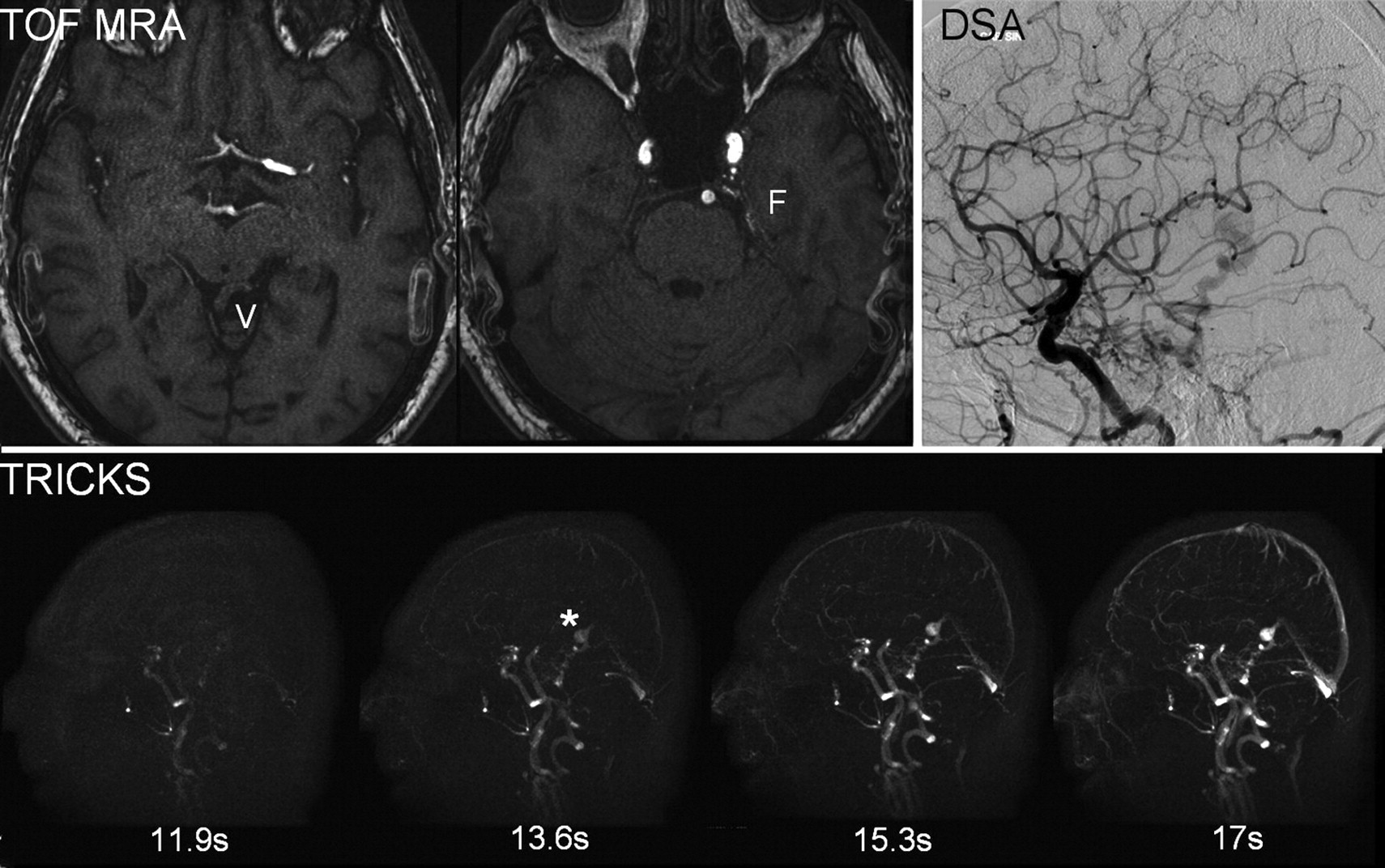
Time-of-flight MR angiography (TOF MRA), digital subtraction angiography (DSA), and dynamic contrast-enhanced MR angiography (TRICKS) images of a patient with a dural AV-fistula (DAVF). Images were obtained during follow-up after treatment. TOF MRA (upper left) shows prominent midline venous structures (V) at the tentorial foramen, and prominent arterial feeders (F) on the left tentorial edge: any high flow-related signal was, however, not visible in any of the venous structures. TRICKS (lower row) shows early filling of midline venous structures draining into the straight sinus. At our temporal resolution (1.7 s), only one or two frames are relevant in each TRICKS series: The ones in which the arteries have just filled but no contrast yet emerges within the normal venous structures. In this case, the early-filling midline venous structures (asterisk) and the straight sinus are faintly visible at 11.9 s (arterial phase for this patient), and they fill with contrast in subsequent frames more intensively and rapidly than does the sagittal sinus. DSA (upper right) shows arteriovenous shunting through the midline venous structures that drained into the straight sinus (straight sinus not shown in this frame). Here, TOF MRA depicted abnormally prominent veins and arterial feeders but failed to show high flow-related signal within venous structures, whereas TRICKS agreed with DSA, showing early venous filling and demonstrating the drainage route
Fistula location was correctly recorded in nine of the 17 correctly positive TRICKS examinations and in eight of the 11 correctly positive TOF examinations. Errors in locating the fistula with TRICKS (n = 8) included: all sinuses filled simultaneously during the arterial phase, making it impossible to define the fistulous point (n = 2); the fistula was thought to be in the medial part of a transverse sinus but was in its lateral part (n = 2); assessment of the location or extensiveness of the fistula near the midline confluence was incorrect (n = 2); the fistula was thought to be in the left foramen jugulare but was in the left tentorial edge (n = 1); and the fistula was thought to be in the left lateral transverse sinus but was in the left foramen jugulare (n =1).
Errors in locating the fistula with TOF MRA (n = 3) included: a fistula thought to be in the left lateral transverse sinus was in the left foramen jugulare (n = 1); and assessment of the location or extensiveness of the fistula near the midline confluence was incorrect (n = 2).
Pathological arterial vessels/feeders were visible in 15 TOF examinations; 14 of these had an open fistula in DSA, and one (a thrombosed fistula) did not. In three cases, feeders were present in TOF images but without abnormal flow signal within the venous structures. In one of these, DSA showed an open fistula; two cases were correctly negative with TOF.
Discussion
Dynamic MR angiography is effective in indicating the arteriovenous shunt of posterior fossa DAVF (9–20). Because dynamic studies require a dose of gadolinium contrast and add to imaging time, it is also relevant to ask whether they provide additional diagnostic value compared to that of TOF MRA. Studies comparing these two methods in the diagnosis of posterior fossa DAVF are, however, few (17, 20).
Our results agree with those of Noguchi et al. (17) and Meckel et al. (20) in showing that dynamic MR angiography is both more sensitive and specific than TOF MRA in detecting posterior fossa DAVF. Our study differs from that of Meckel et al. (20) in one important aspect: intensitivity of postprocessing. They used sophisticated post-processing including free 3D interrogation of the dynamic MRA volumes (20). Our method was considerably more simple and quick, including only serial viewing of the dynamic volumes, each reduced to one 2-dimensional image. Noguchi et al. (17) used a data-viewing approach similar to ours, but their temporal resolution was less (4 s). In the Noguchi group study of 15 open fistulas, two could not be detected with dynamic MR angiography. (17). We had, of 18 open fistulas, one false-negative with TRICKS; the number of cases is too small to compare studies, but it seems reasonable to assume that higher temporal resolution of the currently available techniques offers improved sensitivity in detecting especially low-flow shunts.
Our case with false-negative TRICKS had undergone a partial Onyx embolization on the day before dynamic MR angiography; the residual shunt in his post-embolization DSA was considerably high-flow. In that clinical situation, we considered the negative TRICKS unreliable, and the patient subsequently had radiation therapy, after which the first follow-up DSA showed closure of the shunt. It is in theory possible that the residual shunt had already closed spontaneously during the short time between post-embolization DSA and TRICKS – that is, however, unlikely. With our case of false-positive TRICKS, we had recorded the early arterial filling as ‘very weak’ during the blinded assessment. That patient was on follow-up, and the false-positive finding emerged within the sigmoid sinus contralateral to the location of the cured shunt. In this case, TOF MRA was correctly negative.
TRICKS can be more sensitive than TOF MRA in DAVF assessment because its signal is derived from subtraction of the T1 signal from a background image from serial post-contrast images. It thus avoids two problems inherent in TOF MRA: signal loss due to spin saturation within tortuous vascular structures and the confusing appearance of structures with an inherently high T1 signal such as a fresh intravascular thrombus. Both these problems (false-negative and false-positive with TOF MRA, correct interpretation with TRICKS) emerged in our series (Figs. 1 and 2). Field strength is important for the performance of dynamic MR angiography: Scanning patients at 3T most probably increases dynamic MRA's sensitivity because of the intrinsically higher SNR and increased volume acquisition speed at 3T compared to those at 1.5T (13, 24) Our material suggests, however, that TRICKS imaging is able to detect open fistulas with good sensitivity even at 1.5T, the currently most widely used field strength.
Locating the fistula was less accurate with TRICKS than with TOF MRA, and less accurate in our study than in dynamic MRA in the Meckel (20) and Nishimura (22) group studies. This may be due to the fact that we based our location judgement on thick MIP images over the whole acquisition volume, which offers much less spatial information than does TOF MRA source data or 3-dimensional interrogation of dynamic MR angiography volumes. We believe the same reason to lie behind some of our false-positive CVR findings with TRICKS: normal arterial structures may be mistaken for cortical veins in a thick MIP image. TOF MRA's superior spatial resolution in comparison to that of TRICKS in our series also gave TOF MRA the benefit of being able to demonstrate and locate abnormal arterial feeders. This can enhance its diagnostic accuracy, especially in the case of untreated DAVFs. During follow-up after treatment, prominent feeders may, however, persist for a variable time after shunt closure, so that detecting them is less helpful for diagnosing whether the shunt is still open. We had one primary diagnosis case in which the detection of arterial feeders and abnormally prominent cortical veins would have helped to make the diagnosis with TOF MRA, regardless of the lack of abnormal flow signal within venous structures (Fig. 1).
Based on our own series and the pre-existing studies (9–22), we think that the sensitivity and specificity of TRICKS both justify it as a non-invasive follow-up tool during DAVF treatment. In such clinical use, the relatively insensitive spatial localization of TRICKS with minimal post-processing does not cause a great problem: The prior location of the fistula is already known, and the relevant question is whether or not the shunt is still open. The false-positive CVR rate may cause more confusion because DAVF can evolve from a low to a higher grade; a suspicion of CVR with TRICKS would thus necessitate a check-up DSA. Currently, we use TRICKS in monitoring the response to treatments: For instance, if an open DAVF is visible with TRICKS during radiation treatment, the treatment will continue. We, however, always confirm closing of the shunt with DSA.
The limitations of the study include the retrospective nature, small sample size, lack of assessment of intra- and inter-observer variability, limited number of true-negative cases and selection bias. These restrict our ability to draw exact conclusions on how dynamic MR angiography can reliably exclude DAVF during the primary diagnostic workup. Ideally, prospective studies on non-selected patient populations with symptoms suggestive of DAVF could clarify this important issue. Current clinical practice in diagnosing DAVF, however, varies between institutions, and it is often the case that not all patients with pulsating tinnitus continue to DSA if their structural MRI and TOF MRA are normal. This is because pulsating tinnitus is more common than DAVF and can result from a variety of other vascular and non-vascular causes; the prevalence of DAVF among patients with pulsating tinnitus it is not well known (25). It seems very reasonable to expect TRICKS to detect more DAVF than TOF MRA does, and we have recently added it to our MR imaging protocol for patients with pulsating tinnitus. Based on the accumulating evidence, we believe that structural MRI, TOF MRA and TRICKS can reliably exclude DAVF during primary diagnostic workup and in our institute we do not perform DSA if all these are normal, unless the symptoms are exceptionally suggestive (such as a subjectively audible bruit). Inherent limitations of TRICKS compared to DSA include much less accurate spatial resolution; if DAVF is diagnosed non-invasively, DSA will still always be necessary to delineate its detailed anatomy in order to plan the treatment.
Due to the retrospective nature of our study, the TOF MRA imaging technique differed somewhat between patients imaged in different institutions at different times during the 5-year inclusion period, whereas the TRICKS technique was standard in all cases. It is hard to estimate whether this could have affected our results; the TOF MRA sequences were, however, optimized each time for the specific scanners with which they were acquired.
In conclusion, the commercially available dynamic MR angiography sequence TRICKS with fully automatic vendor postprocessing at 1.5T is more sensitive than is TOF MRA in detecting the arteriovenous shunt in posterior fossa DAVF. Dynamic MR angiography improves the sensitivity of non-invasive imaging in the primary diagnosis and follow-up of DAVF.